1. Background
Primary biliary cirrhosis (PBC) is a chronic cholestatic autoimmune disease of unknown etiology that mainly targets cholangiocytes of interlobular bile ducts. It primarily affects middle-aged women between the 5th and 6th decade, with a female/male ratio of 10:1. The disease has a slowly progressive course towards liver cirrhosis and death with a strong individual variability of progression rate. Currently, Ursodeoxycholic Acid (UDCA) is the only drug specifically approved for the treatment of PBC (1).
Incidence of PBC is extremely variable, ranging from 0.7 per million to a maximum average of 49 per million per year registered in Olmsted County, Minnesota (2). It seems that prevalence and incidence of the disease is increasing worldwide (3); this finding may be influenced by an increased exposure to potential environmental triggers or simply may be the result of a greater awareness of the disease amongst physicians.
Even if the pathogenesis of the disease is still unclear, it most likely results from a combination of genetic factors and superimposed environmental triggers. The role of genetic susceptibility is clear, as demonstrated by a 100-fold higher risk of developing PBC in relatives and a 60% concordance in monozygotic twins (4). Furthermore, a weak susceptibility conferred by the DRB1*08 allele of the human leukocyte antigen (HLA) class II (5) and a protective effect related to HLA DRB1*11 and DRB1*13 alleles have been demonstrated in Italian and UK series (6, 7). More interestingly, several components of an innate and adaptive immune system have been shown to play a critical role in establishing a greater susceptibility to PBC, as clearly stated by recent genome-wide association studies (GWAS) (8-12). Finally, a possible role of environmental triggers, such as infectious agents, xenobiotics, reproductive hormone replacement therapy and cigarette smoking, has been advocated, even if none of them has been definitively confirmed (13-16).
Few population-based studies on epidemiology and natural history of PBC have been conducted (17-21) and only three (19-21) of them are in the past decade. In particular, very few data exists on patients from the Mediterranean area, whose genetic background and risk factors might differ from those of other populations of Northern Europe and of Northern Italians (22).
In addition, there is no current data regarding a potential association between the clinical course of PBC and Interleukin (IL) 28B polymorphisms, whose rs12979860 CC and rs8099917 TT genotypes strongly predict the spontaneous clearance of HCV infection and the sustained virologic response after antiviral therapy in patients with chronic hepatitis C (23). Recently, our group has shown a link between IL28B polymorphisms and severity of liver disease in terms of both necroinflammatory activity and fibrosis in 160 patients suffering from non-alcoholic steatohepatitis (24). Although IL-28 is involved in immune defense against viruses, it also plays a role in the adaptive immune response, as its inclusion as an immunoadjuvant during animals vaccination leads to augmented antigen-specific Interferon Gamma (IFN-γ) release as well as an increased cytotoxic potential in CD8+ T cells (25, 26).
2. Objectives
The aim of our study was to perform a cohort study to describe genetic susceptibility and clinical course of PBC in patients from Southern Italy. In addition, a subgroup analysis was carried out to assess the potential impact of IL28B polymorphisms on the clinical expression of the disease.
3. Methods
3.1. Patients
This study was carried out on a sample of 81 consecutive patients with PBC who were recruited at the gastroenterology and liver unit of Azienda Ospedaliera Policlinico Universitario P. Giaccone of Palermo, Italy, from January 2001. Patients were included if they had a diagnosis of PBC according to the American association for the study of liver diseases (AASLD) guidelines (27), based on the presence of two out of three of the following criterias: (i) biochemical evidence of cholestasis with elevation of alkaline phosphatase activity; (ii) presence of anti-mithocondrial autoantibodies (AMA) positivity with titer ≥ 1: 40; (iii) histopathologic evidence of non-suppurative cholangitis and destruction of small or medium-sized bile ducts.
Histological staging, available in 77 patients, was performed according to Scheuer’s classification. Four patients did not undergo liver biopsy because of advanced age.
