1. Introduction
Opportunistic infections, including Nocardia spp. and Klebsiella pneumoniae, are predominantly reported in immunocompromised patients (1, 2). It has been noted that lung injury, associated with high mortality, is the primary manifestation of Nocardia infections (3). Moreover, Nocardia spp. comprises a diverse group of bacteria, though brain lesions caused by these organisms are relatively rare (4). Nocardia gipuzkoensis, a newly identified species within the Nocardia genus, is an uncommon cause of cerebral abscess (5, 6). However, the optimal treatment for N. gipuzkoensis infection has yet to be established.
Klebsiella pneumoniae, a member of the Enterobacteriaceae family, is widely distributed in terrestrial and aquatic environments (7). This strain is particularly significant in community-acquired infections and has progressively developed antimicrobial resistance to multiple drugs (8). Therefore, clinicians must monitor therapeutic efficacy based on antimicrobial susceptibility test (AST) results.
Herein, we describe a rare case of concurrent infection in a 71-year-old female, whose good prognosis provides supporting evidence for effective treatment of nocardiosis and pneumonia caused by N. gipuzkoensis and K. pneumoniae, respectively. Based on this case, we aim to optimize treatment strategies and improve outcomes in managing concurrent infections.
2. Case Presentation
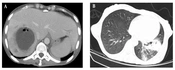
A 71-year-old female patient was referred to our hospital due to an intracranial space-occupying lesion persisting for over 20 days. A review of her case history revealed chief complaints of lisping, right-hand buffeting, a mild cough with expectoration, and no fever. Initial computerized tomography (CT) and contrast-enhanced magnetic resonance imaging (MRI) of the cranium revealed an intracranial space-occupying lesion. Additionally, chest CT showed a pulmonary mass in the upper lobe of the left lung. The preliminary diagnosis suggested a lung tumor with brain metastases, and the patient was treated with a diuretic agent to relieve intracranial pressure (day 0, Figure 1). However, an enhanced chest CT performed on day 10 continued to show a persistent pulmonary mass with an inflammatory component. Lung tissue was subsequently collected via paracentesis for pathology, confirming chronic lung inflammation with alveolar epithelial hyperplasia rather than a tumor. Empirical treatment with azithromycin (500 mg once daily) was initiated. Further cranial diffusion-weighted imaging (DWI) revealed a left parietal space-occupying lesion, suggesting a brain abscess (day 22).
![The timeline of therapy. Brain imaging [computerized tomography (CT) and/or magnetic resonance imaging (MRI)] and thoracic imaging (CT and/or MRI) were all listed and marked in arrows. The corresponding therapy were also marked in red dots. The treatment of vancomycin (1 g/12 h, iv) and meropenem (2 g/8 h, iv) was showed as yellow line, and the treatment of linezolid (0.6 g/12 h, po) and levofloxacin (0.5 g/24 h, po) was represented as green line. Green box indicated the C-reactive protein (CRP) value with the corresponding time.](https://brieflands.com/journals/jjm/articles/158335/figures/jjm-158335-i001-F1-preview.webp "The timeline of therapy. Brain imaging [computerized tomography (CT) and/or magnetic resonance imaging (MRI)] and thoracic imaging (CT and/or MRI) were all listed and marked in arrows. The corresponding therapy were also marked in red dots. The treatment of vancomycin (1 g/12 h, iv) and meropenem (2 g/8 h, iv) was showed as yellow line, and the treatment of linezolid (0.6 g/12 h, po) and levofloxacin (0.5 g/24 h, po) was represented as green line. Green box indicated the C-reactive protein (CRP) value with the corresponding time.")
Figure 1.
The timeline of therapy. Brain imaging [computerized tomography (CT) and/or magnetic resonance imaging (MRI)] and thoracic imaging (CT and/or MRI) were all listed and marked in arrows. The corresponding therapy were also marked in red dots. The treatment of vancomycin (1 g/12 h, iv) and meropenem (2 g/8 h, iv) was showed as yellow line, and the treatment of linezolid (0.6 g/12 h, po) and levofloxacin (0.5 g/24 h, po) was represented as green line. Green box indicated the C-reactive protein (CRP) value with the corresponding time.
