




1. Introduction
Hepatitis B virus (HBV) infection is a significant global health issue, affecting approximately 300 million individuals worldwide (1). Chronic HBV infection, characterized by the persistent presence of the hepatitis B surface antigen (HBsAg) for over six months, can lead to long-term complications such as cirrhosis, hepatocellular carcinoma, and liver failure (2). Despite advancements in vaccination and antiviral therapies, HBV remains endemic in many parts of Asia and Africa, with considerable public health implications (3). Healthcare workers (HCWs), particularly those involved in invasive and exposure-prone procedures, face unique challenges when diagnosed with chronic HBV (4). The potential risk of transmission to patients has led to the development of specific guidelines and restrictions to minimize these risks (2). However, the risk of transmission from HBV-positive healthcare workers to patients is low, especially for those with low viral loads and who follow strict infection control practices (4). These case reports highlight the occupational and medical considerations for two HCWs with chronic HBV infection. They explore the balance between patient safety, infection control, and the professional rights of healthcare workers with HBV. The reports also delve into the ethical and medical guidelines for HBV-positive individuals working in healthcare, offering practical insights into the management and surveillance required to ensure a safe work environment.
2. Case Presentation
Two healthcare professionals were referred to the occupational medicine clinic for pre-recruitment health evaluations. Both individuals had chronic hepatitis B and sought employment in clinical settings with potential exposure to biological hazards.
2.1. Case 1
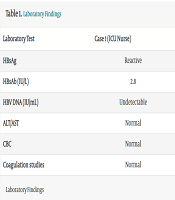
A 35-year-old male ICU nurse with nine years of work experience presented for a pre-employment occupational health evaluation. His occupational exposures included biological hazards (bacteria, viruses, and parasites), ergonomic challenges (prolonged standing, awkward postures, and repetitive tasks), and psychological stressors associated with shift work. The patient was diagnosed with chronic hepatitis B at the age of 18 following an unprotected sexual encounter and was exempted from military service due to his condition. He had no other significant medical history and denied smoking or alcohol consumption. He had no significant past medical history, did not report any known family history of liver disease or hepatitis, and had no notable psychosocial or psychiatric concerns. On physical examination, he appeared in good general health. Laboratory findings revealed a reactive HBsAg, a low hepatitis B surface antibody (HBsAb) level (2.8 IU/L), and an undetectable hepatitis B viral load (HBV DNA). Liver function tests, complete blood count (CBC), and coagulation studies were within normal limits. Routine occupational health evaluations, including optometry, audiometry, spirometry, and electrocardiography (ECG), yielded normal results. He was referred to an infectious disease specialist, who confirmed that he was a healthy carrier of hepatitis B without contraindications to working in a hospital environment.
2.2. Case 2
A 42-year-old female nephrologist presented for a pre-employment medical examination. She had similar occupational exposures to the ICU nurse. She had been diagnosed with chronic hepatitis B at birth due to vertical transmission. She had no underlying chronic conditions, no family history of HBV or liver-related illnesses, and no reported psychosocial or mental health issues. The physical examination was unremarkable. Laboratory tests revealed a reactive HBsAg, a low HBsAb level (1.0 IU/L), and an HBV DNA level of 4,212 IU/mL. Liver function tests, CBC, coagulation studies, and other routine occupational health evaluations were all normal. She was referred to an infectious disease specialist, and antiviral treatment with tenofovir was initiated. A comparative summary of laboratory findings is provided in Table 1.
| Laboratory Test | Case 1 (ICU Nurse) | Case 2 (Nephrologist) |
|---|---|---|
| HBsAg | Reactive | Reactive |
| HBsAb (IU/L) | 2.8 | 1.0 |
| HBV DNA (IU/mL) | Undetectable | 4,212 |
| ALT/AST | Normal | Normal |
| CBC | Normal | Normal |
| Coagulation studies | Normal | Normal |
Laboratory Findings
Based on the occupational medicine assessment and infectious disease recommendations, work suitability was determined under specific conditions:
- Case 1 (ICU nurse): Fit for work with the following precautions:
(1) Use of specialized infection-control gloves during invasive procedures.
(2) Immediate reporting of any high-risk exposure incidents to the hospital’s infection control unit.
(3) Periodic follow-up with an infectious disease specialist and annual viral marker and viral load testing.
- Case 2 (nephrologist): Fit for work with restrictions:
(1) Avoidance of invasive procedures involving internal body spaces.
(2) Immediate reporting of any high-risk exposure incidents to the hospital’s infection control unit.
(3) Continued treatment and follow-up with an infectious disease specialist, with a reassessment in three months.
(4) Periodic viral marker and viral load testing under the supervision of the hospital’s infection control unit.
(5) Re-evaluation by occupational medicine in case of disease progression or complications.
3. Discussion
The management of HCWs with chronic HBV infection involves a nuanced understanding of medical guidelines, occupational risks, and ethical principles. These cases highlight the importance of adhering to evidence-based protocols while balancing the rights and safety of the HCW and their patients.
3.1. Epidemiology and Transmission of Hepatitis B Virus
The HBV infection remains a global health concern, with approximately 300 million people affected worldwide (1). Chronic infection occurs in 10% of cases and is often associated with perinatal transmission (5). Healthcare workers are at heightened risk due to occupational exposure to infected blood and body fluids, especially during invasive procedures classified as exposure-prone (6). Despite these risks, advancements in antiviral therapy and infection control measures have significantly reduced the likelihood of HBV transmission in clinical settings (7).