The exclusion criterias were: (i) other causes of liver disease or mixed etiologies, including overlap syndromes; (ii) significant alcohol consumption, i.e. superior to 21 alcohol units per week in men and 7 - 14 alcohol units per week in women (28), evaluated by interview (iii) HIV infection; (iiii) geographical origin outside Mediterranean area (Figure 1).

Figure 1.
Flowchart of Enrollment
Clinical and biochemical data was collected at the time of the diagnosis and then every 6 months. The diagnosis of extrahepatic autoimmune diseases was made on clinical grounds following the diagnostic criteria commonly used for each single rheumatologic condition, without any grading/staging of the diseases. The presence of symptoms was assessed by interview. Patients with PBC-related symptoms (itching, jaundice, fatigue) or with symptoms ascribable to the autoimmune diseases associated with PBC (xerostomia, xerophthalmia, joint pain) were defined as symptomatic.
3.2. HLA Class II Genotyping
In a subgroup of PBC patients (n = 31), normally distributed for age, clinical presentation and histological stage, DNA typing of HLA class II alleles of Major Histocompatibility Complex (MHC) was performed using the MicroSSP DNA Typing trays by One Lambda (Canoga Park CA, USA). Firstly, the DNA was extracted from 200 μL of whole peripheral blood using the PureLink Genomic DNA Kit (Invitrogen by Life technologies) according to the manufacturer’s instructions. Secondly, DNA genotyping was performed by a single polymerase chain reaction (PCR) sequence specific primer (SSP) in accordance with the protocol, which was provided by the manufacturers (One Lambda, Canoga Park CA, USA). This method permits to discriminate each allelic difference overtaking the problem of possible ambiguous results linked to the cross-reagent group, typical of serological typing. The PCR products were separated on 2% agarose gel containing ethidium bromide and visualized under ultraviolet light. HLA class II DRB1 alleles were also genotyped in a control group of healthy subjects (n = 237) with the same method (MicroSSP DNA typing trays by one lambda). These patients belonged to the same population in terms of geographic distribution. Moreover, the selected subjects grandparents were all born in the Western part of Sicily. For this control group we used the entire reference of the healthy blood donor population.
3.3. IL28B Genotyping
IL28B genotyping for rs12979860 and rs8099917 polymorphisms was carried out in a subgroup of patients (n = 32). DNA was purified from whole-blood patient samples using the QIAmp DNA blood mini kit (Qiagen, Mainz, Germany). DNA samples were quantified using the Quant-iT™ PicoGreen® dsDNA Assay Kit (Invitrogen, Pasley, UK) and stored at 20°C. Genotyping for rs12979860 and rs8099917 was carried out using the TaqMan SNP genotyping allelic discrimination method (Applied Biosystems, Foster City, CA, USA). A commercial genotyping assay was available for the rs8099917 (cat. C_11710096_10), while a custom assay was created by AB for rs12979860.
3.4. Follow-Up and Treatment
A liver ultrasound was performed at the diagnosis and then annually in pre-cirrhotic patients as well as every 6 months in cirrhotic patients. Later, an esophagogastroduodenoscopy was performed every 1 - 3 years. Furthermore, patients with medium to large esophageal varices underwent primary prophylaxis of variceal bleeding according to the BAVENO V guidelines (29).
All patients were treated with UDCA (average dose: 15 mg/kg/day). In absence of the biochemical response to UDCA, as defined by the Barcelona or Paris criteria (30), either budesonide, fenofibrate or colchicine were added to UDCA.
Out of 81 patients, eight were lost during the follow-up. The other 73 patients were followed up for a period of at least one year. Disease progression was defined as the development of one or more of the following complications: esophageal varices, ascites, sonographic signs of portal hypertension, portosystemic encephalopathy, hepatocellular carcinoma (HCC), orthotopic liver transplantation (OLT) and death.
