1. Background
Benign growths called uterine fibroids, or leiomyomas, originate from the uterus's smooth muscle layer and may extend either inside the uterus or outward into the pelvic cavity. They are highly prevalent, affecting up to 80% of women at some point in their lives, although many remain asymptomatic. Because of this, a considerable number of cases are discovered incidentally during routine gynecologic examinations or imaging studies such as ultrasound. Not all fibroids require medical or surgical intervention, as their clinical significance varies. They most commonly occur during the reproductive years and typically shrink or disappear after menopause (1).
According to many studies, uterine leiomyomas affect over 70% of women by the age of 50, and among African American women, the frequency increases to 80% (2). Based on regional epidemiological studies, the prevalence of uterine leiomyomas among Iranian women is estimated to be about 31%, depending on age group and diagnostic method, indicating a substantial national health burden comparable to global trends (3).
Uterine leiomyoma risk factors include age, vitamin D insufficiency, family history, prolonged time since previous delivery, obesity, use of soy milk or dietary supplements, and high blood pressure (4). Given that several metabolic and hormonal factors contribute to leiomyoma development, increasing attention has been directed toward the potential role of vitamin D deficiency as an additional, biologically plausible risk factor.
Uterine leiomyoma is a major cause of menstrual irregularities, which lower women's quality of life (5). Uterine leiomyomas account for 30% of all hysterectomies performed on women of reproductive age (6). The direct and indirect costs per patient range from 2,000 to 16,000 USD (7).
Although leiomyomas are typically benign and asymptomatic in certain patients, in 25% to 50% of cases, they can cause a variety of severe and persistent symptoms, including infertility, anemia, pelvic pressure and pain, abnormal uterine bleeding, gastrointestinal issues, and other obstetric complications. Currently, the main treatments for uterine leiomyomas involve surgical methods, including hysterectomy or myomectomy, which are costly. Alternative and preventive therapies are thus required, particularly for women who want to maintain their fertility (8, 9).
For uterine fibroids, a number of therapeutic options have been suggested, including surgery and pharmaceutical treatments such as gonadotropin-releasing hormone agonists, oral contraceptives, and nonsteroidal anti-inflammatory medications (10). Recent studies suggest that vitamin D supplementation may decrease the growth of uterine myomas. This is supported by multiple meta-analyses, which demonstrated that vitamin D supplementation significantly reduces fibroid size and improves serum vitamin D levels in women with uterine fibroids (11, 12). Consequently, vitamin D supplementation seems to be an effective treatment for leiomyoma. Vitamin D may influence leiomyoma development by regulating cell growth through the vitamin D receptor (VDR) in uterine tissue. It helps reduce fibrotic activity, modulates hormone-related pathways, and limits extracellular matrix buildup. These effects provide a clear biological basis for the link between vitamin D deficiency and fibroid growth (13). Recent studies have also highlighted the broader physiological importance of vitamin D across various clinical conditions, further emphasizing the need to clarify its potential role in uterine leiomyomas (14-16).
Recent systematic reviews and meta-analyses have reinforced the role of vitamin D in uterine fibroids. A 2023 review showed an inverse association between vitamin D levels and fibroid presence, with supplementation inhibiting growth (17). A 2024 meta-analysis confirmed a higher risk of deficiency in women with fibroids and significant reductions in fibroid size after supplementation (11). Another 2024 analysis of randomized trials also found that oral vitamin D improved serum levels and decreased fibroid size, especially with longer treatment durations (12). Although previous studies have examined vitamin D and uterine leiomyomas, their findings are inconsistent and often limited by small samples or inadequate control of confounders. There are also no data from Kurdish women, whose vitamin D status may differ due to regional lifestyle and sunlight exposure.
2. Objectives
This study aimed to address this gap by evaluating the association between vitamin D levels and leiomyomas in women from Kurdistan province.
3. Methods
3.1. Study Design
This case-control study was conducted at Besat Hospital, Sanandaj, from December 2021 to December 2022. The study population consisted of women of reproductive age diagnosed with uterine leiomyoma measuring ≥ 2 cm.
