1. Background
Adeno-tonsillectomy surgery in pediatrics is commonly managed as an ambulatory surgery. This may be attributed to the use of the electro-dissection surgical technique that decreases the incidence of immediate postoperative hemorrhage. However, use of the electro-cautery technique increases postoperative inflammation (1, 2). The inflammatory process involves the release or generation of multiple inflammatory mediators from the damaged tissues. Some mediators, such as bradykinin and serotonin, may directly activate the peripheral nociceptive receptors. Other mediators, such as prostaglandins, increase the sensitivity of nociceptive receptors to other mediators. Thus, increased inflammation is associated with increased postoperative pain and discomfort, especially during the first postoperative day (3, 4).
Increased postoperative pain can delay hospital discharge, delay return to school, and affect the child’s nutrition (5). Many techniques were tried to alleviate postoperative pain following adeno-tonsillectomy and improve the patients’ and parents’ comfort, with conflicting outcomes. These included the use of systemic opioid analgesics (6), non-steroidal anti-inflammatory medications (7), corticosteroids (8), local anesthesia spray (9), and local anesthesia infiltration (10).
2. Objectives
Glossopharyngeal nerve block, when used in children presented for tonsillectomy, may improve the duration and the quality of postoperative analgesia. The aim of this clinical trial was to evaluate the effect of glossopharyngeal nerve block on the time of the first call for rescue analgesia (primary outcome) and pain scores during swallowing and resting (secondary outcome) in children undergoing tonsillectomy.
3. Methods
This prospective double-blinded trial was conducted at Tanta University Hospitals after approval of the local research ethics committee was obtained (Tanta Faculty of Medicine Research Ethics Committee 34531/07/2017), and it was registered at the Pan African Trial Registry (identification number: PACTR201711002816160). It lasted for nine months (August 2017 to April 2018). Children aged four to ten years old, of both genders, American Society of Anesthesiologists classes I or II, and scheduled for adeno-tonsillectomy were included in this study. Diabetic children, those with cardiac, renal, or liver diseases, those suspected for or having evident hypersensitivity to the used medications, those with peritonsillar abscess, those with swallowing disorders, and those receiving regular analgesia within the last week before surgery were all excluded from the study.
All patients underwent pre-anesthetic checkup, and routine laboratory investigations were requested from them, including complete blood count and coagulation assessment. The study was adequately explained to the guardians of the children, including its purpose, technique, benefits, and risks, as well as methods to overcome them. Parents, who accepted to participate were reassured and asked to sign informed written consent. The children were kept fasting from solid food for six hours and from clear water for two hours before surgery. They were also reassured and received full explanation of the whole process on the morning of the surgery.
In the preparation room and under the supervision of a well-trained expert nurse, all children were premedicated 30 minutes before surgery with atropine 0.01 mg/kg and midazolam 0.04 mg/kg, intravenously. They were then transported to the operating room and attached to a non-invasive monitor consisting of a 5-lead electrocardiogram, a Noninvasive Blood Pressure (NIBP) monitoring system, and a pulse oximeter to measure oxygen saturation (SpO2). The induction of anesthesia was carried out by fentanyl 1 μg/kg, propofol 2 mg/kg, and cisatracurium 0.15mg/kg to facilitate tracheal intubation. A cuffed endotracheal tube of suitable size was then introduced, with the patient attached to a mechanical ventilator, parameters being adjusted to maintain normocapnia (EtCO2 35 ± 4 mmHg). Isoflurane 1.2% in oxygen:air (1:1) was used to maintain anesthesia. All children received an intravenous fluid infusion composed of D5 ½ at a rate of 6 mL/kg/hour. Paracetamol 15 mg/kg I.V. was administered over the span of 15 minutes.
Tonsillectomies were carried out by the same expert surgeon using the same technique (bipolar electro-cautery). The patients were randomly distributed to two equal groups by the aid of a computer generated software of randomization that introduced groups in sealed closed envelopes. This made sure that parents stay blind to the group their children were assigned to.
3.1. Control Group (Group C)
The patients in this group did not receive glossopharyngeal nerve block at the end of the surgery.