3.5. Ethical Approval
This study was performed in accordance with the principles of the declaration of Helsinki and its appendices as well as with the local and national laws. Approval was obtained from the hospital’s internal review board and the ethical committee, as well as written informed consent from all patients.
3.6. Statistical Analysis
Continuous variables were summarized as mean ± standard deviation and categorical variables as frequency and percentage. Mann-Whitney or χ2 tests were used as appropriate to compare continuous or categorical variables.
All patients were divided into groups, according to presence or absence of extrahepatic autoimmune disease and then to presence or absence of AMA positivity, in order to analyze statistically significant differences in terms of clinical presentation and laboratory tests. In addition, they were divided in three age groups (< 45 years, 45 - 65 years, > 65 years) in order to perform a similar comparison.
Typing of HLA class II DRB1 alleles, performed in 31 PBC patients, was compared with that of 237 healthy control subjects. The relative risk was calculated using Fischer’s test and Bonferroni correction method. After IL28B genotyping for rs12979860 and rs8099917 polymorphisms (n = 32), clinical, laboratory and histological features as well as disease progression of CC vs. non-CC rs12979860 and TT vs. non-TT rs8099917 patients were compared.
A Cox regression analysis was performed to identify the presence of independent predictors of clinical progression. A multivariate analysis including all the significant baseline variables (P < 0.05) was also conducted using a binary logistic regression.
All statistical analysis were performed using a SPSS v. 20.0 for Macintosh (SPSS Inc., Chicago, USA).
4. Results
4.1. Baseline Features
Baseline demographic, laboratory, clinic, histologic and genetic characteristics of 81 patients with PBC are summarized in Table 1. The mean age was 53.2 years (range 31 - 84), with a strong predominance of female sex (96.3%). Fourteen patients (17.3%) were diagnosed over the age of 65 years. Median gamma-glutamyl transpeptidase (GGT) values were five times the upper limit of normal (X u.l.n.) and those of alkaline phosphatase (AP) 3 X u.l.n. Median values of aspartate and alanine transferase (AST and ALT) were slightly higher than normal, even if 24 patients (24.6%) had values more than 2 X u.l.n. The median value of total cholesterol was 213 mg/dL with an interquartile range between 199 and 244 mg/dL.
Table 1.
Baseline Demographic, Laboratory, Clinic, Histologic Characteristics of 81 Patients with Primary Biliary Cirrhosisa
| Characteristics | |
|---|---|
| Age - years, mean ± SD (range) | 53.2 ± 12.2 (31 - 84) |
| Female gender | 78 (96.3) |
| Antimitocondrial Antibodies (AMA) | 71 (87.7) |
| Antinuclear Antibodies (ANA) | 31 (38.3) |
| Smooth Muscle Antibodies (SMA) | 6 (7.4) |
| γ-Glutamyl Transpeptidase (IU/L), median (I.Q.I.) | 164 (83 - 322) |
| Alkaline Phosphatase (IU/L), median (I.Q.I.) | 297 (160 - 425) |
| Aspartate Aminotransferase (IU/L), median (I.Q.I.) | 41 (33 - 70) |
| Alanine Aminotransferase (IU/L), median (I.Q.I.) | 48 (34 - 80) |
| Total Bilirubin (mg/dL), mean ± SD | 0.76 ± 0.7 |
| Platelets (x103/mmc), mean ± SD | 242 ± 84.5 |
| Symptomatics | 54 (66.7) |
| Pruritus | 42 (51.6) |
| Fatigue | 13 (16.1) |
| Xerostomia | 13 (16.1) |
| Xerophtalmia | 11 (13.6) |
| Arthralgias | 3 (3.7) |
| Right upper abdominal quadrant discomfort | 3 (3.7) |
| Extrahepatic autoimmune diseases | 33 (40.7) |
| Sjogren’s Syndrome | 22 (27.2) |
| Autoimmune Thyroiditis | 7 (8.6) |
| Rheumatoid arthritis | 3 (3.7) |
| Seronegative Spondyloarthritis | 1 (1.2) |
| Liver Histology (n = 77) | |
| Stage I | 15 (19.5) |
| Stage II | 40 (51.9) |
| Early (I - II) | 55 (71.4) |
| Stage III | 13 (16.9) |
| Stage IV | 9 (11.7) |
| Advanced (III - IV) | 22 (28.6) |
aValues are expressed as No. (%) unless otherwise indicated.
