



1. Background
Mental health concerns among university students have become a significant global public health issue, with a notable increase in the prevalence of stress, anxiety, and depression (1). These mental health challenges are especially pronounced during the transition to university life, a critical period marked by increased academic demands, social pressures, and the need for independence (2). Globally, studies estimate that nearly 20% of university students experience mental health problems (3) that negatively affect their academic performance, relationships, and overall well-being (4).
In Asia, university students face additional pressures due to cultural expectations, intense academic competition, and persistent mental health stigma (4). Research in countries such as China, South Korea, and Japan has shown elevated levels of anxiety and depression among students, partly due to the reluctance to seek professional help for psychological issues (5). This stigma, combined with limited access to support services (6), contributes to a growing mental health burden among student populations in the region (7).
Thailand mirrors these regional trends (1). A 2020 national mental health hotline report revealed that more than one-third of calls from adolescents were related to stress and anxiety, followed by issues with romantic relationships and depression (8). These concerns have been compounded by the COVID-19 pandemic, which intensified feelings of isolation, financial insecurity, and academic disruption — particularly for first-year university students. Additionally, mental health stigma and cultural norms that emphasize emotional restraint may discourage students from expressing distress or seeking help (7). Despite increasing awareness, the availability of mental health professionals and dedicated services in Thai universities remains limited.
While many studies have examined mental health challenges among university students, few have comprehensively assessed the combination of students’ mental health status (9), their knowledge of mental health (10), and the influencing factors such as family (11), institutional (12), and social support (13, 14). Moreover, although awareness of mental health has been shown to influence coping behaviors and help-seeking, little is known about how mental health knowledge interacts with other determinants of well-being in this population, especially in the context of Thai first-year students.
2. Objectives
To address these gaps, this study aims to assess the mental health status and knowledge of mental health among first-year university students in Thailand and to identify factors that influence their mental health. The findings are expected to inform the development of targeted interventions to support students’ psychological resilience and academic success.
3. Methods
3.1. Study Design and Setting
This cross-sectional study was conducted at Suan Sunandha Rajabhat University, located in Bangkok, Thailand. The research took place between October 2023 and March 2024. The study aimed to assess the mental health status, knowledge of mental health, and influencing factors among first-year university students.
3.2. Study Population and Sampling
The target population included all first-year undergraduate students enrolled in the 2023 - 2024 academic year at the College of Allied Health Sciences, Suan Sunandha Rajabhat University. A total of 165 students were enrolled during this period. We used census sampling, a non-probability sampling method in which all eligible individuals are included in the study. Therefore, all 165 first-year students who met the inclusion criteria and provided informed consent were included, representing 100% of the target population. As the entire accessible population was surveyed, no formal sample size calculation was conducted.
3.3. Research Instruments
3.3.1. Demographic Information
Collected data on age, gender, academic discipline, birth order, chronic illnesses, family income, monthly expenses, and financial aid status.
3.3.2. Mental Health Assessment
The Thai Mental Health Indicator (TMHI-15) (15) is a 15-item scale used to measure mental health. Respondents provide their answers using a 5-point scale, where "1 = strongly disagree" and "5 = strongly agree". Total scores can range from 15 to 75, with higher scores indicating better mental health. The scores were divided into three groups: Good (51 - 60 points), fair (44 - 50 points), and poor mental health (43 points or below). The reliability of the questionnaire was assessed using Cronbach’s alpha coefficient. The previous study, which was conducted in Thai, reported a value of 0.89 (16), whereas this study found it to be 0.85.
