1. Background
Staphylococcus aureus can be carried asymptomatically and it is one of the main causes of hospital and community-acquired infections (1). The extensive use of antibiotics for the treatment of S. aureus skin and soft tissue infections has caused selective pressure and eventually has given rise to multiple drug-resistant strains (2). Fusidic acid is an antibiotic often used in topical preparations for skin infections of S. aureus. It inhibits bacterial protein synthesis by binding to elongation factor G (EF-G), through which preventing its release from the ribosome and consequently, the elongation of nascent polypeptides (3). Fusidic acid-resistant Staphylococcus aureus (FRSA) has been reported in many countries to have a remarkable difference in resistance determinants. Fusidic acid resistance is very important because it might lead to the failure of topical treatment, especially when it is used as empiric therapy. In addition, its resistance might be linked to other antibiotic resistances. The overall rate of fusidic acid resistance is still relatively low. However, there is an increase in the prevalence of clinical isolates of FRSA worldwide.
There are a number of fusidic acid resistance mechanisms among S. aureus and other staphylococci (4, 5). Numerous classes of fus genes have been recognized in fusidic acid-resistant S. aureus. The FusA class is linked to mutations in the chromosomal EF-G-encoding gene fusA that reduce the fusidic acid binding with EF-G ribosome complex (6). FusA mutations are mostly seen in the structural domain III of EF-G, and to a lower extent in domains I and V, and they are associated with high-level resistance (7). The fusA-small-colony variant (SCV) class is a subset of the FusA class in which mutations in fusA mostly appear in the structural domain V of EF-G, and some in domains I and III. The mutants of this class are the SCVs of S. aureus (8). They are characterized by slow growth and are implicated in chronic and relapsing infections (9).
Mutants of the FusE class carry mutations in rplF, which encodes ribosomal protein L6 that is situated at the interaction site with EF-G; these mutants also demonstrate the SCV phenotype and either hemin or menadione auxotrophy (10). In contrast, the FusB, FusC, and FusD classes harbor fusidic acid-resistance genes that yield proteins protecting EF-G from binding to fusidic acid and can be transmitted horizontally. In addition, they result in low-level resistance (11). The fusB gene is carried on different genetic elements (12); it can be present on the pUB101 plasmid, on a transposon-like element, or else in a pathogenicity island (4). The fusC and fusD genes are located on the chromosome in clinical isolates of different Staphylococcus species (13). The fusC gene has been associated with S. aureus, S. intermedius, and S. epidermidis, whereas fusD has been associated with S. saprophyticus and is the cause of intrinsic resistance of the bacteria to fusidic acid (4, 5).
2. Objectives
There is a lack of data concerning the prevalence of fusidic acid resistance amongst S. aureus isolates from Jordan. Therefore, the present study was performed to determine the rate and distribution of fusidic acid resistance, including fusB and fusC resistance genes, among clinical isolates from Jordan.
3. Methods
3.1. Collecting and Identifying Staphylococcus aureus Isolates
This prospective cross-sectional study was conducted using 113 clinical S. aureus isolates collected from adult Jordanian patients admitted to Prince Hamzah Hospital in Amman between February 1st, and July 30th, 2015. Of the 113 isolates, 63 (55.8%) were isolated from skin and soft tissues, 28 (24.8%) from respiratory secretions, including nasal swabs and sputum, 15 (13.3%) from blood, and seven (6.1%) from urine. Control nasal and skin sample specimens were obtained from 288 healthy adults from the community using sterile cotton swabs, and were placed in screw-capped tubes containing trypticase soy broth supplemented with 7% NaCl (14). Each isolate was cultured and identified presumptively as S. aureus by colony morphology, gram staining, and a set of biochemical tests, including catalase test, coagulase activity using rabbit plasma (Remel-Oxoid, Lenexa, UK), and mannitol fermentation. The isolates were further verified as being S. aureus by confirmation of the occurrence of the thermonuclease-encoding (nuc) gene by polymerase chain reaction (PCR) (15).