Seventy-one out of eighty-one (87.7%) patients showed AMA positivity with titer ≥ 1:40, while ten were AMA negative. Amongst these, seven (12.3%) showed antinuclear autoantibodies (ANA) positivity with titer ≥ 1:80, two ANA and smooth muscle antibodies (SMA) positivity and one SMA positivity only. Comparing PBC AMA-positive and PBC AMA-negative cases, no significant differences regarding age and laboratory features at onset were found (data not shown).
Liver biopsy was performed in 77 out of 81 patients. Amongst these, 71.4% presented an early histological stage (Scheuer stage I and II) and 28.6% an advanced stage (Scheuer stage III and IV).
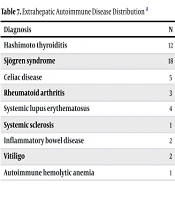
Two thirds of patients were symptomatic at the time of diagnosis. Most common symptoms were: pruritus (51.6%), asthenia (16.1%), xerostomia (16.1%), xerophthalmia (13.6%), arthralgia (3.7%) and right upper abdominal quadrant discomfort (3.7%). Thirty-three (40.7%) patients had extrahepatic autoimmune diseases associated with PBC. Amongst these, the most frequent one was Sjogren’s syndrome (27.2%). No significant differences were found on the clinical presentation and laboratory tests between patients with and without extrahepatic autoimmune diseases.
The comparison of the three groups of patients that were distributed according to age (< 45 years, n = 24, 45-65 years, n = 43, > 65 years, n = 14) showed that subjects younger than 45 years had higher ALT (P = 0.038) and AP levels (P = 0.047) than older cases (Table 2).
Table 2.
Comparison Between Groups of Age (< 45 Years, n = 24; 45 - 65 Years, n = 43; > 65 years, n = 14) on Laboratory Characteristics at Onset: Univariate Analysis
| Variable | < 45 years, (n = 24) | 45 - 65 years, (n = 43) | > 65 years, (n = 14) | P |
|---|---|---|---|---|
| ALT (IU/L), median (I.Q.I.) | 62 (47 - 99) | 44 (32 - 71) | 33 (22 - 71) | 0.038 |
| ALT (x u.l.n.), median (range) | 2xN (1.1 - 8.4) | 1.5xN (0.3 - 8.5) | 1xN (0.71 - 4.6) | |
| AP (IU/L), median (I.Q.I.) | 411 (247 - 563) | 296 (115 - 408) | 165 (93 - 271) | 0.047 |
| AP (x u.l.n.), median (range) | 4xN (1.4 - 21) | 3xN (0.5 - 9) | 1.5xN (0.4 - 4.4) |
Abbreviations: ALT, Alanine aminotransferase; AP, Alkaline phosphatase.
4.2. Subgroup Analysis for IL28B Polymorphisms
Aiming to better define the genetic profile of our Mediterranean PBC cohort and considering the pivotal role of IL28B polymorphisms in modulating inflammatory response and progression of liver disease in different clinical settings, we decided to test a small number of PBC patients for IL28B polymorphisms.
Baseline demographic, clinic, laboratory and histological features as well as IL28B rs12979860 and rs8099917 polymorphisms frequency of 32 PBC patients are shown in Table 3. In comparison to non-CC rs12979860 (n = 16), CC rs12979860 genotype (n = 16) was associated with early histological stage (93.8% vs. 62.5%, P = 0.03) and higher mean ALT levels (71 ± 64 vs. 50 ± 25, P = 0.05) at univariate analysis. No statistically significant differences were found comparing non-TT rs8099917 patients with TT rs8099917 ones.
