1. Introduction
Hairy cell leukemia (HCL) is a rare hematologic condition representing about 2% of all leukemias. The overall incidence of HCL is four times higher in males compared to females, with a median age at diagnosis of 55 years. Although it may be seen at a younger age, it is rarely diagnosed in children (1, 2). The onset of the disease is insidious, mostly chronic, and a large spleen (sometimes a giant spleen) is one of the characteristics of this disease (1, 3). The insidious onset and often non-specific symptoms of HCL, such as cytopenias and splenomegaly, frequently pose significant diagnostic challenges. Recent studies underscore the intricate interplay between chronic HBV infection, systemic inflammatory responses, liver changes, and their potential to confound hematologic diagnoses (4, 5). These challenges are particularly pronounced in regions like China, where HBV infection is highly prevalent and stands as the leading cause of cirrhosis (6). Chronic HBV-related liver disease commonly progresses to cirrhosis, often leading to portal hypertension, significant splenomegaly, and subsequent hypersplenism (7, 8). The resulting pancytopenia, conventionally attributed to hypersplenism secondary to cirrhosis, can tragically mask underlying hematological malignancies, including HCL, thereby leading to diagnostic delays and misdiagnosis. In this report, we present the case of a 38-year-old woman who was initially misdiagnosed with hepatitis B cirrhosis, splenomegaly, and hypersplenism but was eventually diagnosed with HCL. This case, therefore, serves as a critical reminder for clinicians to maintain a high index of suspicion for hematological malignancies in HBV-positive patients presenting with unexplained cytopenias and splenomegaly, even when classic signs of cirrhosis appear to explain the symptoms. We describe its clinical and pathological features in detail, providing a good reference for the early diagnosis of HCL.
2. Case Presentation
A 38-year-old woman, with a history of childhood hearing loss and chronic HBsAg positivity for 10 years without regular liver function monitoring, presented with a two-month history of abdominal pain and bloating, accompanied by five days of lower limb swelling. On admission, physical examination revealed a distended abdomen with mild muscle tension but no significant tenderness. The liver was not palpable, but the spleen was notably enlarged (A - B line: 16 cm; A - C line: 26 cm; C - D line: 15 cm). Shifting dullness was absent, bowel sounds were normal, and mild edema was observed in both lower extremities.
2.1. Laboratory Findings
Hematology showed pancytopenia: WBC 3.01 × 10⁹/L, hemoglobin 71 g/L, and platelets 72 × 10⁹/L. Coagulation studies revealed PT 12.6 s, APTT 46.9 s, D-dimer 2.38 mg/L, and FDP 7.08 μg/mL. Biochemistry indicated preserved liver synthetic function (albumin 34 g/L), with mildly elevated ALT (40 U/L) and AST (111 U/L), and LDH 363 U/L. Hepatitis markers were positive for HBsAg, HBeAg, and HBcAb, with HBV DNA at 2.65 × 10⁸ IU/mL. Iron studies showed reduced serum iron (2.9 μmol/L) and transferrin saturation (7%). Other parameters were within normal limits, and tests for occult blood, rheumatic immune markers, and urinary proteins were negative.
2.2. Imaging Findings
Abdominal ultrasound revealed diffuse intrahepatic lesions, a widened portal vein, and marked splenomegaly with irregular hypoechoic areas suggestive of splenic infarction. Contrast-enhanced upper abdominal CT confirmed splenomegaly with partial spontaneous splenic infarction (Figure 1).

Figure 1.
Contrast-enhanced CT scan of the upper abdomen
2.3. Bone Marrow Examination
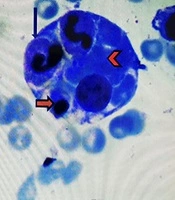
The initial bone marrow smear showed active proliferation of nucleated cells with increased blasts and granulocytic precursors, leading to a preliminary consideration of Myelodysplastic Syndromes with Excess Blasts (MDS-RAEB). The subsequent bone marrow biopsy confirmed myeloid hyperplasia with partial maturation abnormalities based on morphological and immunohistochemical findings (Figure 2A and B). The patient initially received entecavir for antiviral therapy along with liver protection and other symptomatic treatments. While some of her initial symptoms, such as abdominal discomfort, showed partial improvement, the massive splenomegaly persisted, and its underlying etiology remained elusive. Consequently, she was referred to the surgical department for further evaluation and treatment. During surgery, the spleen was markedly congested and massively enlarged (40 × 35 × 15 cm). A liver tissue biopsy showed a disorganized hepatic lobular structure. Histopathological examination of the liver revealed diffuse, invasive growth of monotonous lymphoid cells in the periportal and periductal areas. These tumor cells exhibited uniform morphology, characterized by distinctive coffee bean-shaped nuclei, clear cytoplasm, and fine chromatin (Figure 3A and B). Postoperative pathological examination of the resected spleen revealed diffuse infiltration of the red pulp by monotonous lymphoid cells. Characteristic "blood lakes" (pseudosinuses) were observed, associated with tumor cells displaying uniform morphology, distinctive coffee bean-shaped nuclei, clear cytoplasm, and fine chromatin. Based on these comprehensive morphological and immunohistochemical findings, the diagnosis was highly suggestive of HCL (Figure 4A and B). Following this diagnosis, the patient was strongly advised to undergo standard chemotherapy (e.g., purine nucleoside analogs). However, she refused further specific oncological treatment, primarily due to financial constraints and personal concerns regarding potential side effects. Despite this, the splenectomy provided significant symptomatic relief: her abdominal distension and pain resolved completely, and her peripheral blood counts showed transient improvement post-surgery. Unfortunately, without systemic therapy, the disease eventually progressed, and the patient passed away 20.3 months after initial presentation. Autopsy was not performed due to the family’s decision.