3.2. Testing for Antimicrobial Susceptibility
We detected the antimicrobial susceptibility to fusidic acid (FD/10 µg), penicillin G (10 unit), gentamicin (CN/10 µg), erythromycin (E/15 µg), teicoplanin (TEC/30 µg), cefoxitin (FOX/30 µg), vancomycin (VA/30 µg), clindamycin (DA/2 µg), and sulfamethoxazole-trimethoprim (SXT/25 µg) using the disc diffusion method in accordance with the guidelines of the Clinical and Laboratory Standards Institute (16). All antibiotics were obtained from Oxoid (Hampshire, UK). The methicillin-resistant Staphylococcus aureus (MRSA) phenotype was affirmed by the standard PCR for the mecA gene in the resistant isolates (15). The interpretive criteria for susceptibility and resistance to fusidic acid (10-μg disc) were the inhibition zones of ≥ 22 mm and < 19 mm, respectively, according to Jones et al. (17). The minimum inhibitory concentration (MIC) of fusidic acid was determined using an E-test as the standard procedure in most clinical microbiology laboratories.
The E-test (Liofilchem, Roseto Degli Abruzzi, Italy) consisting of a thin strip carrying a continuous gradient of fusidic acid was deposited on the surface of inoculated Mueller-Hinton agar plates in accordance with the instructions of the manufacturer; in this method, fusidic acid diffuses into the agar to generate its MIC value. This technique is less time-consuming, less expensive if limited drugs are tested, easy to execute, and suitable for testing of certain fastidious bacteria. Two S. aureus strains (ATCC 25923 and ATCC 43300) were used as control strains. Both control strains were obtained from Oxoid (Culti-Loops® Remel- Basingstoke- UK). Stock cultures of these strains were maintained at 4°C on slopes of nutrient agar. Cultures for experiments were prepared by transferring a sample from the stock cultures into Mueller-Hinton broth (MHB) and incubating without agitation for 24 hours at 37°C. The cultures were diluted with fresh Mueller-Hinton broth to achieve optical densities corresponding to 2.0 × 106 colony forming units (CFU/mL). The fusidic acid MIC for S. aureus was grouped as recommended by the European Committee for Antimicrobial Susceptibility Testing (EUCAST)/British Society of Antimicrobial Chemotherapy (BSAC) criteria into susceptible where MIC ≤ 1 µg/mL and resistant where MIC >1 µg/mL (18).
3.3. Detecting of Fusidic Acid Resistance Determinants
All isolates that had fusidic acid MICs of > 1 mg/L were further verified for the occurrence of the fusB and fusC genes using the specific primers listed in Table 1 (6). The E.Z.N.A.® Bacterial DNA Kit (Omega Bio-Tek, USA) was used to isolate genomic DNA from an overnight culture according to the manufacturer’s instructions. PCR amplification was performed according to Lannergard et al. (6).
Table 1.
The Oligonucleotide Primers Used in the Study
| Name | Sequence (5’ – 3’) | Product Size, bp |
|---|---|---|
| fusB | 930 | |
| Forward | CGCCACTCAATGAGTGACGCT | |
| Reverse | CGGGAGGTGATGATGTTATGT | |
| fusC2 | 750 | |
| Forward | ATGAATAAAATAGAAGTGTATAAGTTTGTTAAA | |
| Reverse | CTATTTTATTTTAACAATAAATTCGTAAAGATT |
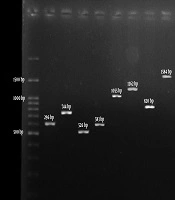
Thermocycling conditions were as follows: preliminary denaturation at 94°C for 5 minutes, and then 30 cycles of denaturation at 94°C for 30 seconds, followed by annealing at 55°C for 30 seconds, and final elongation at 72°C for 1 minutes. Electrophoresis on 1.5% agarose gels was done on the PCR products and then visualized under ultraviolet light after EtBr staining.