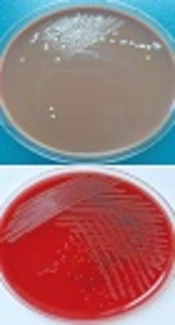
To further evaluate the nature of the intracranial lesion, the patient was referred to our hospital (day 26). Routine blood tests revealed an elevated C-reactive protein (CRP) level (Figure 1). Preoperative CT localization confirmed the left parietal lesion, with progressive focal involvement and perilesional edema. Based on previous imaging findings, a paracentesis and drainage procedure for the brain lesion was performed (day 29). Microbial culture and metagenomic next-generation sequencing (mNGS) of the drainage fluid identified N. gipuzkoensis with susceptibility to meropenem [minimum inhibitory concentration (MIC), 0.008 μg/mL], penicillin G (MIC, 1 μg/mL), and vancomycin (MIC, 0.25 μg/mL). Notably, N. gipuzkoensis was not detected in the sputum, but K. pneumoniae was identified from sputum culture with broad-spectrum sensitivity, including susceptibility to meropenem (MIC, ≤ 0.125 μg/mL) and levofloxacin.
Following paracentesis, a treatment regimen of meropenem (2 g every 8 hours intravenously) combined with vancomycin (1 g every 12 hours intravenously) was initiated due to the patient’s history of sulfonamide allergy. By day 43, neurological symptoms had improved, with resolution of lisping and right-hand buffeting. Consequently, the patient was discharged, and the treatment regimen was adjusted to oral linezolid (0.6 g every 12 hours) and levofloxacin (0.5 g every 24 hours). After one month of treatment (day 70), a clinical follow-up revealed no functional impairment on physical examination. Cranial CT showed a reduction in the high-density area of the brain lesion and perilesional edema. The inflammatory focus in the superior lobe of the left lung had also diminished, with minimal pleural reaction. Oral administration of linezolid and levofloxacin was continued. By day 133, cranial CT and contrast-enhanced MRI demonstrated further improvement, with no neurological deficits observed.
3. Discussion
The genus Nocardia is commonly associated with localized or disseminated infections in humans; however, it is considered a rare pathogen in the context of brain abscess treatment. This case presents a 71-year-old patient with a concurrent brain abscess caused by N. gipuzkoensis and a pulmonary infection caused by K. pneumoniae. With the aid of rapid mNGS and precise antibiotic therapy, the concurrent infection caused by the newly reported species N. gipuzkoensis was successfully treated, providing valuable clinical reference for the management of N. gipuzkoensis infections.
The definitive diagnosis of this case as an infectious disease was complex, necessitating urgent treatment for N. gipuzkoensis. Given the imaging findings of a cranial space-occupying lesion and a pulmonary mass, the initial diagnosis suggested a lung tumor with brain metastases. However, after paracentesis confirmed chronic lung inflammation, the clinician reconsidered the cranial lesion as a potential brain abscess and referred the patient to our hospital on day 26. For brain abscess therapy, targeted antimicrobial treatment based on pathogen identification and AST is strongly recommended, as outlined in clinical guidelines (9). Nocardia gipuzkoensis was ultimately identified as the causative pathogen of the brain abscess in this case. Reported treatments for Nocardia species include trimethoprim-sulfamethoxazole, linezolid, amikacin, and imipenem (10). The AST results for N. gipuzkoensis in this patient demonstrated susceptibility to meropenem, penicillin G, and vancomycin. Considering guideline recommendations, the patient’s history of sulfonamide allergy, and AST results, the initial antibiotic regimen for N. gipuzkoensis consisted of meropenem (2 g every 8 hours intravenously) combined with vancomycin (1 g every 12 hours intravenously) for two weeks, leading to a reduction in the patient’s symptoms.