. Bone marrow proliferation and lymphoid infiltration were observed, initially suggesting MDS-RAEB. This finding highlighted a hematological disorder requiring further characterization, as it lacked definitive HCL morphology and contributed to the initial diagnostic challenge. B, Immunohistochemical staining for CD20 (400×). CD20-positive B-lymphoid proliferation in the bone marrow confirmed a lymphoproliferative disorder. However, without specific HCL morphology or additional markers, it was insufficient to distinguish HCL from other B-cell lymphomas or to definitively resolve initial MDS suspicion.")
Figure 2.
A, Bone marrow pathology: HE staining (400×). Bone marrow proliferation and lymphoid infiltration were observed, initially suggesting MDS-RAEB. This finding highlighted a hematological disorder requiring further characterization, as it lacked definitive HCL morphology and contributed to the initial diagnostic challenge. B, Immunohistochemical staining for CD20 (400×). CD20-positive B-lymphoid proliferation in the bone marrow confirmed a lymphoproliferative disorder. However, without specific HCL morphology or additional markers, it was insufficient to distinguish HCL from other B-cell lymphomas or to definitively resolve initial MDS suspicion.
. Diffuse sinusoidal infiltration of the liver by monotonous lymphoid cells, with distinctive coffee bean-shaped nuclei, highly suggests systemic HCL. This pattern is distinctly atypical for typical inflammatory infiltrates seen in HBV-related liver disease. B, Liver biopsy histopathology: Immunohistochemistry staining for CD20 (400×). Strong CD20 positivity confirms the B-cell lineage of the liver infiltrate with HCL morphology. This reinforces the HCL diagnosis and helps rule out non-lymphoid pathologies often seen in chronic liver disease.")
Figure 3.
A, Liver biopsy histopathology: HE staining (400×). Diffuse sinusoidal infiltration of the liver by monotonous lymphoid cells, with distinctive coffee bean-shaped nuclei, highly suggests systemic HCL. This pattern is distinctly atypical for typical inflammatory infiltrates seen in HBV-related liver disease. B, Liver biopsy histopathology: Immunohistochemistry staining for CD20 (400×). Strong CD20 positivity confirms the B-cell lineage of the liver infiltrate with HCL morphology. This reinforces the HCL diagnosis and helps rule out non-lymphoid pathologies often seen in chronic liver disease.
. Uniform monotonous lymphoid cells with characteristic HCL morphology diffusely infiltrate the red pulp. The pathognomonic \"blood lakes\" (pseudosinuses) provide definitive evidence for HCL, distinguishing it from other causes of splenomegaly (e.g., portal hypertension, other splenic lymphomas). B, Postoperative pathology of spleen: Immunohistochemical staining for CD20 (200×). Robust CD20 positivity, combined with the characteristic HCL morphology and \"blood lakes\" (<a href=\"#A168731FIG3\">Figure 3A</a>), definitively establishes the HCL diagnosis, ruling out non-B-cell lymphomas or non-hematologic causes of massive splenomegaly.")
Figure 4.
A, Postoperative pathology of spleen: HE staining (400×). Uniform monotonous lymphoid cells with characteristic HCL morphology diffusely infiltrate the red pulp. The pathognomonic "blood lakes" (pseudosinuses) provide definitive evidence for HCL, distinguishing it from other causes of splenomegaly (e.g., portal hypertension, other splenic lymphomas). B, Postoperative pathology of spleen: Immunohistochemical staining for CD20 (200×). Robust CD20 positivity, combined with the characteristic HCL morphology and "blood lakes" (Figure 3A), definitively establishes the HCL diagnosis, ruling out non-B-cell lymphomas or non-hematologic causes of massive splenomegaly.