3.4. Data Analyzing
SPSS 22.0 (SPSS Inc., Chicago, USA) was used for statistical analysis. Contingency tables analysis (chi-square test) was used to assess variations in frequencies. The Fisher’s exact test was applied with frequencies of less than five. Variations were considered significant at P < 0.05.
4. Results
4.1. Demographics
Demographic information of the sources of isolates is shown in Table 2. The healthy subjects were significantly younger than the patients.
Table 2.
Demographic Information of the Sources of Isolatesa
| Characteristic | Patients (N = 113) | Healthy Adults (N = 288) |
|---|---|---|
| Sex | ||
| Male | 58 (51.3) | 140 (49.7) |
| Female | 55 (48.7) | 148 (51.3) |
| Age, y | ||
| < 25 | 19 (16.8) | 288 (100) |
| 26 - 50 | 47 (41.6) | 0 (0) |
| ≥ 51 | 43 (38.1) | 0 (0) |
aValues are expressed as No. (%).
4.2. Prevalence and Distribution of FRSA Isolates
Table 3 shows that the FRSA rate was significantly (P < 0.05) lower in the healthy adult control group (3/288, 1%) than in patients (36/113, 31.9%). The incidence of MRSA and methicillin-sensitive Staphylococcus aureus (MSSA) was detected in 53.1% (60/113) and 46.9% (53/113) of the patients, respectively.
Table 3.
Distribution of Fusidic Acid-Resistant and Sensitive Isolates in Patients and Healthy Adultsa
| Clinical Isolates (N = 113) | Healthy Control Isolates (N = 228) | |
|---|---|---|
| FRSA | 36 (31.9) | 3 (1) |
| FSSA | 77 (68.1) | 285 (99) |
Abbreviations: FRSA, fusidic acid-resistant Staphylococcus aureus; FSSA, fusidic acid-sensitive S. aureus.
aValues are expressed as No. (%).
The rate of FRSA was significantly (P < 0.05) higher among MRSA than among MSSA isolates (n = 24, 66.7% and n = 12, 33.3%, respectively) (Table 4). We found no association between fusidic acid determinants among MRSA and MSSA (P > 0.05).
Table 4.
Distribution of Fusidic Acid Resistance Determinants Amongst 36 MSSA and MRSA Clinical Isolates
| Total No. of Isolates (%) | No. of MRSA Isolates (%) | No. of MSSA Isolates (%) | |
|---|---|---|---|
| fusB | 14 (38.9) | 9 (25) | 5 (13.9) |
| fusC | 6 (16.7) | 5 (13.9) | 1 (2.8) |
| Non-fusB, non-fusC | 16 (44.4) | 10 (27.8) | 6 (16.7) |
| Total | 36 (100) | 24 (66.7) | 12 (33.33) |
Abbreviations: MRSA, methicillin-resistant Staphylococcus aureus; MSSA, methicillin-sensitive S. aureus.
Fusidic acid-resistant S. aureus isolates were significantly (P < 0.05) more abundant among clinical than among healthy control isolates (Table 3). While the distribution of FRSA clinical isolates was not statistically significant between sample types (Table 5). However, we found that all FRSA isolates from healthy individuals were from nose specimens.
Table 5.
The Percentage of Fusidic Acid-Resistant Staphylococcus aureus Isolates in Four Sample Typesa
| Source of Isolates | FRSA Isolates |
|---|---|
| Skin and tissue | 19 (16.8) |
| Respiratory secretions | 12 (10.6) |
| Blood | 3 (2.7) |
| Urine | 2 (1.8) |
Abbreviation: FRSA, fusidic acid-resistant Staphylococcus aureus.
aValues are expressed as No. (%).