3.3.3. Mental Health Knowledge Scale
Our research team developed this scale in 2023. Item generation was based on an extensive literature review of mental health literacy frameworks, national mental health guidelines, and existing validated tools assessing mental health knowledge among youth and university students (15, 16). The scale consists of 15 items designed to assess students’ understanding of mental health definitions, causes, symptoms, prevention, and health promotion. Items were rated on a 5-point Likert scale (1 = very low knowledge to 5 = very high knowledge), with total scores ranging from 15 to 75. According to Bloom (17), the mean scores were categorized into three levels: Low (15 - 59), moderate (60 - 79), and high (80 - 100). A higher score indicates a greater level of mental health knowledge. Content validity was assessed using the Content Validity Index (CVI). A panel of three experts in mental health and public health independently evaluated each item for relevance, clarity, and simplicity. Items with a CVI of 0.80 or higher were retained in the final version of the tool. The scale was pilot-tested with 30 first-year students from another university. Reliability testing yielded a Cronbach’s alpha coefficient of 0.88, indicating good internal consistency.
3.3.4. Factors Affecting Mental Health
This 24-item scale was developed by our research team in 2023 based on an extensive literature review of psychosocial determinants of student mental health (1, 4). The scale evaluates three dimensions: Family support, institutional (educational) support, and social support. Responses were recorded using a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Total scores ranged from 24 to 120, with higher scores indicating stronger perceived support. According to Bloom (17), the average scores were classified into three distinct levels: Low (15 - 59), moderate (60 - 79), and high (80 - 100). A higher score signifies a greater number of factors influencing mental health among students. Content validity was established through expert review by three professionals in psychology and mental health education. The items were refined based on their feedback, and the instrument was pilot-tested with a group of 30 university students. The internal reliability was excellent, with a Cronbach’s alpha of 0.90.
3.3.5. Data Collection Procedure
Participants received an invitation via university email and were provided with an online survey link through Google Forms. The survey took approximately 25 - 30 minutes to complete. Participation was voluntary and anonymous. The study protocol was approved by the university’s research ethics committee (Approval No. COA.2-001/2024). Rigorous data quality checks were performed to ensure accuracy and completeness.
3.3.6. Data Analysis
The statistical analysis was performed using SPSS version 26.0. Continuous variables were summarized by reporting the mean and standard deviation (SD), while categorical variables were expressed in terms of frequency and percentage. To investigate the relationships between various influencing factors, mental health levels, and mental health knowledge, multiple regression analysis was utilized to identify predictive factors, with statistical significance defined as a P-value of less than 0.05.
4. Results
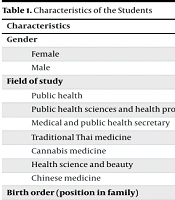
Of the 165 participants, 81.2% were female. The field of study most represented was public health (38.2%), and most students (80%) were 19 years old. Most participants (94.5%) reported no underlying diseases. Nearly one-third of students (30.9%) came from families earning between 15,001 and 20,000 Thai Baht monthly, and 57% had monthly expenses below 10,000 Baht. More than half of the participants (61.2%) reported using student loans to support their studies (Table 1).
| Characteristics | No. (%) |
|---|---|
| Gender | |
| Female | 134 (81.20) |
| Male | 31 (18.80) |
| Field of study | |
| Public health | 63 (38.20) |
| Public health sciences and health promotion | 42 (25.50) |
| Medical and public health secretary | 28 (17.00) |
| Traditional Thai medicine | 17 (10.30) |
| Cannabis medicine | 6 (3.60) |
| Health science and beauty | 4 (2.40) |
| Chinese medicine | 5 (3.00) |
| Birth order (position in family) | |
| First-born | 75 (45.50) |
| Second born | 51 (30.90) |
| Third-born | 21 (12.70) |
| Fourth-born or later | 18 (10.09) |
| Age (y) | |
| < 18 | 17 (10.30) |
| 19 | 132 (80.00) |
| 20 | 10 (6.00) |
| > 21 | 6 (3.60) |
| Underlying diseases | |
| No underlying diseases | 156 (94.50) |
| Heart disease | 1 (0.60) |
| Allergies | 7 (4.20) |
| Panic disorder | 1 (0.60) |
| Family income (per mon, in Thai Baht) | |
| < 15,000 | 37 (22.40) |
| 15,001 - 20,000 | 51 (30.90) |
| 20,001 - 25,000 | 30 (18.20) |
| > 25,000 | 47 (28.50) |
| Monthly expenses | |
| < 10,000 | 94 (57.00) |
| 10,001 - 13,000 | 45 (27.30) |
| 13,001 - 16,000 | 14 (8.50) |
| > 16,001 | 12 (7.30) |
| Student loan usage | |
| No student loan | 64 (38.80) |
| Using student loan | 101 (61.20) |
Characteristics of the Students
Regarding mental health status, 59.4% of students had scores at a good level, 38.2% were at a fair level, and 2.4% were at a poor mental health level (Table 2).
