1. Background
Around 20 million hernia repair surgeries occur worldwide and 5 - 15% of these surgeries happen in the emergency setting (1). The use of mesh in this type of surgery is an indispensable part that constitutes 90% of this type of surgery. The favorable changes in the new type of meshes have made them popular, as they result in less pain and less recurrence rate and reduce visceral or neurovascular injuries (2).
However, the use of the mesh is believed to be related to a higher rate of surgical site infection (SSI) (3). In fact, inguinal hernia surgery in the presence of mesh is defined as dirty wound, while in the absence of mesh is classified as a clean wound (4). Moreover, when foreign bodies are present, the bacterial inoculum required to cause SSI is lower. It is reported that up to 14% of the hernia repairs with mesh may develop SSI (5). Therefore, it has been conventional teaching that synthetic non-absorbable mesh should be used only in clean cases and avoided in case of clean-contaminated or contaminated hernia or dirty cases to minimize the risk of infection and hence recurrence (6).
Most of the isolated organisms from SSI site after inguinal hernia were skin-originated isolates, including Staphylococcus aureus and coagulase-negative staphylococci such as Staphylococcus epidermidis (7). The conditions become more complicated when the isolated species from the surgeon’s glove is similar to skin’s normal flora. Prolonged use of the glove during surgery is also believed to be a risk factor for SSI. Moreover, long-term use of the same glove increases the risk of globe perforation, which is another risk factor for SSI (8). We hypothesized that changing the gloves during hernia surgery may reduce the risk of SSI.
2. Objectives
This study aimed to compare the frequency of SSI between the group that surgeon and his assistants changed the glove and the group in which the gloves remained unchanged.
3. Methods
3.1. Study Population and Design
This prospective observational study was conducted on 200 inguinal hernia cases referred to Imam Reza hospital of Mashhad city in Iran in 2019. All the patients were more than 18 and were elective patients, not emergency strangulation cases. Moreover, all patients underwent open using Lichtenstein’s method along with mesh reconstruction. The included cases were randomly assigned into two groups. The allocation was conducted by a blind person to the study, using sealed envelopes. All of the cases received prophylactic antibiotic therapy.
3.2. Intervention and Outcome Measurement
All participants in the surgery procedure put on two layers of gloves. Just before opening the mesh cover, the involved cases removed the overlying glove and used the underlying glove for mesh insertion. The patients received no antibiotic therapy after the surgery and were discharged two days after the surgery. The cases were advised to visit the clinic ten days and thirty days after the discharge time.
The gathered data included age, gender, surgery duration, the side of hernia, and short-term complications. The patients were examined in order to find clues for SSI. The wounds of those patients who had symptoms of this problem were sampled, and the culture was gathered for wound infection confirmation.
3.3. Ethics
All the patients were provided with written informed consent. The patients were free to discontinue the study whenever they decided to unfollow the course. Moreover, all the steps of this study were in accordance with Helsinki’s declaration and were approved by the Ethics Committee of Mashhad University of Medical Sciences.
3.4. Statistical Analysis
All data were entered in SPSS software version 20. Descriptive data, including frequency, percent, mean and standard deviation (SD) were calculated. The qualitative data were compared between the two study groups using chi-square and Fisher’s exact tests. Moreover, quantitative data were compared between the two groups, using independent sample t-test. P-values less than 0.05 were considered significant.
4. Results
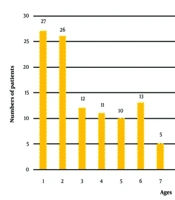
Totally, 200 cases were enrolled in the study, including 102 males (51.0%) and 98 females (49.0%). The mean age of the patients was 42.60 ± 15.79 years ranging from 29 to 55 years old. Past medical history was positive in 100 cases (50.0%), and 98 patients (49.0%) had previous hospitalization history. The mean surgery time was 2.08 ± 0.80 hours and the mean hospitalization period was 1.87 ± 0.84 days. Table 1 shows the details of gender, past medical history, previous hospitalization history, smoking, alcohol abuse, type of prophylactic antibiotic, and surgery side.
Table 2 compares quantitative data between the two study groups, including those who developed an infection and those who had no clue of infection. Also, there was no significant difference between the two groups in terms of age (P = 0.766), surgery (P = 0.531), and hospitalization duration (P = 0.125).
Table 1.
Frequency and Percent of Gender, Past Medical History, Previous Hospitalization History, Smoking, Alcohol Abuse, Type of Prophylactic Antibiotic, and Surgery Side
| Feature | Frequency (%) |
|---|---|
| Gender | |
| Male | 102 (51.0) |
| Female | 98 (49.0) |
| Past medical history | |
| Positive | 100 (50.0) |
| Negative | 94 (47.0) |
| Unknown | 6 (3.0) |
| Previous hospitalization history | |
| Positive | 98 (49.0) |
| Negative | 93 (46.5) |
| Unknown | 9 (4.5) |
| Smoking | |
| Positive | 68 (34.0) |
| Negative | 130 (65.0) |
| Unknown | 2 (1.0) |
| Alcohol abuse | |
| Positive | 12 (6.0) |
| Negative | 185 (92.5) |
| Unknown | 3 (1.5) |
| Type of prophylactic antibiotic | |
| Clindamycin | 75 (37.5) |
| Cefazoline | 58 (29.0) |
| Ceftriaxone | 62 (31.0) |
| Unknown | 5 (2.5) |
| Surgery side | |
| Right | 102 (51.0) |
| Left | 83 (41.5) |
| Bilateral | 13 (6.5) |
| Unknown | 2 (1.0) |
Table 2.