3. Discussion
This case involved a 38-year-old woman, atypical for HCL, with a 10-year history of HBsAg positivity and congenital deafness. She presented with abdominal pain, bloating, lower limb swelling, and a significantly enlarged spleen, alongside pancytopenia and HBV DNA positivity. Based on diffuse liver lesions, portal vein dilation, and splenomegaly, a preliminary diagnosis of cirrhosis with secondary hypersplenism was made. At first glance, this seemed straightforward; furthermore, chronic HBV-induced inflammation and liver changes can directly affect bone marrow and splenic function, complicating differentiation from primary hematologic disorders. However, a deeper analysis raised questions. Despite massive splenomegaly, her liver function tests (ALB, ALT, AST) were normal, and coagulation function was intact, indicating preserved synthetic liver function. Imaging revealed spleen size exceeding that typically observed in cirrhotic portal hypertension, and her clinical presentation was inconsistent with conventional cirrhosis-related portal hypertension (9). These discrepancies suggested an alternative etiology. Consideration then shifted to other causes of non-cirrhotic portal hypertension, including hematological malignancies (e.g., acute leukemia, MDS, splenic lymphoma) and genetic/metabolic disorders (e.g., Niemann-Pick disease) (10). Ultimately, the pronounced splenomegaly, compression symptoms, and splenic infarction warranted splenectomy for both therapeutic and diagnostic purposes. Histopathological examination of the resected spleen confirmed HCL. This case underscores the diagnostic complexity of HCL, a rare hematological malignancy that can mimic other conditions, particularly those associated with splenomegaly and pancytopenia. These findings emphasize the importance of comprehensive evaluation and reconsideration of initial diagnoses when clinical and laboratory data are incongruent. The diagnostic journey of this patient illustrates the challenges often encountered in distinguishing HCL from other hematologic disorders. Specifically, the initial bone marrow examination misleadingly suggested Myelodysplastic Syndromes (MDS) due to the presence of proliferative nucleated cells and apparent maturation abnormalities. This misinterpretation can be attributed to the "dry tap" phenomenon often associated with HCL, caused by reactive reticulin fibrosis in the bone marrow (11). As noted in the NCCN guidelines (11), this fibrosis can result in suboptimal aspiration, where the few obtained hairy cells—with their oval nuclei and irregular cytoplasm—may be morphologically confused with blasts or dysplastic precursors seen in MDS. The definitive diagnosis in our case was eventually established through histopathological examination of the spleen, which corrected the initial error. The resection revealed the pathognomonic features of HCL: Diffuse infiltration of the red pulp, the formation of "blood lakes" (pseudosinuses), and cells with characteristic "bean-shaped" nuclei. Although advanced molecular testing (such as BRAF V600E mutation analysis) and flow cytometry markers (e.g., CD11c+, CD25+, CD103+, CD123+, and Annexin A1) are recommended by the NCCN to distinguish classic HCL (HCL-c) from HCL variant (HCL-v) or splenic diffuse red pulp lymphoma (SDRPL)11, the distinct splenic morphology combined with strong CD20 positivity in this patient provided sufficient evidence to support the diagnosis of HCL. A major drawback of this case was that molecular biology tests were not performed. However, in recent years, Kreitman RJ and other studies have confirmed that BRAFV600E mutations occur in more than 98% of HCL-c, while no BRAFV600E mutation was found in HCL-v, indicating that the BRAFV600E gene is a genetic marker of HCL (12, 13). While immunophenotyping and BRAF mutations are definitive for HCL, they are typically used only when malignancy is highly suspected (3, 14). Our case suggested that preserved synthetic liver function despite massive splenomegaly was a key differentiator. This case underscores that while molecular profiling is the gold standard, careful histopathological evaluation remains crucial, especially when bone marrow aspiration is inconclusive. Future research should explore specific serum biomarkers, flow cytometry, advanced imaging, or diagnostic applications like metabolomics as early, non-invasive screening tools. Regarding treatment, purine nucleoside analogs (PNA) such as cladribine or pentostatin remain the standard first-line therapy for HCL, inducing high rates of durable complete remission (15). In our case, although splenectomy is no longer considered a first-line treatment in the era of effective chemotherapy, it played a crucial role in diagnosis and palliation. The procedure successfully removed the massive splenic burden, resolving the patient's severe abdominal compression and hypersplenism symptoms. While the patient ultimately declined systemic chemotherapy due to economic factors, the splenectomy likely contributed to her survival of over 20 months by mitigating the immediate life-threatening complications of splenic rupture or severe cytopenias.