3.2. Participants
Eligible participants were women with uterine leiomyomas ≥ 2 cm confirmed by transvaginal or abdominal ultrasound. Exclusion criteria were prior myomectomy or hysterectomy, pregnancy, breastfeeding, abortion, metabolic disorders (renal dysfunction, hypothyroidism, diabetes), previous corticosteroid use, suspected sarcoma or other uterine malignancies, and intake of vitamin D supplements or hormonal therapy during the previous two years. Controls were recruited contemporaneously from the same hospital population and were required to have no leiomyoma or other uterine pathology on ultrasound. To reduce confounding by age, we aimed to recruit controls within a ±5-year age window (i.e., 5-year age strata) with an intended 1:1 case-control distribution; however, because recruitment was convenience-based, strict age matching could not be fully maintained, and a residual age difference remained between groups in the final sample (Table 1).
Table 1.
Baseline Characteristics, Reproductive History, and Family History of Participants a
| Variables | Control (n = 100) | Leiomyoma (n = 100) | P-Value |
|---|---|---|---|
| Age (y) | 33.92 ± 7.99 | 39.04 ± 5.19 | 0.001 |
| BMI (kg/m²) | 27.20 ± 3.93 | 32.26 ± 2.83 | 0.001 |
| Age at menarche (y) | 13.62 ± 0.90 | 13.66 ± 1.27 | 0.85 |
| Age at first pregnancy (y) | 21.97 ± 4.88 | 20.41 ± 5.76 | 0.14 |
| Serum 25-hydroxyvitamin D (ng/mL) | 26.46 ± 13.29 | 19.96 ± 10.78 | 0.009 |
| Leiomyoma size (mm) | 0 | 58.28 ± 22.83 | |
| Family history of leiomyoma | 11 | 18% | P > 0.05 |
| History of infertility | 3 | 9% | P > 0.05 |
a Values are as expressed as precent or mean ± SD.
3.3. Participants Section
To ensure consistency, all participants in the case group had at least one leiomyoma measuring ≥2 cm, which served as the standardized minimum threshold for inclusion.
3.4. Sample Size and Sampling
Based on the mean serum 25-hydroxyvitamin D levels reported in previous studies, and considering a 95% confidence interval and 80% statistical power, the required sample size was calculated using the following formula (18, 19):
σ1 and σ2: These represent the standard deviations of the two groups. They indicate the variability or spread of the data within each group.
µ1 and µ2: These represent the means of the two groups. They indicate the average values for each group.
n = (7.84) [(7.9)² + (6.1)²] / (26.1 − 15.1)²
n = (7.84) [99.49] / (121) 70
To account for potential variability in serum vitamin D levels and to increase the statistical power and precision of our estimates, we recruited 100 participants per group (200 total), exceeding the minimum required sample size of 70. Although the calculated minimum sample size was 70 per group, previous studies have reported considerable heterogeneity in vitamin D levels; therefore, increasing the sample size reduced the likelihood of type II error. Recruitment was performed using a convenience sampling method.
3.5. Data Collection
Demographic and clinical data (age, marital status, education, place of birth, income) were obtained via structured interviews by a gynecology resident. In the case group, leiomyoma size and volume were measured using both transvaginal and abdominal probes. All ultrasound examinations were performed by a single experienced radiologist to ensure consistency and eliminate inter-observer variation. Leiomyoma was defined as a well-circumscribed, symmetric, hypoechoic, and heterogeneous lesion.
Blood samples (≈12 mL) were collected from all participants in the morning (8 - 10 AM) to reduce diurnal variation. Samples were drawn by venipuncture, centrifuged, and the serum was stored at –20°C until analysis. Serum 25-hydroxyvitamin D levels were measured using the Arya Mabna Teb enzyme-linked immunosorbent assay kit (Iran), with a measurement range of 5–150 ng/mL and analytical sensitivity of ≈2 ng/mL. Vitamin D status was categorized as deficient (< 12 ng/mL), insufficient (12 - 20 ng/mL), and sufficient (≥ 20 ng/mL) (18).