Table 3.
Univariate Analysis on Demographic, Laboratory, Clinical and Histological Characteristics at Onset Between PBC Patients With CC rs12979860 (n = 16) vs. non-CC rs12979860 (n = 16) Interleukin-28B Polymorphism
| Variable | CC rs12979860 (n = 16) | Non-CC rs12979860 (n = 16) | P |
|---|---|---|---|
| Age - years, mean ± SD | 54 ± 10 | 52 ± 14 | n.s. |
| Total Bilirubin (mg/dL), mean ± SD | 0.6 ± 0.24 | 0.53 ± 0.29 | n.s. |
| Alanine aminotransferase (IU/L), mean ± SD | 71 ± 64 | 50 ± 25 | 0.05 |
| γ-Glutamyl Transpeptidase (IU/L), mean ± SD | 188 ± 125 | 199 ± 173 | n.s. |
| Alkaline Phosphatase (IU/L), mean ± SD | 281 ± 222 | 295 ± 171 | n.s. |
| Platelets (x103/mmc), mean ± SD | 266 ± 64 | 233 ± 95 | n.s. |
| Symptomatics, No. (%) | 6 (37.5) | 10 (62.5) | n.s |
| Extrahepatic autoimmune diseases, No. (%) | 8 (50) | 8 (50) | n.s |
| Liver Histology, No. (%) | 0.03 | ||
| Early (I - II) | 15 (93.8) | 10 (62.5) | |
| Advanced (III - IV) | 1 (6.7) | 6 (37.5) |
4.3. Subgroup Analysis for HLA Class II Typing
HLA-DRB1 allele frequencies of 31 PBC patients are reported in Table 4. Compared to healthy controls (n = 237), we found a higher frequency of HLA-DRB1 * 07 (39.2% vs. 11.4%, RR 5.03) and HLA-DRB1 * 08 (10.7% vs. 0, RR n.c.).
Table 4.
Typing of HLA Class II Alleles of Major Histocompatibility Complex (MHC) in PBC Patients Compared to a Control Group of Healthy Subjectsa
| DRB1 Alleles | PBC (n = 28) | Controls (n = 237) | R. R. | P | P* |
|---|---|---|---|---|---|
| HLA DRB1*07 | 11 (39.2) | 27 (11.4) | 5.03 | 0.00007 | 0.0008 |
| HLA DRB1*08 | 3 (10.7) | 0 | n.s. | 0.00004 | 0.0005 |
| HLA DRB1*14 | 5 (17.8) | 16 (6.7) | 3.0 | 0.02 | n.s. |
| HLA DRB1*11 | 4 (14.2) | 87 (36.7) | 0.28 | 0.04 | n.s. |
| HLA DRB1*13 | 6 (21.4) | 24 (10.1) | n.s. | n.s. | |
| HLA DRB1*15 | 2 (7.1) | 63 (26.5) | 0.21 | 0.02 | n.s. |
aValues are expressed as No. (%).
4.4. Analysis of Follow-up
Amongst the 73 patients in follow-up (mean duration 61 months), three died (two because of cardiovascular disease and one because of end-stage liver disease) and one underwent liver transplantation. Overall, 16 (21.9%) patients had progression of a disease (Table 5).
Table 5.
Events Leading to Disease Progression in 16 out of 73 PBC Patient (Mean Follow-Up 61 Months)a
| Event (Disease Progression: n = 16) | N = 73 |
|---|---|
| US signs of portal hypertension | 20 (27.4) |
| Esophageal varices | 11 (15.1) |
| Ascites | 3 (4.1) |
| Hepatic encephalopathy | 2 (2.7) |
| Jaundice (bilirubin >5 mg/dL) | 2 (2.7) |
| Liver transplantation | 1 (1.4) |
| Death | 3 (4.1) |
| Hepatocellular carcinoma | 0 |
aValues are expressed as No. (%).