3.2. Glossopharyngeal Nerve Block Group (Group G)
At the end of the surgery, glossopharyngeal nerve block was carried out using 10 mL (5 mL in each side) of a local anesthetic mixture composed of 0.25% plain bupivacaine (Marcaine, ASTRA, UK).
3.3. The Technique of Glossopharyngeal Nerve Block
Glossopharyngeal nerve block was carried out by the surgeon with the aid of McIvor gag and a 25-gauge spinal needle, set at an angle of 45 degrees at a distance of 1 cm from its tip. In the middle point of the palatopharyngeal fold (posterior tonsillar pillar), the needle pierced the retropharyngeal mucosa and was directed behind the posterior tonsillar pillar as lateral as possible. It was then inserted in the pharyngeal wall at a depth of about 0.5 cm. After careful aspiration, the prepared local anesthetic mixture was slowly injected over the span of three minutes.
At the end of the surgery, inhalational anesthesia was switched off and muscle relaxation was reversed (using neostigmine 0.05 mg/kg and atropine 0.01 mg/kg), with full awake extubation, and the children being kept in lateral position. They were then transported to the PACU for close observation and monitoring. They were discharged when the modified Aldrete score reached 10. All measurements were obtained by an assistant physician, who was not participating in the study and who was blinded to its groups.
The FLACC behavioral pain assessment scale (13) was used to assess postoperative pain during rest and during swallowing, 30 minutes, two, four, six, 12, 18, and 24 hours after surgery. Children with a pain score of four or more received pethidine 0.5 mg/kg I.V. as rescue analgesia, which may be repeated, taking in consideration that the total daily dose should not exceed 1.5 mg/kg. The time of first request of rescue analgesia was recorded, representing the time interval between the end of the surgery and the first request of rescue analgesia (primary outcome). The total dose of pethidine consumed in the first 24 hours was also recorded.
In the PACU, gag reflex was assessed by a tongue depressor that was used to lightly touch the posterior wall of the lower part of the oropharynx and estimate the patients response (none: no response, mild: grimace but tolerable, moderate: facial flushing, or severe: facial flushing with coughing, lacrimation, or restlessness). Moreover, before discharge from the PACU, swallowing was assessed by the aid of a four-point scale (none: normal or no difficulty in swallowing, mild: some difficulty in swallowing, moderate: effort is required for swallowing, or severe: no swallowing or swallowing only with maximal effort).
The incidence of perioperative complications, such as postoperative nausea and vomiting, delayed hospital discharge, choking, local anesthetic toxicity, dyspnea, bradycardia, dry mouth, nasal obstruction, hoarseness of voice, or foreign body sensation in the throat, was also assessed. On the second postoperative day, the parents were asked to rate their satisfaction with postoperative analgesia given to their children, as either very good, good, fair, bad, or very bad. The children were discharged from the hospital after at least 24 hours and when there was no bleeding, nausea, or vomiting, they were able to swallow clear fluids, and their pain score was less than four.
3.4. Statistics
A pilot study was conducted to assess the effect of glossopharyngeal nerve block on the time for the first request for pethidine rescue analgesia in 10 children (not included in the final study) presented for tonsillectomy. The use of glossopharyngeal nerve block significantly increased the time for the first request of analgesia from 3.11 ± 1.73 hours to 6.93 ± 2.88 hours. Based on these results, 45 patients from each group were required to detect a significant increase by two hours in the time for the first request of rescue analgesia, at an α value of 0.05 and 90% power of the study. The SPSS computer program (SPSS Inc., Chicago, IL, USA) was used for statistical analysis of the measured data by unpaired t-test for parametric data (expressed as a mean and standard deviation) and Fisher’s exact test for categorical data (expressed as a number and percent). Pain score, response to gag reflex, degree of swallowing, and parents’ satisfaction were assessed by the Mann-Whitney test. When the P value was less than 0.05, changes were considered significant.