Sunlight exposure was measured using the SEM-Q questionnaire, which has established validity and reliability in its original form. The Persian version was translated using a standard forward–backward procedure and was reviewed by experts, confirming that it was suitable and understandable for our study population (20).
3.6. Statistical Analysis
Continuous variables were summarized using mean ± standard deviation [or median (IQR) when appropriate], and categorical variables using number (percentage). Between-group comparisons were performed using the Student's t-test (or Mann-Whitney U test for non-normally distributed data) for continuous variables and the chi-square test (or Fisher's exact test) for categorical variables. The association between vitamin D deficiency and insufficiency (serum 25-hydroxyvitamin D < 20 ng/mL) and the presence of uterine leiomyoma was evaluated using univariable logistic regression, and results are presented as crude odds ratios (ORs) with 95% confidence intervals (CIs). Statistical significance was defined as a two-sided P < 0.05. Analyses were conducted using Stata (StataCorp, College Station, TX, USA). Because of the modest sample size, multivariable models including several covariates could yield unstable estimates; therefore, we report crude associations. Future studies with larger samples should confirm these findings using fully adjusted models.
4. Result
When compared to the control group, the leiomyoma group's mean age was much greater (39.04 ± 5.19 vs. 33.92 ± 7.99 years, P < 0.05). Comparisons between the leiomyoma and control groups in Table 1 were performed using the Student's t-test for continuous variables and the chi-square test for categorical variables. The mean Body Mass Index (BMI) differed significantly between groups (32.26 ± 2.83 vs. 27.20 ± 3.93 kg/m², P < 0.001). Similarly, no significant differences were observed in the mean age at menarche (13.66 ± 1.27 vs. 13.62 ± 0.90 years) or age at first pregnancy (20.41 ± 5.76 vs. 21.97 ± 4.88 years).
The group with leiomyoma had a considerably lower mean blood vitamin D level than the control group (19.96 ± 10.78 vs. 26.46 ± 13.29 ng/mL, P = 0.009). In the leiomyoma group, the mean fibroid size was 58.28 ± 22.83 mm. A family history of leiomyoma was reported in 18 patients in the leiomyoma group and 11 in the control group, with no statistically significant difference (P > 0.05). A history of infertility was observed in 9 women with leiomyoma and 3 controls, also without a significant difference (P > 0.05). Although controls were recruited within the intended ±5-year age window, a residual age imbalance remained between groups in the final sample (Table 1).
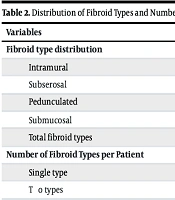
Descriptive statistics were used to summarize the distribution and frequency of fibroid types, and percentages were calculated for categorical variables without inferential statistical testing for Table 2. Regarding fibroid characteristics, the most frequent type was intramural (40.8%), followed by subserosal (32.4%), pedunculated (16.9%), and submucosal (9.9%). Because some women presented with two concurrent fibroid types, the total number of recorded fibroid types exceeded the number of patients. Among women with leiomyoma (n = 100), 58 (58%) had a single fibroid type, while 42 (42%) had two fibroid types simultaneously (Table 2). No statistically significant association was found between fibroid type and vitamin D levels (P = 0.63, Fisher's exact test) (Table 3). Likewise, the number of fibroids per patient was not associated with vitamin D levels (P = 0.60) (Table 4).
Table 2.
Distribution of Fibroid Types and Number of Fibroid Types per Patient
| Variables | Precent |
|---|---|
| Fibroid type distribution | |
| Intramural | 40.8 |
| Subserosal | 32.4 |
| Pedunculated | 16.9 |
| Submucosal | 9.9 |
| Total fibroid types | 100 |
| Number of Fibroid Types per Patient | |
| Single type | 58 |
| Two types | 42 |
Table 3.