The rate of progression of disease was equal amongst patients with AMA positivity or AMA negativity. Furthermore, 81.3% of patients with disease progression had medium/intense itching during follow-up and amongst all patients with medium or intense itching, 48.1% had disease progression as compared to 6.5% without pruritus. Five years after diagnosis, 13% of patients with initial histological stage and 49% of patients with advanced histological stage showed sonographic signs of portal hypertension, whereas 8% of patients with initial histological stage and 27% with advanced histological stage developed esophageal varices (Figure 2). Notably, no patient developed hepatocellular carcinoma.
 in PBC Patients with Early Stage (Solid Line) and Advanced Stage (Broken Line); P = 0.026 by Log-Rank Test")
Figure 2.
Event-Free Survival (Portal Hypertension) in PBC Patients with Early Stage (Solid Line) and Advanced Stage (Broken Line); P = 0.026 by Log-Rank Test
The only independent risk factors associated with disease progression for the multivariate analysis was, the presence of extrahepatic autoimmune disease (P = 0.049, RR 2.96), pruritus for more than one year (P = 0.008, RR 3.84) and advanced histological stage (P < 0.001, RR 8.31) (Table 6).
Table 6.
Multivariate Analysis of Risk Factors Associated With Disease Progression in 73 Patients with Primary Biliary Cirrhosis by Logistic Regression Analysis
| Covariates | β | S.E. | O.R. (95% CI) | P |
|---|---|---|---|---|
| Extrahepatic autoimmune diseases | 1.086 | 0.553 | 2.96 (1.007 - 8.711) | 0.049 |
| Persistence of pruritus > 1 year | 1.346 | 0.509 | 3.84 (1.424 - 10.379) | 0.008 |
| Advanced (III - IV) histological stage | 2.117 | 0.554 | 8.31 (2.823 - 24.471) | 0.0001 |
5. Discussion
Primary biliary cirrhosis, as well as other autoimmune diseases are more common in Caucasian populations. Nevertheless, few European studies exist on epidemiology and disease course of PBC and most of them are derived from Northern European cohorts (3). In addition, natural history of PBC is incompletely characterized in patients of the Mediterranean area whose genetic background and risk factors might differ from those of Northern Europeans.
Our patients showed demographic, clinical and biochemical features at onset, which was very similar to those described in other population-based cohorts. In particular, patients with AMA-negative PBC have a comparable presentation and progression of the disease compared to AMA-positive subjects, as already stated by several evidences (1). A more severe cytolytic pattern was observed at onset in younger patients compared with older ones, a trend that was already emphasized by Muratori et al. (31). Interestingly, the most common symptom in our cohort was pruritus, which was complained in a sporadic or constant way in about half of the patients at diagnosis, while fatigue was less reported (16% of patients). These two symptoms have been related to an impairment of the quality of life with potential serious repercussions (32, 33). In a study by Prince et al. (34), the prevalence of fatigue at diagnosis was similar to that reported in our cohort (21%) but itching was present at diagnosis in only 18.9% of patients, a smaller proportion compared with our findings.
The rate of progression of PBC is extremely variable (1). In our cohort, presence of pruritus for more than one year, an advanced histological stage at diagnosis and the presence of extrahepatic autoimmune disease were found to be independently associated with disease progression. With regards to the first, several authors already reported that symptomatic patients at diagnosis have a shorter survival rate compared with asymptomatic subjects (35, 36). It is interesting that among all the symptoms only itching was associated with progression of the disease. The presence of an advanced histological stage is recognizably associated with a greater rate of progression, due to the fact that it is representative of a disease, which was already advanced at diagnosis in most of the cases. Lastly, the association of other autoimmune diseases, with a less favourable prognosis, had already been suggested by several lines of evidence (36). Nonetheless, the association of PBC with other autoimmune diseases further confirms the immune pathogenesis of the disease. In our cohort, 33 (40.7%) out of 81 patients showed an association with extrahepatic autoimmune diseases. Amongst these, the most frequent one was Sjogren’s syndrome (27.2%). This finding confirms its high prevalence in patients with PBC, as reported by recent studies (37, 38).
