1. Background
Substance use disorder (SUD) is associated with a wide range of physical, psychological, and social health problems (1). It has increasingly become a public health concern because of its adverse effects on social, occupational, and legal functioning. Despite the expansion of treatment programs, sustaining treatment engagement remains challenging, and limited treatment eagerness has been linked to poorer outcomes (1).
Limited treatment eagerness is a common challenge in SUD treatment and has been associated with higher relapse rates during periods of abstinence (2). It is considered a key barrier to initiating and maintaining treatment. Treatment eagerness refers to an individual’s willingness and readiness to change and engage in the therapeutic process (3). Previous research has linked individual, family, social, and economic factors to treatment eagerness and relapse (4). Better family functioning has also been associated with greater treatment eagerness and treatment engagement (5).
Perceived social support has been associated with greater treatment engagement and treatment eagerness among individuals with SUD (6). Several studies have also reported that lower perceived social support is associated with a higher probability of relapse and lower treatment eagerness (7).
Psychological symptoms have been associated with treatment eagerness and engagement in individuals with SUD. Various symptoms, including physical pain, craving-related difficulties, aggression, obsessive symptoms, depression, and sensation seeking, have been linked to relapse risk (8). Depressive symptoms reported during treatment have been associated with lower vitality, diminished treatment eagerness, and hopelessness, whereas physical pain has been linked to a greater tendency to use substances to relieve discomfort (9). Furthermore, anxiety and stress have been associated with an elevated risk of relapse, particularly when individuals encounter stressful situations without adequate coping strategies (10).
In this context, substance use is often described as a maladaptive emotion regulation strategy. Such strategies, including rumination, worry, and emotional suppression, have been associated with temporary relief of emotional distress but poorer long-term emotional adjustment (11). Evidence also suggests that limited access to effective emotion regulation strategies is linked to greater impulsivity, difficulties with cognitive inhibition, and emotional instability, which may be associated with lower adherence to treatment goals and reduced treatment eagerness. In contrast, stronger emotion regulation skills have been reported to be associated with lower substance craving and greater treatment eagerness (12).
Although these variables have been examined separately, limited evidence is available regarding their combined associations with treatment eagerness among individuals with SUD. Therefore, the present study aimed to investigate the relationships between these variables and treatment eagerness among patients diagnosed with SUD in Zahedan, Iran, in 2025.
2. Objectives
This study aimed to examine the relationships among family functioning, perceived social support, psychological symptoms, and difficulties in emotion regulation, and treatment eagerness among patients with SUD in Zahedan, Iran, in 2025.
3. Methods
3.1. Study Design and Ethics
This applied study employed a cross-sectional descriptive-correlational design. The study protocol was reviewed and approved by the Ethics Committee of Islamic Azad University, Zahedan Branch (Ethics ID: IR.IAU.ZAH.REC.1404.050).
3.2. Participants and Sampling
The statistical population comprised all men with SUD residing in medium-term residential treatment centers in Zahedan, Iran, in 2025. According to information obtained from the Welfare Organization of Sistan and Baluchestan Province, 14 medium-term residential substance use treatment centers for men were active in Zahedan at the time of the study, with approximately 420 residents in total. Based on the study inclusion and exclusion criteria and the centers’ willingness to cooperate, four centers were introduced by the Welfare Organization and selected for participation. Each selected center had approximately 30 residents.
The minimum sample size was determined using Green’s (1991) second rule of thumb for regression models: N = 104 + m
where m represents the number of predictor variables. Given the four predictor variables in the present study, the minimum required sample size was calculated as 108 participants. In total, 120 questionnaires were distributed.
A two-stage sampling method was used. In the first stage, participants were selected purposively based on the study inclusion and exclusion criteria. In the second stage, questionnaires were distributed using convenience sampling.
A total of 120 questionnaire packages were prepared. Two eligible individuals declined participation and did not provide written informed consent. Therefore, 118 questionnaires were distributed. After excluding 6 incomplete questionnaires, data from 114 participants were included in the final analysis.
The inclusion criteria were as follows: 1) age 20 - 45 years, 2) minimum literacy, defined as the ability to read and write, and 3) residence in the treatment center for at least 1 week. The exclusion criteria were unwillingness to participate and a current diagnosis of schizophrenia spectrum disorders.