4. Results
Along the nine months of the study, 111 patients were enrolled. Twenty-one were excluded (nine were not meeting the inclusion criteria and 11 declined participation). The remaining 90 patients were randomly allocated to either the control group or the glossopharyngeal nerve block group, with successful follow-up and analysis of the data of all patients (Figure 1). Differences in age, gender, body weight, and the ASA class of the studied patients between the two groups were statistically insignificant (P = 0.903, 0.662, 0.442, and 0.758, respectively). Also, the duration of the surgery was comparable between both groups (P = 0.362) (Table 1).

Figure 1.
CONSORT flowchart of the study
Table 1.
Demographic Data and the Incidence of Postoperative Complications in the Studied Groupsa
| Group C | Group G | P Value | CI (95%) | |
|---|---|---|---|---|
| Age, y | 5.956 ± 1.692 | 5.911 ± 1.743 | 0.903 | -0.764; 0.675 |
| Gender | ||||
| Male | 27 (60) | 30 (66.67) | 0.662 | 0.574; 1.315 |
| Female | 18 (40) | 15 (33.33) | ||
| Body weight, kg | 19.667 ± 3.323 | 19.067 ± 3.72 | 0.422 | -2.078; 0.8777 |
| Duration of the surgery, min | 22.556 ± 3.787 | 23.333 ± 4.264 | 0.362 | -0.912; 2.467 |
| ASA Class | ||||
| Class I | 40 (88.89) | 38 (84.44) | 0.758 | 0.609; 2.488 |
| Class II | 5 (11.11) | 7 (15.56) | ||
| Postoperative complications | ||||
| Nausea and vomiting | 8 (17.78) | 10 (22.22) | 0.798 | 0.492; 1.519 |
| Delayed hospital discharge | 0 | 0 | - | - |
| Choking | 4 (8.89) | 7 (15.56) | 0.522 | 0.312; 1.575 |
| Local anesthetic toxicity | 0 | 0 | - | - |
| Dry mouth | 9 (20) | 11 (24.44) | 0.800 | 0.512; 1.495 |
| Nasal obstruction | 4 (8.89) | 6 (13.33) | 0.739 | 0.355; 1.718 |
| Hoarseness of voice | 0 | 0 | - | - |
| Foreign body sensation in the throat | 12 (26.67) | 19 (42.22) | 0.183 | 0.421; 1.138 |
Abbreviation: CI, confidence interval.
aValues are expressed as mean ± SD or No. (%).
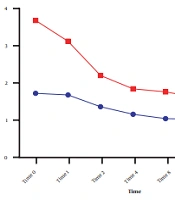
The time for the first request for pethidine rescue analgesia was significantly prolonged in the glossopharyngeal nerve block group compared to the control group (P < 0.0001). Moreover, the postoperative dose of pethidine consumed by the glossopharyngeal nerve block group was significantly lower than the control group (P = 0.0009). The postoperative pain score during rest (FLACC score) was statistically decreased in the glossopharyngeal nerve block group compared to the control group, at two, four, six, and 12 hours, respectively (P ≤ 0.0001, 0.0002, 0.0009, and 0.039, respectively). However, the FLACC pain score during rest was comparable between the two groups at 30 minutes, 18 hours, and 24 hours after surgery (P = 0.168, 0.791, and 0.464, respectively). In addition, the glossopharyngeal nerve block group showed significantly lower postoperative pain scores during swallowing compared to the control group, at two, four, and six hours postoperatively (P ≤ 0.0001, 0.0012, and 0.0013, respectively), with an insignificant difference between the two groups at 30 minutes, 12 hours, 18 hours, and 24 hours, postoperatively (P = 0.234, 0.197, 0.994, and 0.360, respectively) (Table 2).
Table 2.
