Control of pain and PONV after tonsillectomy is one of great significance for patients because most of these patients are children, and the pain in this group of patients can create an unfavorable mental background. This study aimed to assess the effects of a local injection of bupivacaine on postoperative pain and nausea vomiting after tonsillectomy, and the key result was that this way of administration of bupivacaine had a better analgesic effect and reduced PONV after tonsillectomy; thus, it might be reliably used for postoperative pain relief.
İhvan et al. found that bupivacaine caused significant pain relief at 2 and 6 hours after surgery compared to the control group, but no differences were shown at 24 hours after surgery (
9). In our research, however, the pain difference between the two groups continued 24 hours after surgery. This discrepancy may be because of a lower dose of bupivacaine or due to the different areas of injection. While the local effect of bupivacaine continues up to about 6 to 9 hours, such a long effect in our study (about 24 hours) may be due to the fact that the neural block by bupivacaine prevents sending pain impulses to the central nervous system immediately after the operation, reduces excitability resisting treatment, and is responsible for long postoperative pain relief.
Ozmen et al. compared the long-term effects of 0.25% and 0.5% bupivacaine on pain after tonsillectomy. They determined that patients’ pain was reduced even up to one week after taking the drug (
7). The results of their study are consistent with our findings.
The results of a study by Kadar and Obaid showed that the use of bupivacaine in tonsillar pills can reduce relief after surgery and provide the possibility of drinking and eating soon after operation (
10).
The results of Somdas et al. showed a significant difference in pain relief at the injection side of bupivacaine in the first 8 hours after administration (
11). The results of our study were consistent with the above findings.
Postoperative nausea and vomiting is an unpleasant experience that can lead to more serious complications, such as dehydration, electrolyte imbalance, the opening of surgical sutures, increased venous pressure, and so on (
12,
13). It also increases intracranial and ocular pressure and hospital costs (and delays the discharge of outpatients and inpatients) (
14,
15).
Various studies have examined the effects of various drugs such as intravenous dexamethasone, gabapentin, ketamine, morphine, lidocaine, bupivacaine, and ropivacaine as the main or complementary drugs to reduce pain, nausea, and vomiting. Among them, the effectiveness of lidocaine and bupivacaine was more popular due to their cheapness and availability (
16).
In the present study, at all the measurement times, the mean PONV scores were greater in the control group compared to the bupivacaine group (P < 0.05).
Costas-Gastiaburo et al. compared the effect of 0.5% of bupivacaine injection with bupivacaine compound with adrenaline and normal saline on the reduction of morbidities after tonsillectomy. Their results showed the highest incidence of nausea and vomiting among patients treated with bupivacaine alone (71.4%) (
17).
They explained that the impact was mostly due to the type of solution chosen. The results of their study did not agree with the present findings, which may be attributed to the differences in dose and combination of injected drugs.
Teunkens et al. compared bupivacaine and tramadol local administration on the pain and PONV after tonsillectomy. They concluded that there was less need to prescribe piritramide in the tramadol group. Furthermore, their study established no significant correlations between the incidence of post-operation nausea and vomiting and antiemetic need or associated complications (
18).
Faruk Cicekci investigated the correlation between levobupivacaine and levobupivacaine + adrenaline and pediatric tonsillectomy outcomes. Their results indicated that in both study groups, with the quantity of analgesic consumption 24 hours post-operation being equal, the participants experienced the same post-operation pain levels and PONV rates. In addition, the two groups were consistent in terms of time until the first oral consumption, time taken for recovery, and the time until they requested their first analgesic dose (
19). This was consistent with our results.
Ahmed El Daly, in a study with the effect of injection of local anesthetics on pain after tonsillectomy, they found that topical application of the tonsillar bed led to a significant reduction in postoperative throat pain (
1).
Regarding side effects, no special complications were observed in using bupivacaine in the peritonsillar area. Bean-Lijewski found an obstruction in the upper airway in the two cases (
20). They elucidated that this had been due to very deep injection and the blockage of the dendrites of the recurrent laryngeal nerve. This complication was not secondary to the type of injected drug (bupivacaine), and if any other drug was injected, this side effect could have occurred. The pain intensity and the amount of analgesic consumption of the two groups within 24 after the operation was compared. Duration of being pain-free, petedin need, and the time to start drinking liquids were significantly less in the bupivacaine group than the control group. This was consistent with our results.
4.1. Limitations and Recommendations
The first limitation of our study concerns the side effects associated with the peritonsillar injection of bupivacaine. For future studies, we recommend that other postoperative analgesics that are higher in quality and pose a lower risk of complications be used in tonsillectomy procedures. The second limitation was the lack of understanding of pain scores by some patients.
4.2. Conclusions
Preoperative local injection of 0.5% bupivacaine in tonsillectomy effectively reduced postoperative pain, opioid consumption, PONV in children. We recommend the prophylactic administration of bupivacaine before the beginning of tonsillectomy to achieve adequate postoperative analgesia and lesser PONV.
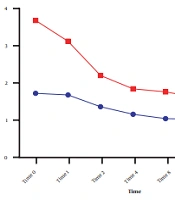







 score for the bupivacaine and control groups during 24 hours. Data are expressed as mean ± SD. The statistical test used was <i>t</i>-test. *P < 0.05 is considered as significant level. At all times, the mean VAS score in the control group was significantly higher than in the bupivacaine group (P < 0.001).")
.")
.")