| Score Range | No. (%) | Interpretation |
|---|---|---|
| 51 - 60 | 98 (59.40) | Good |
| 44 - 50 | 63 (38.20) | Fair |
| < 43 | 4 (2.40) | Poor mental health |
Levels of Mental Health of First-Year University Students
Most first-year students (81.2%) exhibited a high level of mental health knowledge. A smaller segment (13.9%) demonstrated a moderate level of knowledge, while only 4.8% showed a low level of knowledge (Table 3).
| Score Range | No. (%) | Interpretation |
|---|---|---|
| 11 - 15 | 134 (81.20) | High |
| 6 - 10 | 23 (13.90) | Moderate |
| 0 - 5 | 8 (4.80) | Low |
Levels of Mental Health Knowledge in Students
In terms of influencing factors, family support received the highest mean score of 4.34 (SD = 0.57), followed by educational support (mean = 4.21, SD = 0.66). Social support received a moderate mean score (mean = 3.46, SD = 0.64), with an overall mean of 3.90 (SD = 0.51) across all domains (Table 4).
| Factors Affecting Mental Health | Mean ± SD | Interpretation |
|---|---|---|
| Family institution | 4.34 ± 0.57 | High |
| Educational institution | 4.21 ± 0.66 | High |
| Social institution | 3.46 ± 0.64 | Moderate |
| Overall | 3.90 ± 0.51 | High |
Levels of Factors Affecting Mental Health in Students
In Table 5, multiple regression analysis identified several significant predictors of mental health. Gender (β = -0.327, P < 0.001), field of study (β = -0.204, P = 0.024), birth order (β = 0.179, P = 0.022), family support (β = 0.248, P = 0.010), educational support (β = 0.225, P = 0.016), and social support (β = -0.210, P = 0.022) were all significantly associated with students’ mental health status. The overall model accounted for 31.5% of the variance in mental health scores (R2 = 0.315, F = 8.796, P < 0.05). Non-significant variables included age, student loan usage, underlying health conditions, family income, monthly expenses, and mental health knowledge.
| Model | Unstandardized Coefficients | Standardized Coefficients | t | P-Value | |
|---|---|---|---|---|---|
| B | SE | Beta | |||
| (Constant) | 32.219 | 4.852 | 6.640 | < 0.001 | |
| Sex (female vs. male b) | -5.353 | 1.389 | -0.327 | -3.852 | < 0.001 |
| Student loan usage (no vs. yes b) | -1.326 | 1.077 | -0.101 | -1.231 | 0.221 |
| Field of study (public health b vs other) c | -2.993 | 1.308 | -0.204 | -2.288 | 0.024 |
| Birth order (1st born b vs. other) d | 2.483 | 1.073 | 0.179 | 2.314 | 0.022 |
| Age | -0.434 | 1.584 | -0.027 | -0.274 | 0.784 |
| Underlying diseases (no b vs. yes) | 0.352 | 6.126 | 0.004 | 0.057 | 0.954 |
| Family income | -0.919 | 1.385 | -0.066 | -0.664 | 0.508 |
| Monthly expenses | 0.365 | 1.171 | 0.025 | 0.312 | 0.756 |
| Mental health knowledge | -0.275 | 0.163 | -0.131 | -1.685 | 0.094 |
| Family support | 3.193 | 1.222 | 0.248 | 2.612 | 0.010 |
| Educational support | 2.162 | 0.885 | 0.225 | 2.442 | 0.016 |
| Social support | -1.808 | 0.779 | -0.210 | -2.321 | 0.022 |
Factors Predicting Mental Health a
5. Discussion
The present study aimed to assess the mental health status and knowledge of mental health among first-year university students and to identify factors influencing their mental well-being. Most students demonstrated above-standard mental health and a high level of mental health knowledge. These findings suggest that while the majority of students are mentally healthy and informed, specific groups remain at risk for mental health challenges.