3.3. Instruments
3.3.1. Stages of Change Readiness and Treatment Eagerness Scale
The Stages of Change Readiness and Treatment Eagerness Scale (SOCRATES) was developed by Miller and Tonigan (1996) to assess readiness and eagerness for change among individuals with SUD. The questionnaire consists of 19 items rated on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). It includes 3 subscales: Recognition, Ambivalence, and Taking Steps. Total scores range from 19 to 95, with higher scores indicating greater treatment eagerness or readiness for change. The Persian version of SOCRATES was validated by Basharpoor (2015). Cronbach’s alpha coefficients for the subscales were reported as 0.76 for Recognition, 0.71 for Taking Steps, and 0.85 for Ambivalence. In the present study, Cronbach’s alpha for the total scale was 0.91.
In this study, the total SOCRATES score was used as an overall indicator of treatment eagerness rather than analyzing the 3 subscales separately.
3.3.2. Family Assessment Device
The Family Assessment Device (FAD) was developed by Epstein, Baldwin, and Bishop (1983) to assess family functioning. The questionnaire contains 60 items scored on a 4-point Likert scale ranging from strongly agree to strongly disagree. Previous studies in Iran have reported acceptable reliability, with Cronbach’s alpha ranging from 0.85 to 0.93. In Kargar’s study (2017), Cronbach’s alpha for this questionnaire was reported as 0.93. In the present study, Cronbach’s alpha for the total scale was 0.91.
Notably, higher FAD scores indicate poorer family functioning.
3.3.3. Multidimensional Scale of Perceived Social Support
The Multidimensional Scale of Perceived Social Support (MSPSS) was developed by Dahlem, Zimet, and Farley (1988) and consists of 12 items measuring perceived social support from 3 sources: family, friends, and significant others. Responses are rated on a 7-point Likert scale from 1 (strongly disagree) to 7 (strongly agree). In Samani’s study (1997), Cronbach’s alpha for this questionnaire was reported as 0.83. In the present study, Cronbach’s alpha was 0.91 for the total scale and 0.85, 0.86, and 0.85 for the family, friends, and significant others subscales, respectively.
3.3.4. Symptom Checklist-25
The Symptom Checklist-25 (SCL-25) is a shortened version of the SCL-90 developed by Najarian and Davoudi (2001) based on a sample of Iranian university students. It contains 25 items rated on a 5-point Likert scale ranging from 0 (rarely) to 4 (very much). The scale includes 7 subscales: dissociation, somatization, anxiety, depression, interpersonal sensitivity, phobia, and obsessive-compulsive symptoms. Subscale scores are calculated by averaging the corresponding items, and a global psychological distress score is obtained by dividing the total score by 25. Higher scores indicate greater psychological distress. In the study by Najarian et al. (2001), Cronbach’s alpha for this questionnaire was reported as 0.91. In the present study, Cronbach’s alpha for the total scale was 0.61.
Although the internal consistency coefficient was relatively low, the scale was retained because of its established use in Iranian populations and its relevance for assessing multiple dimensions of psychological distress in individuals with SUD.
3.3.5. Difficulties in Emotion Regulation Scale
The Difficulties in Emotion Regulation Scale (DERS) was developed by Gratz and Roemer (2004) to assess difficulties in emotion regulation. The questionnaire includes 36 items rated on a 5-point Likert scale from 1 (almost never) to 5 (almost always). Eleven items (1, 2, 6, 7, 8, 10, 17, 20, 22, 24, and 34) are reverse-scored. Higher scores indicate greater difficulties in emotion regulation. In the study by Azizi et al. (2009), Cronbach’s alpha for this questionnaire was reported as 0.92. In the present study, Cronbach’s alpha was 0.70 for the total scale.
3.4. Procedure
After ethical approval was obtained, official permission was granted by Islamic Azad University, Zahedan Branch. A formal letter was then sent to the Welfare Organization of Sistan and Baluchestan Province to facilitate access to residential treatment centers. Four eligible centers in Zahedan were selected based on the study criteria and their willingness to cooperate.