Subsequently, the pulmonary infection was confirmed as K. pneumoniae through sputum culture, rather than Nocardia spp. The presence of different pathogens in a concurrent infection increased the complexity of clinical decision-making. K. pneumoniae is frequently reported to exhibit resistance to multiple antibiotics (11, 12); therefore, treatment decisions must be guided by AST results. As previously reported, K. pneumoniae is considered a multidrug-resistant (MDR) pathogen with a high risk of morbidity and mortality due to limited therapeutic options. Notably, the resistance rate of K. pneumoniae has steadily increased over the years, posing a significant challenge to empirical antibiotic therapy for K. pneumoniae infections (2). Additionally, clinicians should closely monitor the patient’s condition and treatment response, making adjustments as necessary (13).
For this case, AST of K. pneumoniae demonstrated sensitivity to meropenem and levofloxacin. Despite the AST results, meropenem therapy did not resolve the lung inflammation. Consequently, levofloxacin was administered, leading to improvement in lung injury. This outcome highlights the potential disparity between in vitro antimicrobial activity and in vivo pharmacological efficacy. A reliable in vivo model is needed to accurately reflect the real-world effectiveness of antibiotics in preventing infections. Given the susceptibility of N. gipuzkoensis to linezolid and K. pneumoniae to levofloxacin, oral administration of linezolid and levofloxacin was ultimately prescribed upon discharge.
Diagnosis of a brain abscess typically begins with brain CT or MRI and is confirmed through neurological excision or aspiration. Optimal empirical and targeted antimicrobial therapy is crucial for controlling and managing such infections (9). In accordance with established recommendations, a combination of meropenem and vancomycin was used as empirical therapy following neurosurgery. The 2-week intravenous regimen effectively alleviated neurological symptoms, after which a 6-week course of oral linezolid and levofloxacin was initiated.
The clinical pharmacological dosing of antibiotics varies depending on the specific agent, and the relationship between antibiotic administration and pharmacokinetic optimization remains incompletely understood. Further studies are required to establish optimal dosing strategies for therapeutic efficacy. Although early transition from intravenous to oral administration is not yet sufficient to warrant a formal recommendation (14), this case provides supporting evidence for the potential to shorten the duration of intravenous therapy for nocardiosis. Additionally, the application of mNGS effectively facilitated the identification of N. gipuzkoensis, a newly recognized species. The rapid and precise identification of pathogens contributed to the tailored antimicrobial regimen and successful treatment in this case.
A review of the literature on cerebral abscesses caused by Nocardia spp. infection (15) indicates that a patient with N. farcinica was successfully treated with linezolid for 182 days, while another patient with N. cyriacigeorgica infection was cured after 64 days of linezolid therapy. Conversely, a patient with N. wallacei infection succumbed after 308 days of linezolid treatment. These findings suggest potential variations in antibiotic sensitivity among different Nocardia species.
Nocardia gipuzkoensis, an uncommon species, demonstrated sensitivity to linezolid in our study. Although the cerebral abscess in this patient ultimately resolved following an extended course of linezolid therapy, data regarding the MIC and optimal treatment duration remain unclear. Furthermore, in this case of concurrent infections, levofloxacin—rather than the initial meropenem therapy—was effective in resolving K. pneumoniae-associated lung injury, as indicated by AST results. This case highlights the importance of correlating in vitro susceptibility data with in vivo treatment outcomes.
Further research is needed to elucidate the epidemiology and pathogenesis of N. gipuzkoensis infections, particularly in cases involving concurrent infections, to guide optimal therapeutic strategies.
3.1. Conclusions
This case provides evidence supporting the successful management of concurrent cranial N. gipuzkoensis and pulmonary K. pneumoniae infections. The treatment regimen consisted of intravenous meropenem and vancomycin for 2 weeks, followed by oral linezolid and levofloxacin for 6 weeks. These findings may contribute to emerging evidence supporting a potential reduction in the duration of intravenous therapy for nocardiosis.