Comparison of Quantitative Data Between the Two Study Groups a
| Feature | Infection | P-Value | |
|---|---|---|---|
| Yes | No | ||
| Age (y) | 42.13 ± 15.14 | 42.84 ± 16.15 | 0.766 |
| Surgery duration (h) | 2.13 ± 0.86 | 2.06 ± 0.77 | 0.531 |
| Hospitalization duration (d) | 1.75 ± 0.78 | 1.94 ± 0.86 | 0.125 |
a Values are expressed as mean ± SD.
The comparison of the qualitative data is summarized in Table 3. There was no significant difference in this regard between those who developed infections and those who did not develop this complication. Especially, infection showed no significant difference between the group that the surgeon changed the glove and the group that remained unchanged.
Table 3.
Comparison of Qualitative Data Between the Two Study Groups
| Feature | Infection | P-Value | |
|---|---|---|---|
| Yes | No | ||
| Gender | 0.342 | ||
| Male | 31 (30.4) | 71 (69.6) | |
| Female | 36 (36.7) | 62 (63.3) | |
| Past medical history | 0.685 | ||
| Positive | 36 (36.0) | 64 (64.0) | |
| Negative | 31 (33.0) | 63 (67.0) | |
| Smoking | 0.997 | ||
| Positive | 23 (33.8) | 45 (66.2) | |
| Negative | 44 (33.8) | 86 (66.2) | |
| Alcohol abuse | > 0.999 | ||
| Positive | 4 (33.3) | 8 (66.7) | |
| Negative | 63 (34.1) | 122 (65.9) | |
| Type of prophylactic antibiotic | 0.363 | ||
| Clindamycin | 29 (38.7) | 46 (61.3) | |
| Cefazoline | 21 (36.2) | 37 (63.8) | |
| Ceftriaxone | 17 (27.4) | 45 (72.6) | |
| Surgery side | 0.541 | ||
| Right | 33 (32.4) | 69 (67.6) | |
| Left | 31 (37.3) | 52 (62.7) | |
| Bilateral | 3 (23.1) | 10 (76.9) | |
| Study group | 0.653 | ||
| Glove changed | 35 (35.0) | 65 (65.0) | |
| Glove unchanged | 32 (32.0) | 68 (68.0) | |
5. Discussion
Although in cases with strangulation, intestine-derived pathogens are the main reason for SSI after inguinal hernia surgery, SSI usually happens by skin-derived pathogens in elective cases (9, 10). In fact, 2.4% of elective inguinal hernia cases surgeries may be complicated with SSI, which is comparable with SSI rate of 4.1% in emergency surgeries (11, 12). With this regard, many efforts have been made to minimize the risk of SSI after inguinal repair.
One of the prerequisites in case of lowering the rate of infection is believed to be prophylactic antibiotic therapy. Several clinical trials assessing the use of preoperative antibiotics in groin and incisional hernia repair have supported their use (13). However, a published meta-analysis reported no significant difference in cases with infections between those who administrated prophylactic antimicrobial therapy and those without this provision (14).
Another part of the problem that deals with SSI is the use of prosthetic meshes. Although meshes reduce the risk of hernia recurrence, they provide a surface for opportunistic pathogens to form a biofilm (2, 15). Many efforts have been made to provide materials that lower the rate of SSI, such as silver and chlorhexidine-impregnated products or recently proposed polypropylene meshes. However, some studies proposed that there is no superiority of these materials compared to the conventional materials (16-18).
The pathophysiology of SSI in inguinal hernia repair is not clearly known; however, in case of non-emergent cases, it is believed that contamination of the wound with epidermal microbiota plays a substantial role. With this regard, it is advised to prevent the contact of the mesh with patient’s skin. Moreover, it is proposed that changing the gloves before mesh insertion reduces the risk of SSI in this type of surgery (12). However, no proved evidence in this regard is proposed, and the role of glove changing in SSI reduction remained a hypothesis. Our results showed no statistically significant difference regarding the rate of infection between the group that the surgeon changed his glove and the group that had their glove unchanged.
Long duration of surgery is another possible risk factor for infection. Long-time surgery makes the surgeon tiered and is associated with higher risk of inadvertent contamination. Moreover, the risk of glove perforation increases as the surgery takes time (8, 19). However, we found no significant difference in case of mean surgery time between those who developed infection and those who had no infection. It is reported that an operation time of more than two hours is especially responsible for glove perforation, and most gloves last around two hours (20). The mean surgery time in our study was not more than two hours, and the lack of significance may be partly due to this.
Altogether, the present study was the first in its case and should be weighed in comparison to other studies. We tried to fulfill all the possible limitations. The study had random allocation, and the surgeon, researcher, patient, and those who conducted statistical analysis were blind to the allocation. Moreover, SSI is a multifactorial disorder, and all the possible risk factors should be considered, as we tried to do so. However, there were some missing data in our study that partly influenced our results.
5.1. Conclusions
Our study could not show any benefit for glove changing in reducing SSI after inguinal hernia surgery. Moreover, the time of the surgery was not important in this regard, according to our results. However, this is the first report and the result should be completed with further studies in the future.