The regression analysis revealed that female students had significantly lower mental health scores than male students, aligning with existing literature that highlights the greater prevalence of mental health issues (e.g., anxiety and depression) among female students (18). Academic stress, gender-based expectations, and societal pressures may contribute to these outcomes. Similarly, students in public health programs had lower mental health scores, possibly due to the intensive academic demands and emotionally charged course content in health-related fields (19-21).
Birth order has been identified as a significant determinant of mental health, with first-born students exhibiting superior mental health outcomes compared to their later-born peers. This phenomenon may be attributed to the heightened influence of parental expectations on first-borns, along with their propensity to assume more structured familial roles, which may foster enhanced coping mechanisms and resilience (22). Furthermore, it has been observed that first-born students benefit from a greater extent of parental support and possess a more extensive repertoire of experience in managing responsibilities. These factors likely contribute to their comparatively favorable mental health status relative to their later-born siblings (23).
Another important predictor identified was the field of study, with students enrolled in public health programs reporting lower mental health scores compared to their peers in other disciplines. This trend may be linked to the rigorous workload of health-related courses and emotional challenges (24).
Among the support factors, family and educational support were positively associated with better mental health. These findings are consistent with studies suggesting that emotional and practical support from family (11) and academic institutions (12) can buffer students from stress and promote psychological well-being. Interestingly, social support had a negative association with mental health in this study, which may indicate that certain peer or societal pressures could be contributing to student stress rather than alleviating it (13, 25, 26). This finding warrants further investigation.
Although there exists a general high level of mental health knowledge, it does not significantly predict the overall mental health status of individuals. This finding implies that possessing knowledge alone may be inadequate for influencing well-being, particularly in the absence of supportive environments and effective coping strategies.
These results support the need for targeted mental health interventions, particularly for high-risk groups such as female students and those in health-related academic tracks (27). Additionally, strengthening institutional mental health services and family involvement could serve as protective factors for student well-being (28).
5.1. Conclusions
This study examines the mental health status and knowledge of first-year university students in Thailand, identifying key influencing factors. The findings reveal that a majority of students exhibit above-average mental health and a strong understanding of mental health issues. Significant predictors of mental health include gender, academic field, birth order, and levels of family, educational, and social support. These results underscore the importance of implementing targeted mental health promotion strategies within universities. In particular, female students and those enrolled in rigorous programs, such as public health, may require enhanced psychological support. Improving family engagement and bolstering institutional mental health services could further enhance student well-being. Future research should adopt longitudinal and multi-institutional approaches to develop a more comprehensive understanding of student mental health trajectories and inform scalable interventions.
5.2. Implications
The findings of this study offer several important implications for promoting mental health among university students. Firstly, universities should prioritize early mental health screenings and ensure that counseling services are easily accessible, with particular attention given to female students and those enrolled in high-stress academic disciplines like public health. Secondly, educational institutions ought to enhance family engagement initiatives, acknowledging the significant role that family support plays in fostering student well-being. Additionally, universities should assess their existing social support structures to ensure they nurture positive peer relationships rather than inadvertently contributing to stress. Lastly, policy-level interventions should aim to reduce mental health stigma and promote help-seeking behaviors among students.
5.3. Limitations
This study has several limitations that should be acknowledged. Firstly, the cross-sectional design restricts causal interpretations of the relationships between the factors and mental health. Future longitudinal research could offer a clearer insight into the evolution of these relationships over time. Secondly, the findings rely on self-reported measures, which are potentially influenced by social desirability bias. Thirdly, the sample was drawn from a single university, which may restrict the generalizability of the results to other institutions and regions. Expanding the research to include multiple universities in Thailand and across Southeast Asia would provide a more comprehensive understanding of the factors affecting student mental health.