The researcher coordinated with the administrators of each center and explained the study objectives, procedures, inclusion and exclusion criteria, and ethical considerations. Eligible participants were informed about the voluntary nature of participation, the confidentiality of responses, and their right to withdraw at any time without affecting their treatment process. Written informed consent was obtained before questionnaire administration. Incomplete questionnaires were excluded from the final analysis.
3.5. Data Analysis
Data were analyzed at the descriptive and inferential levels. Descriptive statistics included means, standard deviations, and frequency distributions. Treatment eagerness was considered the dependent variable, whereas family functioning, perceived social support, psychological symptoms, and difficulties in emotion regulation were treated as predictor variables.
To examine the relationships among the study variables, stepwise multiple regression analysis was conducted to identify the most significant predictors of treatment eagerness. Before analysis, the assumptions of multiple regression, including normality of residuals, independence of errors, and multicollinearity, were examined and found to be adequately met. The criteria for variable entry and removal in the stepwise procedure were set at P < 0.05 and P > 0.10, respectively.
All statistical analyses were performed using SPSS version 27.
4. Results
4.1. Demographic Characteristics
The largest proportion of participants was in the 25 - 30-year age group, with 40 individuals (35.1%), whereas the smallest proportion was in the 41 - 45-year age group, with 4 individuals (3.5%). Of the 114 participants, 65 (57.0%) were single and 49 (43.0%) were married. Regarding educational level, most participants had less than a high school diploma (66 individuals, 57.9%), followed by 39 participants (34.2%) with a high school diploma and 9 participants (7.9%) with a bachelor’s degree.
4.2. Descriptive Statistics
Descriptive statistics for the main study variables are presented in Table 1. The mean score for perceived social support was 52.68 (SD = 14.96). The mean score for psychological symptoms was 36.88 (SD = 9.19). The mean score for difficulties in emotion regulation was 98.17 (SD = 11.53). In addition, the mean score for family functioning was 141.56 (SD = 22.04), and the mean score for treatment eagerness was 61.55 (SD = 13.60).
Table 1.
Descriptive Statistics of the Study Variables a
| Variables | Mean (SD) | Min-Max |
|---|---|---|
| Treatment eagerness | 61.55 (13.60) | 34 - 90 |
| Family functioning | 141.56 (22.03) | 93 - 207 |
| Perceived social support | 52.68 (14.96) | 20 - 80 |
| Psychological symptoms | 36.88 (9.19) | 15 - 68 |
| Difficulties in emotion regulation | 98.17 (11.53) | 66 - 138 |
a Higher scores indicate higher levels of each measured variable. Abbreviation: SD, standard deviation.
4.3. Correlation Analysis
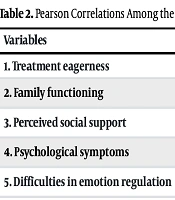
Pearson correlation analysis was conducted to examine the relationships among treatment eagerness, family functioning, perceived social support, psychological symptoms, and difficulties in emotion regulation. As shown in Table 2, treatment eagerness was significantly negatively correlated with family functioning (r = -0.772, P < 0.01) and difficulties in emotion regulation (r = -0.435, P < 0.01). In contrast, treatment eagerness showed significant positive correlations with perceived social support (r = 0.763, P < 0.01) and psychological symptoms (r = 0.307, P < 0.01).
Table 2.
Pearson Correlations Among the Study Variables
| Variables | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| 1. Treatment eagerness | 1 | ||||
| 2. Family functioning | -0.772 a | 1 | |||
| 3. Perceived social support | 0.763 a | -0.738 a | 1 | ||
| 4. Psychological symptoms | 0.307 a | -0.204 b | 0.270 a | 1 | |
| 5. Difficulties in emotion regulation | -0.435 a | 0.445 a | -0.210 b | 0.102 | 1 |
a P < 0.01.
b P < 0.05 (two-tailed).
4.4. Multiple Regression Analysis
Multicollinearity diagnostics for the independent variables are presented in Table 3. All variance inflation factor (VIF) values were below 5, and all tolerance values were above 0.1, indicating that multicollinearity was not a concern in the regression model. Therefore, the standardized regression coefficients were considered stable and interpretable.
Table 3.