The Postoperative Pain Score and Analgesic Consumption in the Two Groupsa
| Group C | Group G | P Value | CI (95%) | |
|---|---|---|---|---|
| Time for the first request to pethidine, h | 3.478 ± 2.116 | 5.833 ± 2.667 | < 0.0001b | 1.347; 3.364 |
| Postoperative consumption, dose of pethidine, mg/kg | 1.144 ± 0.347 | 0.878 ± 0.387 | 0.0009b | 0.1127; 0.421 |
| FLACC score during rest | ||||
| 30 min | 3 (2 - 7) | 3 (2 - 6) | 0.168 | |
| 2 h | 4 (3 - 6) | 3 (2 - 6) | < 0.0001b | |
| 4 h | 5 (3 - 7) | 4 (3 - 7) | 0.0002b | |
| 6 h | 5 (3 - 7) | 4 (3 - 7) | 0.0009b | |
| 12 h | 3 (2 - 6) | 4 (2 - 7) | 0.039b | |
| 18 h | 3 (1 - 4) | 3 (1 - 4) | 0.791 | |
| 24 h | 2 (1 - 4) | 2 (1 - 4) | 0.464 | |
| FLACC score during swallowing | ||||
| 30 min | 2 (1 - 6) | 1 (1 - 6) | 0.234 | |
| 2 h | 3 (1 - 6) | 2 (1 - 5) | < 0.0001b | |
| 4 h | 5 (3 - 7) | 4 (3 - 7) | 0.0002b | |
| 6 h | 3 (1 - 6) | 4 (1 - 6) | 0.0013b | |
| 12 h | 2 (1 - 5) | 3 (1 - 6) | 0.197 | |
| 18 h | 1 (0 - 3) | 2 (0 - 3) | 0.994 | |
| 24 h | 1 (0 - 3) | 1 (0 - 2) | 0.360 |
Abbreviation: CI, confidence interval.
aValues are expressed as mean ± SD or median (range).
bdenotes significant changes.
Postoperatively, in the post-anesthesia care unit, the response to gag reflex was significantly lower in the glossopharyngeal nerve block group than in the control group (P < 0.0001). Furthermore, glossopharyngeal nerve block significantly decreased the difficulty in swallowing compared to the control group (P = 0.006) (Table 3).
Table 3.
Postoperative Response to the Gag Reflex and Difficulty in Swallowing in the Recovery Rooma
| Group C | Group G | P Value | |
|---|---|---|---|
| Response to gag reflex (No. of patients) | < 0.0001b | ||
| None | 5 | 18 | |
| Mild | 8 | 17 | |
| Moderate | 19 | 5 | |
| Severe | 13 | 5 | |
| Difficulty in swallowing (No. of patients) | 0.006b | ||
| None | 9 | 15 | |
| Mild | 8 | 17 | |
| Moderate | 21 | 11 | |
| Severe | 7 | 2 |
aData are expressed as a No. of patients.
b Denotes significant changes.
Parents of the glossopharyngeal nerve block group were statistically more satisfied with postoperative analgesia given to their children than those of the control group (P = 0.0002) (Figure 2). The incidence of postoperative complications, including nausea and vomiting, choking, dry mouth, nasal obstruction, or foreign body sensation in the throat, was comparable between the two groups (P > 0.05). No cases of local anesthetic toxicity, postoperative hoarseness of voice, or delayed hospital discharge were reported in the two studied groups (Table 1).

Figure 2.
The parent’s satisfaction of the studied patients in the two groups. Data were expressed by the No. of patients and the degree of satisfaction.
5. Discussion
The results of this clinical study proved that the use of bilateral glossopharyngeal nerve block in children presented for adeno-tonsillectomy significantly prolonged the time for the first request of pethidine rescue analgesia. It also decreased the postoperative dose consumed of pethidine, postoperative FLACC score during rest and swallowing, and postoperative gag reflex and difficulty of swallowing. Moreover, glossopharyngeal nerve block significantly increased parents’ satisfaction, without increasing the incidence of complications.
The tonsillar and peritonsillar areas are supplied by sensory fibers from the glossopharyngeal nerve. Consequently, glossopharyngeal nerve block resulted in decreased postoperative pain after tonsillectomy and decreased analgesic consumption. The control of postoperative pain following adeno-tonsillectomy resulted in decreased morbidity and increased satisfaction (3, 11).