Association Between Fibroid Type and Serum Vitamin D Status a
| Fibroid Type | Vitamin D < 20 ng/mL | Vitamin D ≥ 20 ng/mL |
|---|---|---|
| Intramural | 36 (66.7) | 18 (33.3) |
| Subserosal | 4 (50.0) | 4 (50.0) |
| Pedunculated | 14 (58.3) | 10 (41.7) |
| Submucosal | 6 (42.9) | 8 (57.1) |
a Values are as expressed as No (%).
Table 4.
Association Between Fibroid Burden (Number of Fibroids and Number of Fibroid Types) and Serum Vitamin D Status Among Women with Leiomyoma a
| Fibroid Category | Vitamin D < 20 ng/mL | Vitamin D ≥ 20 ng/mL | P-Value | OR (95% CI) |
|---|---|---|---|---|
| Number of fibroids | ||||
| 1 | 24 (70.6) | 10 (29.4) | ||
| 2 | 8 (66.7) | 4 (33.3) | ||
| 3 | 8 (44.4) | 10 (55.6) | ||
| 4 | 6 (42.9) | 8 (57.1) | ||
| Fibroid type (single vs. multiple) | 0.73 | 0.81 (0.26 - 2.55) | ||
| Single fibroid type | 36 (62.1) | 22 (37.9) | ||
| Two fibroid types | 24 (57.1) | 18 (42.9) |
a Values are as expressed as No (%).
For Table 5, comparisons of fibroid volume and serum vitamin D levels were analyzed using a non-parametric test (Mann-Whitney U test), as reflected by the reported Z-values. However, vitamin D deficiency (< 20 ng/mL) was significantly associated with the presence of leiomyoma. We dichotomized vitamin D status at 20 ng/mL because this cut-point is commonly used to define deficiency in clinical guidance and reference reports, enabling clinically interpretable comparisons with prior literature (21). Women with low vitamin D had a 3.5-fold higher unadjusted risk of leiomyoma (OR = 3.5, 95% CI: 1.36 - 8.99, P = 0.008). Because age and BMI are known confounders linked to both vitamin D deficiency and leiomyoma risk, cases and controls were age matched, and the reported ORs are presented as crude (unadjusted) estimates. Furthermore, women who were vitamin D deficient had a considerably greater mean fibroid volume than women who were adequately vitamin D enriched (236,757 ± 250,416 mm³ vs. 41,602 ± 65,573 mm³, P = 0.003) (Table 5).
Table 5.
Association of Vitamin D With Leiomyoma Presence and Fibroid Volume a
| Outcome and Vitamin D Status | Values | Statistical Test | P-Value | OR/Effect Size |
|---|---|---|---|---|
| Proportion of leiomyoma | Chi-square | 0.008 | OR = 3.5 (95% CI: 1.36 - 8.99) | |
| < 20 ng/mL | 60 | |||
| ≥ 20 ng/mL | 40 | |||
| Proportion of control group | ||||
| < 20 ng/mL | 16 | |||
| ≥ 20 ng/mL | 84 | |||
| Fibroid volume (mm³) | ||||
| < 20 ng/mL | 250,416 ± 236,757 | Z = 2.9 | 0.003 | |
| ≥ 20 ng/mL | 65,573 ± 41,602 |
a Values are as expressed as precent or mean ± SD.
In Table 6, differences in mean fibroid volume and mean serum vitamin D levels across fibroid types were evaluated using one-way analysis of variance. No significant associations were found between fibroid volume and fibroid type (P = 0.31) or between vitamin D levels and fibroid type (P = 0.31, Table 6).
Table 6.