Interestingly, the median value of the total cholesterol was quite high in comparison to that of the healthy population. A recent systematic review (39) showed that cholesterol levels are increased in about 50% of patients with PBC. Essentially, 75% of the patients in our series had a total cholesterol value greater than the normal values (> 200 mg/dL). Even if the risk of mortality from cardiovascular disease is not increased in patients with PBC, despite the presence of hypercholesterolemia (40), we reported two deaths for cardiovascular events during follow-up.
Typing of HLA class II alleles of MHC in a subgroup of patients (n = 31) and its comparison with a control group of healthy subjects (n = 237) showed a higher frequency of HLA-DRB1 * 07 and HLA-DRB1 * 08 in PBC. In contrast to other series from Northern Europe (5), we also reported a higher prevalence of a DRB1 * 08 allele of HLA class II, respect to DRB1 * 07. This difference may reflect a different genetic background of patients from the Mediterranean area as compared to those of Northern Europe.
One of the most interesting findings arising from our cohort lies in the statistically significant association between CC IL28B rs12979860 genotype, early histological stage and higher mean ALT values. To our knowledge, this is the first study assessing the potential association between IL28B polymorphisms and the severity of liver damage in PBC patients. Our original result is consistent with the identification of an independent association between the presence of IL28B CC homozygosis, the genotype associated with a good response to antiviral therapy in patients with chronic hepatitis C (41), and the severity of inflammation at early stages in patients with PBC. In this line, growing evidences demonstrated that IL28B rs12979860 polymorphism strongly affects the histological severity of chronic liver diseases, in terms of both necroinflammation and fibrosis progression, independently of the underlying etiology (24, 41-43). By contrast, we did not find any association with IL28B rs12979917 polymorphism. However, it should be noted that our data is not consistent enough to evaluate whether patients with PBC have a higher prevalence of IL28B rs12979860 CC genotype compared to the Mediterranean general population, due to the lack of data in this setting. Of note, we can only observe that the frequency (about 50%) of IL28B rs12979860 CC genotype in our PBC cohort is higher compared with that reported (about 30%) in Sicilian patients with chronic hepatitis C (44) and similar to that observed (46%) in a homogeneous cohort of 301 Sicilian patients with thalassemia major (45).
Evidently, the main and biggest limitation of our study lies in the small simple size of our cohort and the fact that the genetic analysis was performed on a fraction of patients only. In addition, data regarding the progression of the disease is mainly limited to development of portal hypertension, an aspect likely due to the small number of reported events. However, although all of the above data needs further validation in larger studies, they might identify a subgroup of PBC patients at a higher risk of disease severity and progression deserving a more rigorous follow-up. Furthermore, these high-risk patients may be the ideal candidates who could benefit from possible future experimental treatments of chronic liver diseases focused on liver regeneration, including the use of endogenous hepatocytes, fetal hepatic stem cells, bone marrow-derived stem cells and embryonic stem cells and induced pluripotent stem cells (46).
In conclusion, our prospective cohort study provides further insights in the natural history and overall genetic background of Mediterranean patients with PBC. At disease onset, a more severe biochemical activity was observed in younger patients, while the presence of rs12979860 CC genotype was associated with a milder histological stage. Persistence of pruritus and presence of extrahepatic autoimmune liver disease were significantly associated with a poorer prognosis. Taken altogether, these findings might be useful to identify subgroups of PBC patients at different risks of disease severity and progression. However, larger studies are needed in this setting to elaborate novel follow-up protocols or treatment strategies for such patients.