Variance Inflation Factor and Tolerance Values for Regression Predictors
| Predictor | VIF | Tolerance |
|---|---|---|
| Family functioning | 2.734 | 0.336 |
| Difficulties in goal-directed behavior | 1.517 | 0.656 |
| Impulse control difficulties | 1.927 | 0.519 |
| Somatization | 1.477 | 0.677 |
| Limited access to emotion regulation strategies | 1.572 | 0.636 |
| Perceived social support | 3.160 | 0.316 |
Because the subscales of difficulties in emotion regulation and psychological symptoms showed differential associations with treatment eagerness, subscale scores rather than total scores were entered into the regression analysis.
To determine the predictive roles of family functioning, perceived social support, psychological symptoms, and difficulties in emotion regulation in treatment eagerness, a stepwise multiple regression analysis was performed. The final regression model is presented in Table 4.
Table 4.
Final Stepwise Regression Model Predicting Treatment Eagerness a
| Predictor | B | β | t | P-Value |
|---|---|---|---|---|
| Family functioning | -0.139 | -0.225 | -3.35 | 0.001 |
| Difficulties in goal-directed behavior | 1.015 | 0.235 | 4.71 | 0.001 |
| Impulse control difficulties | -0.914 | -0.219 | -3.89 | 0.001 |
| Somatization | 0.519 | 0.165 | 3.35 | 0.001 |
| Limited access to emotion regulation strategies | -0.691 | -0.240 | -4.71 | 0.001 |
| Perceived social support | 0.191 | 0.210 | 2.91 | 0.004 |
a The final stepwise regression model was significant (F = 83.48, P < 0.001) and explained 82.4% of the variance in treatment eagerness (R2 = 0.824).
The final model was statistically significant (F = 83.48, P < 0.001) and explained 82.4% of the variance in treatment eagerness (R2 = 0.824, r = 0.908). The results indicated that family functioning (β = -0.225, P = 0.001), difficulties in goal-directed behavior (β = 0.235, P = 0.001), impulse control difficulties (β = -0.219, P = 0.001), somatization (β = 0.165, P = 0.001), limited access to emotion regulation strategies (β = -0.240, P = 0.001), and perceived social support (β = 0.210, P = 0.004) were significant predictors of treatment eagerness.
Overall, these findings indicated significant associations between psychosocial factors and treatment eagerness.
5. Discussion
This study aimed to examine the relationships among family functioning, perceived social support, psychological symptoms, and difficulties in emotion regulation, and treatment eagerness among patients diagnosed with SUD in Zahedan, Iran. The findings indicated that treatment eagerness was significantly associated with family functioning, perceived social support, psychological symptoms, and difficulties in emotion regulation.
The relatively high explained variance may partly reflect conceptual overlap among psychosocial constructs and the use of self-report measures collected at a single time point.
The final regression model indicated that poorer family functioning, lower perceived social support, limited access to emotion regulation strategies, and greater impulse control difficulties were associated with lower treatment eagerness among patients with SUD. In addition, somatic complaints and difficulties in goal-directed behavior were significantly associated with greater treatment eagerness in these patients. These findings are consistent with previous studies on family systems, social support, psychological factors, and emotion regulation in substance use treatment (5-7, 11, 15).
These findings may be explained by the role of family interaction quality and emotional support in shaping individuals’ attitudes toward treatment. Effective family functioning may be associated with greater psychological security, hope, and trust, as well as greater treatment eagerness. In contrast, poor family functioning may be associated with lower treatment eagerness and the development of negative attitudes toward treatment.
According to family systems theory and Bowen’s perspective, the family is an interconnected system, and dysfunction within this system may be associated with increased chronic anxiety, lower differentiation of self, unresolved conflicts, and a lack of emotional support. Such conditions can weaken family emotional cohesion and reduce an individual’s eagerness to seek treatment (13). In addition, structural family theory suggests that unclear or inappropriate roles among family members and ineffective family boundaries may reduce the family’s ability to adapt to change, which may be associated with lower individual responsibility and treatment eagerness (14). Jones et al. underscored the central role of the family in the development, continuation, or cessation of substance use, as well as in treatment adherence (5). In addition, Zeng and Tan reported that healthy family functioning can foster feelings of security and self-worth, which may enhance persistence in treatment and strengthen eagerness for recovery (15).