Hung et al. (14) studied the effect of topical bupivacaine or normal saline on postoperative analgesia in 99 adult patients undergoing tonsillectomy. They found that bupivacaine instillation was associated with better postoperative analgesia and early recovery. Naja et al. (15), in their randomized double-blinded study, reported that pre-incisional local anesthetic infiltration in children presented for tonsillectomy significantly decreased post-tonsillectomy pain and helped in better recovery of activities. Moreover, the systematic review of Grainger and Saravanappa (16) included 13 randomized studies that evaluated the effect of local anesthetic techniques on post-tonsillectomy pain. It was concluded that local anesthetic techniques were effective in controlling postoperative pain after tonsillectomy and decreasing postoperative analgesic consumption. Topical anesthesia was preferred as it was associated with a lower incidence of side effects.
In concordance with the current results, Mohamed et al. (17) compared the use of bilateral glossopharyngeal nerve block and preoperative dexamethasone (0.5 mg/kg I.V.) in children presented for tonsillectomy. They showed a significant prolongation in the absolute analgesia time, decreased values of postoperative pain score, and decreased difficulty in swallowing with the use of bilateral glossopharyngeal nerve block. Park et al. (18) studied 75 patients to evaluate the effect of bilateral glossopharyngeal nerve block with ropivacaine, bupivacaine, or no block, on post-tonsillectomy pain. They concluded that bilateral glossopharyngeal nerve block with ropivacaine or bupivacaine significantly decreased the postoperative pain score during rest and swallowing and obtunded the response to gag reflex. Also, there were no significant differences in postoperative nausea and vomiting, difficulty in swallowing, foreign body sensation in the posterior pharynx, dyspnea, nasal obstruction, or dry mouth among the studied groups.
In contrast to the current findings, El-Hakim et al. (19) studied 92 adult patients presented for tonsillectomy and concluded that glossopharyngeal nerve block with 0.5% bupivacaine was not effective in reducing early post-tonsillectomy pain. Their study found that patients in the bupivacaine group reported more severe pain the morning after surgery in comparison to the saline and no block groups. Moreover, the pain score over the entire postoperative period and the analgesic consumption were similar in the three groups. This study, however, was carried out on adult patients, which may explain the difference between its results and that of the current study. In addition, Violaris and Tuffin (20) evaluated the effect of topical infiltration of plain bupivacaine (0.5%) or normal saline on postoperative pain in adult patients presented for tonsillectomy. They revealed that topical infiltration of bupivacaine did not decrease the postoperative pain score or postoperative analgesic consumption. These discouraging results may be attributed to failure of local anesthetics to reach sensory nerve endings, as explained by the expanded case report by Naja et al. (11).
Bell et al. (21) evaluated the effect of bilateral glossopharyngeal nerve block on postoperative analgesia in adult patients undergoing tonsillectomy or uvulopalatoplasty. They reported similar postoperative pain scores with or without glossopharyngeal nerve block. Moreover, the tonsillectomy subgroup analysis revealed increased postoperative pain in the glossopharyngeal nerve block group in comparison with the no block group. This difference may be attributed to the fact that they have conducted their studies on adult patients. In addition, Kountakis (22) assessed the effect of local infiltration of either bupivacaine (0.5%) or normal saline on postoperative pain after tonsillectomy. They revealed an insignificant difference between the two groups. This difference may be explained by the use of standard tonsillectomy in their study instead of bipolar diathermy.
Limitations of this trial include the absence of evaluation of preoperative gag reflex. Postoperative absence of gag reflex may be due to its preoperative absence, which could be found in certain populations. On the other hand, the evaluation of the difficulty in swallowing and parents’ satisfaction was subjective and may depend on other factors, such as the effort exerted by the patients. Moreover, patients in the control group did not receive sham block, and thus the effect of the needle was absent. Another limitation was that pethidine was used for postoperative rescue analgesia. Despite the limitation on its use as a postoperative analgesic in many countries, it is used in Egypt owing to limited resources.
In conclusion, the use of bilateral glossopharyngeal nerve block with plain bupivacaine (0.25%) in children undergoing tonsillectomy significantly prolonged the time for the first call for pethidine rescue analgesia and decreased postoperative analgesic consumption and the postoperative pain score during rest and swallowing. Moreover, it decreased response to gag reflex and difficulty in swallowing and improved parents’ satisfaction, without a significant increase in the incidence of complications.