Fibroid Volume and Serum Vitamin D Levels Across Fibroid Types a
| Fibroid Type | Fibroid Volume (mm³) | Serum Vitamin D (ng/mL) |
|---|---|---|
| Intramural | 212,121 ± 215,352 | 23.73 ± 11.36 |
| Subserosal | 5,234 ± 29,411 | 29.95 ± 15.07 |
| Pedunculated | 248,691 ± 281,650 | 27.12 ± 15.55 |
| Submucosal | 7,680 ± 34,817 | 33.86 ± 14.89 |
| Overall test | F = 3.17, P = 0.34 (volume) | F = 1.22, P = 0.31 (vitamin D) |
a Values are as expressed as mean ± SD.
5. Discussion
Because uterine leiomyoma is so common in premenopausal women and there is currently no safe and efficient non-surgical therapy, managing it is still difficult. This condition imposes a considerable financial burden on healthcare resources worldwide (22, 23). At present, hysterectomy is the main treatment option for uterine leiomyoma, and after cesarean section, it is one of the most common surgical procedures in women. However, surgery is not always an ideal choice, particularly for women who wish to preserve their fertility. Thus, creating a non-surgical, safe, and successful treatment plan is essential for women's healthcare (24).
Numerous studies have shown that vitamin D insufficiency is linked to the development and growth of leiomyomas, especially following menopause (15, 25). In an Iranian study, Hajhashemi and Ansari examined the effect of vitamin D supplementation in women with vitamin D deficiency on fibroid size. Following 10 weeks of supplementation, the intervention group's fibroid size decreased and their blood vitamin D levels were noticeably greater than those of the control group. This study suggested that vitamin D deficiency may be associated with the prevalence of uterine leiomyomas (13). Other studies have also reported that the incidence of uterine leiomyomas is approximately 32% lower among women with normal vitamin D levels (26). Similar to this, our results showed that uterine leiomyomas may form in women who are vitamin D deficient, likely because inadequate vitamin D reduces its regulatory effects on cell proliferation, extracellular matrix production, and hormonal signaling pathways in myometrial tissue. These biological mechanisms may allow unchecked fibroid growth in women with low vitamin D levels.
In a case-control study on 24 women, the mean vitamin D level was significantly lower among patients with uterine leiomyomas, although there was no association with fibroid size or volume (27). Another study on 90 women found that vitamin D concentration was significantly lower in leiomyoma patients compared to controls, and fibroid size increased proportionally with decreased vitamin D levels (19). By contrast, Mitro and Zota found no connection between vitamin D levels and leiomyoma risk, likely due to differences in study design, population characteristics, and inadequate control of confounding factors such as BMI and seasonal variation (28).
Srivastava et al. evaluated 25-hydroxyvitamin D3 levels in women with and without uterine leiomyomas. The study included 90 participants (45 cases and 45 controls). Women with at least one fibroid ≥10 mm detected on ultrasound were included as cases, while controls had no uterine pathology. Compared to controls, patients had substantially decreased serum 25-hydroxyvitamin D3 levels, and fibroid size rose in proportion to declining vitamin D levels. The study concluded that vitamin D3 deficiency is significantly associated with uterine leiomyoma, and this study supports a strong association between vitamin D deficiency and fibroid growth (19).
Farzaneh et al. conducted a case-control study in 2018 at Shahid Beheshti University of Medical Sciences, Tehran, Iran, to examine the relationship between serum vitamin D3 levels and uterine leiomyomas. Women with at least one ultrasound-confirmed leiomyoma ≥ 2 cm were included as cases, while controls had no uterine pathology based on transvaginal ultrasound. Serum vitamin D3 levels were measured using radioimmunoassay. Of 148 eligible participants, 71 had at least one uterine leiomyoma, while 77 had normal uterine structures. Serum 25-hydroxyvitamin D3 levels were significantly lower in leiomyoma patients than in controls. The study concluded that vitamin D3 deficiency may be a potential risk factor for uterine leiomyoma, and their findings suggest that vitamin D deficiency may be an important risk factor for leiomyoma among Iranian women (3).