3.2. Understanding Hepatitis B Virus Markers and Their Clinical Significance
The interpretation of HBV markers is critical in diagnosing and managing infection. Key markers include (3, 8):
(1) The HBsAg (Hepatitis B surface antigen): Indicates active HBV infection, whether acute or chronic.
(2) The HBsAb (Hepatitis B surface antibody): Reflects immunity, either from vaccination or resolved infection.
(3) The HBcAb (Hepatitis B core antibody): Suggests past or ongoing infection; the IgM subtype indicates acute infection, while IgG suggests chronic or resolved infection.
(4) The HBeAg (Hepatitis B e antigen): Signifies active viral replication and high infectivity.
(5) Anti-HBe (Antibody to hepatitis B e antigen): Indicates reduced replication and infectivity.
(6) The HBV DNA: Quantifies viral load and helps assess the risk of transmission.
3.3. Indications for Treatment in Chronic Hepatitis B Virus
Treatment for chronic HBV is indicated based on several clinical and laboratory criteria (9). Key factors include elevated HBV DNA levels, abnormal ALT levels, and evidence of liver inflammation or fibrosis (10, 11). Specifically:
- The HBV DNA > 2,000 IU/mL combined with ALT levels above the upper limit of normal (ULN) and signs of liver damage warrants antiviral therapy.
- Patients with HBV DNA > 20,000 IU/mL and ALT > 2 × ULN should receive treatment regardless of liver inflammation.
- In cases of cirrhosis, whether compensated or decompensated, detectable HBV DNA necessitates treatment, regardless of ALT levels.
3.4. Exposure-Prone Procedures-Definition and Relevance
EPPs are defined as medical or surgical procedures where the healthcare worker’s (HCW’s) gloved hands may come into contact with sharp instruments, needle tips, or sharp tissues within a patient’s open body cavity or confined anatomical space (6). The risk of blood-to-blood exposure is heightened during these procedures, particularly when the HCW's hands or fingertips are not fully visible at all times (7). Examples of EPPs include surgeries, wound treatments, and certain invasive diagnostic procedures (6). Given the potential for HBV transmission during EPPs, strict monitoring of HBV-positive HCWs performing these tasks is crucial. The HCWs with chronic HBV may be restricted from performing EPPs or working in dialysis units under certain conditions (10):
3.4.1. HBeAg Positivity
Indicates high viral replication and infectivity, making participation in EPPs unsafe.
3.4.2. High Viral Load
The HBV DNA levels exceeding 103 IU/mL are associated with a greater risk of transmission and typically warrant restriction.
3.4.3. Failure to Achieve Viral Suppression
In cases where antiviral therapy fails to reduce viral load to < 103 IU/mL after one year of stable treatment, restrictions remain in place.
3.5. Use of Specialized Infection-Control Gloves
High-risk infection control gloves, also known as HBV protection gloves, are essential in healthcare settings for preventing the transmission of blood-borne infections such as Hepatitis B (12). These gloves are typically made from materials like latex, nitrile, or vinyl, which provide a strong barrier against pathogens. Their thickness ensures durability and reduces the risk of tears or punctures, making them particularly effective in high-risk situations. The bright orange color of these gloves serves as an easy identifier, ensuring they are used appropriately. Proper fit is crucial to maintain dexterity and comfort while performing medical tasks. These gloves should be worn during any procedure that involves exposure to blood or bodily fluids and must be disposed of immediately after use to prevent cross-contamination (13). Along with other infection control measures, these gloves play a vital role in protecting both healthcare workers and patients from the spread of infections (14).
3.6. Ethical Implications
Managing healthcare workers with chronic HBV involves balancing patient safety with the rights of the worker (15). Discrimination and stigmatization are significant concerns, as unjustified restrictions can adversely affect the individual’s career and mental health (15).
3.7. Long-Term Monitoring and Management
The chronic nature of HBV necessitates ongoing monitoring to detect disease progression and prevent complications (4). Regular testing for liver function, serological markers, and viral load is critical (3). Annual viral load testing, as recommended for this nurse, ensures early detection of any increase in replication that may necessitate antiviral therapy or additional restrictions (10).
3.8. Conclusion
These cases underscore the importance of personalized, evidence-based management for HCWs with chronic HBV to balance patient safety and workers' rights. Both HCWs presented with chronic HBV, but their clinical statuses differed, influencing the occupational health recommendations made for them. The first patient, an ICU nurse, had undetectable HBV DNA, low HBsAb levels, and normal liver function tests, indicating a low-risk chronic carrier status. This allowed for his eligibility to work in EPPs under specific precautions, such as the use of infection-control gloves during invasive procedures. Regular monitoring was recommended to detect any potential changes in his clinical condition. In contrast, the second patient, a nephrologist, had a detectable HBV DNA level of 4,212 IU/mL, indicating a higher risk of transmission. Consequently, additional precautions, including restriction from high-risk invasive procedures, were implemented, and antiviral therapy with tenofovir was initiated to reduce viral load. The tailored approach in both cases demonstrates the importance of assessing the infectivity levels of HCWs with chronic HBV. By adjusting employment conditions based on clinical status, both patient welfare and professional rights were safeguarded. Ongoing monitoring and follow-up with infectious disease specialists are crucial in ensuring the workers’ health remains stable and that any potential risks to patients are minimized. Incorporating both medical and ethical considerations, this approach allows healthcare institutions to protect public health while maintaining an inclusive environment for HCWs with chronic HBV. By adhering to infection prevention guidelines and making informed decisions based on clinical data, it is possible to optimize workplace accommodations for HCWs and ensure both safe and fair working conditions.