4.3. Antibiotic Resistance Phenotypes of FRSA and FSSA
The percentage of FRSA isolates resistant to various other antimicrobial agents is shown in Table 6, which ranged from 0% for vancomycin to 100% for penicillin G. A high degree of resistance to erythromycin was observed, followed by clindamycin, gentamicin, and sulfamethoxazole-trimethoprim. The rate of resistance to teicoplanin was relatively low.
Table 6.
Comparison of the Resistance Profile Between FRSA and FSSA Isolates
| Antimicrobial Agent | ||||||||
|---|---|---|---|---|---|---|---|---|
| VA | TEC | SXT | CN | DA | E | FOX | P | |
| Resistance of FRSA isolates, % | 0 | 9.10 | 24.2 | 45.50 | 54.50 | 66.70 | 72.7 | 100 |
| Resistance of FSSA isolates, % | 0 | 2.70 | 13.3 | 14.20 | 32.70 | 43.4 | 53.10 | 100 |
Abbreviations: CN, gentamicin; DA, clindamycin; E, erythromycin; FOX, cefoxitin; FRSA, fusidic acid-resistant Staphylococcus aureus; FSSA, fusidic acid-sensitive S. aureus; P, penicillin G; TEC, teicoplanin; VA, vancomycin; SXT, sulfamethoxazole-trimethoprim.
The data in Table 6 show that the resistance of FSSA isolates to various other antimicrobial agents ranged from 0% for vancomycin to 100% for penicillin G. In general, lower degrees of resistance were noticed in FSSA isolates than in FRSA isolates.
4.4. Fusidic Acid Resistance
The results showed a significant (P < 0.05) relationship between fusidic acid resistance genes and resistance rate. Fusidic acid MICs ranged between 6 and ≥ 128 µg/mL. The majority of FRSA isolates (72.2%) displayed a low level of resistance (MIC ≤ 32 µg/mL), whereas 27.8% of isolates displayed an elevated level of resistance (MIC ≥ 128 µg/mL) (Table 7).
Table 7.
Distribution of FRSA Isolates According to Fusidic Acid Resistance Determinants and MICa
| Resistance Determinant | Total Isolates | No. of Isolates | P Value | |
|---|---|---|---|---|
| Low-Level Resistance, MIC ≤ 32 | High-Level Resistance, MIC ≥ 128 | |||
| fusB | 14 (38.9) | 14 | 0 | 0.0078 |
| fusC | 6 (16.7) | 5 | 1 | |
| Non-fusB, non-fusC | 16 (44.4) | 7 | 9 | |
| Total | 36 (100) | 26 (72.2) | 10 (27.8) | |
Abbreviation: MIC, minimum inhibitory concentration.
aValues are expressed as No. or No. (%).
Amplification of the fusB and fusC genes with specific primers revealed that each resistant isolate carried a single resistance gene; 38.9% carried fusB, 16.7% carried fusC, and 44.4% of the isolates possessed neither fusB nor fusC (Table 4). Table 7 shows that most FRSA isolates harboring fusB and fusC (19/36 (52.7%) possessed a low degree of resistance (MIC ≤ 32 µg/mL). One isolate with a high level of resistance possessed the fusC gene. However, most isolates that did not have fusB or fusC showed a high degree of resistance (> 128 µg/mL). Interestingly, there was a statistically significant correlation between fusidic acid MICs and resistance genes (P < 0.05) (Table 7).
5. Discussion
A study in Jordan by Aqel et al. (15) revealed a high rate of infections with MRSA in both hospital and community-acquired diseases. In Jordan, fusidic acid is one of the conventional over-the-counter antibiotics increasingly used for the management of S. aureus skin and soft tissue infections. It is exclusively used topically either alone or in combination with anti-inflammatory agents, such as cortisone. The occurrence and mode of resistance of S. aureus clinical isolates to fusidic acid have not been studied in Jordan. We believe this is the first report on fusidic acid resistance gene determination among clinical S. aureus isolates from Jordan. Here, S. aureus phenotypic and genotypic characteristics were studied to explain the molecular mechanism underlying resistance.