Perceived social support plays an important role in treatment eagerness among patients with SUD. From a psychosocial perspective, social support is associated with greater feelings of self-worth, belonging, and emotional security, and may be linked to a greater willingness to initiate and maintain treatment. Consequently, individuals who receive greater support from family members, friends, and other significant people in their lives tend to hold more positive attitudes toward treatment and participate in the treatment process with greater eagerness. Khazaee-Pool et al. demonstrated that adequate social support was associated with reduced substance craving and improved quality of life, whereas Liu et al. found that lower perceived social support was associated with a higher likelihood of relapse and reduced treatment eagerness (6, 7).
Psychological symptoms may be associated with individuals’ eagerness for treatment in different ways. Distressing psychological symptoms may be associated with greater discomfort and concern about health, which may, in turn, be related to greater eagerness to seek help and engage in treatment. Consistent with these findings, Liu et al., in a study examining changes in motivation to discontinue substance use among individuals experiencing relapse, reported that psychological factors were associated with the development and strengthening of motivation for substance use cessation. Their findings also indicated that lower perceived stress was associated with greater treatment eagerness (7).
Difficulties in emotion regulation can be conceptualized as a multidimensional construct, with different components showing distinct associations with treatment eagerness. In the present study, limited access to emotion regulation strategies and impulse control difficulties were associated with lower treatment eagerness among individuals with SUD. These difficulties may be related to problems with managing negative emotions, emotional instability, and reduced perceived ability to engage effectively in treatment. In contrast, difficulties in goal-directed behavior showed a positive association with treatment eagerness. One possible explanation is that individuals experiencing greater disruption in daily functioning and goal-directed activities may become more aware of the negative effects of substance use on their lives, which may be associated with greater eagerness to seek treatment and pursue behavioral change.
Chretien et al. noted that although maladaptive emotion regulation strategies may temporarily alleviate emotional distress, they may ultimately be associated with lower eagerness for change and reduced treatment engagement (11). Likewise, previous research has suggested that limited access to effective emotion regulation strategies is often associated with impulsivity, emotional instability, and difficulties in maintaining commitment to therapeutic goals, which may be associated with lower treatment eagerness.
A notable aspect of the present study was its integrated examination of multiple psychosocial determinants within a single analytical model. Although many previous studies have focused on isolated predictors of treatment eagerness, this study simultaneously considered individual, familial, and social factors associated with treatment eagerness. This study represents one of the first comprehensive investigations of these variables among individuals with SUD in Zahedan. As such, the findings provide additional empirical evidence highlighting the multifaceted nature of treatment eagerness in this population.
Overall, the results suggest that effective addiction treatment programs should extend beyond addressing substance use alone. Interventions focused on family functioning, enhancing social support networks, improving psychological symptoms, and developing adaptive emotion regulation skills may be associated with greater treatment eagerness and persistence in recovery.
5.1. Limitations
Despite the contributions of this study, several limitations should be acknowledged when interpreting the findings. First, the cross-sectional design limits the ability to establish causal relationships among the variables studied. Second, participants were recruited from residential treatment centers in Zahedan, Iran, which may restrict the generalizability of the findings to other regions or treatment contexts. In addition, the use of purposive and convenience sampling methods may have reduced the representativeness of the sample. Third, the study sample consisted exclusively of men; therefore, the findings may not be generalizable to women with SUD. Finally, the type of substance used by participants was not specifically categorized or analyzed in this study. Different substances may be associated with distinct psychological profiles, treatment eagerness, and recovery trajectories.
5.2. Implications and Future Research
The findings of this study offer several practical implications for addiction treatment and prevention programs. Treatment providers may benefit from incorporating family-based interventions, strengthening patients’ perceived social support systems, and implementing psychological interventions aimed at improving psychological symptoms and emotion regulation capacities. Integrating these psychosocial dimensions into treatment programs may be associated with greater readiness to initiate and sustain treatment eagerness.
Future studies are encouraged to employ longitudinal or prospective designs to better clarify the relationships between psychosocial factors and treatment eagerness. In addition, research involving more diverse samples, including participants from different regions, treatment settings, and female populations, would improve the generalizability of the findings. Further investigations are also recommended to examine potential differences in treatment eagerness across various types of substances used, as this factor may play a meaningful role in shaping treatment engagement and recovery outcomes.