In Turkey, Oskovi Kaplan et al. carried out a prospective observational cross-sectional study to assess the association between premenopausal women's blood 25-hydroxyvitamin D levels and their risk of developing uterine leiomyomas. 56 healthy women were compared to 68 women who had at least one fibroid measuring more than 10 mm. Serum vitamin D3 was measured using electrochemiluminescence immunoassay. The groups were similar in age, BMI, weight, and parity. Approximately 78% of patients had severe vitamin D deficiency. Although the case group's serum vitamin D levels were noticeably lower, there was no correlation between vitamin D levels and the size, volume, location, or number of fibroids. Oskovi Kaplan et al. also reported that factors such as conventional clothing style, lower education levels, and being a homemaker were associated with a higher risk of vitamin D insufficiency (27).
In a systematic review and meta-analysis, Mohammadi et al. investigated the relationship between serum vitamin D levels and uterine leiomyoma. Up to February 6, 2020, a thorough search of the databases PubMed, Scopus, EMBASE, Web of Science (ISI), Cochrane Library, Ovid, and Google Scholar revealed nine relevant studies with 1,730 individuals (835 leiomyoma cases and 895 controls)(28). According to the pooled study, which used a random-effects model, patients with uterine leiomyomas had considerably lower blood vitamin D levels than controls and showed that women with leiomyomas consistently had lower serum vitamin D levels than those without fibroids, reinforcing a robust overall association (29).
Overall, the study's findings imply that the incidence of uterine leiomyomas may be related to blood vitamin D levels. This result highlights the potential role of vitamin D deficiency not only as a correlating factor but also as a strong predictor of leiomyoma occurrence. Moreover, we found that mean fibroid volume was significantly larger in women with vitamin D deficiency compared with those with sufficient levels (236,757 ± 250,416 mm³ vs. 41,602 ± 65,573 mm³, P = 0.003). This suggests that vitamin D status may not only influence the presence of leiomyoma but also affect its growth dynamics. In line with several earlier reports (3, 19), our findings support the hypothesis that vitamin D has an inhibitory effect on fibroid progression.
In contrast, no statistically significant associations were observed between vitamin D levels and either fibroid type or fibroid number. This may suggest that vitamin D primarily influences leiomyoma development and enlargement rather than their anatomical characteristics. However, these non-significant findings should be interpreted with caution, as the study was not powered specifically to detect differences in fibroid type or number, and the subgroup sample sizes may have been insufficient to reveal smaller effect sizes. Similar results were reported by Oskovi Kaplan et al. (27), who also found no correlation between vitamin D status and fibroid size, number, or location.
5.1. Conclusions
Our findings indicate that vitamin D deficiency is significantly associated with both the presence of uterine leiomyomas and increased fibroid volume, although no associations were observed with fibroid type or number. These results suggest that vitamin D may play a meaningful role in the development and growth of leiomyomas and highlight the potential value of vitamin D supplementation as a preventive or therapeutic strategy. Nonetheless, the case–control design limits causal inference, and further prospective studies and randomized clinical trials are required to confirm these associations and clarify their clinical implications.
5.2. Study Limitations
As a case–control design, it cannot establish causality. Although we adjusted for age and BMI, other confounders — such as seasonal sunlight variation, diet, and recall bias in self-reported sunlight exposure — may still have influenced vitamin D levels. Because the sample size was calculated based on the primary outcome, the study was not specifically powered to detect smaller associations with secondary outcomes such as fibroid type or number; thus, these non-significant findings should be interpreted with caution. In addition, the study was conducted in a single region, which may limit generalizability. Furthermore, the use of convenience sampling is a significant limitation, as it affects the generalizability of the findings and may introduce selection bias.
5.3. Future Research Recommendations
Future studies should include larger, multicenter cohorts to improve generalizability and strengthen statistical power, particularly for analyzing fibroid subtypes and number. Longitudinal designs are needed to clarify causal relationships between vitamin D deficiency and leiomyoma development. Randomized clinical trials evaluating vitamin D supplementation could further determine its therapeutic or preventive potential. Future research should also assess genetic, lifestyle, and environmental factors that may modify the vitamin D–leiomyoma relationship.