The study revealed a significantly higher rate of fusidic acid resistance amongst clinical isolates than amongst isolates collected from healthy individuals, and it was comparably higher than those reported in other Arabic countries, such as Morocco (14%) (19). However, compared to European findings, the FRSA rate in Jordan is lower (31.9% vs. 64.9%), the occurrence of fusB is four times higher (38.9% vs. 10.1%), and the occurrence of fusC is similar (16.7% vs. 16.9%) (20). Interestingly, the FRSA rates were notably lower in the USA (0.3%), Canada, and Australia (7.0% for both countries), which can be explained by the fact that fusidic acid is not listed as a prescribed medication and is not yet authorized by the US Food and Drug Administration (21).
This corroborates that excessive antibiotic use exerts a selective pressure and increases the rate of resistance, and thus might affect the treatment regimen and narrow the choice of antibiotics effective against S. aureus. The resistance rate of FRSA isolates to antibiotics tested was overwhelmingly higher than that corresponding to the FSSA isolate. However both groups showed high susceptibility to vancomycin and teicoplanin. The retained susceptibility to vancomycin and teicoplanin correlates with the restricted use of the drug and indicates its usefulness. It is also worth mentioning that the percentage of FRSA isolates was significantly different among various sample types. A possible explanation is that skin commensal staphylococci may be a major source for fusidic acid resistance genes as suggested by Wei-Chun Hung et al. (22). A successful clone of FRSA circulating in the hospital could account for clonal expansion, thus spreading the resistance.
The study showed a high prevalence of fusB and fusC genes among isolates, with fusB being more prevalent than fusC. Previously, fusB was the predominant element causing fusidic acid resistance among 73.2% and 90% of S. aureus isolates in China and the Netherlands, respectively (23, 24). In contrast, Elazhari et al. reported that FusC was the most known fusidic acid resistance element among S. aureus from Casablanca (25). In Australia, New Zealand, the USA, and some European countries, fusC was the most common fusidic acid resistance gene (20, 21). In Canada, fusB and fusC occur at the same rates amongst S. aureus isolates (20, 21). Studies in Taiwan revealed that 84% of fusidic acid-resistant MRSA isolates had fusA mutations (20, 21, 26).
We found a significant association between the genetic determinants and the level of fusidic acid resistance. All fusB and fusC carrying isolates had low levels of resistance. The majority of the isolates that lacked fusB and fusC genes presented high fusidic acid resistance. This is in accordance with the results of Chen et al. (26) showing that generally isolates with fusA mutations were highly resistant to fusidic acid (MIC ≥ 128 µg/mL), whereas isolates with other determinants (fusB or fusC) had low-level resistance (MIC ≤ 32 µg/mL) (26). The present study had several limitations; it was a single-hospital study and a limited number of samples were collected over a period of only six months. To reflect the trend in infections caused by FRSA strains in the region, we need a multicenter study involving all types of healthcare setups for a longer period. In addition, we did not evaluate the presence of potentially new mutations in fusB, fusC, and fusA. Finally, there were no data on antibiotic use history of the patients. Thus, further investigation is warranted.
5.1. Conclusions
In conclusion, the rate of fusidic acid resistance is high amongst clinical isolates of S. aureus, particularly among MRSA isolates in Jordan. FRSA isolates in Jordan presented unique epidemiological characteristics, with a high incidence of fusB-carrying isolates. Furthermore, the majority of the isolates with acquired resistance genes had a low level of resistance to fusidic acid. Based on the findings of this study, further investigations and comparative studies should be performed in various patient groups and clinical conditions. Research to examine the presence of potentially new and novel mutations in the fusA gene is recommended. Antimicrobial susceptibility testing for fusidic acid is strongly recommended in medical laboratories. The restricted use of fusidic acid is advised.