1. Background
Following the COVID-19 pandemic, telemedicine has shifted from an optional service to a strategic necessity for health systems; however, achieving sustainable and equitable implementation remains a global challenge (1). In practice, telemedicine enables remote clinical consultation, diagnosis, and treatment through information and communication technologies, with the potential to reduce travel burdens, improve the timeliness of care, and expand access for geographically or socially underserved populations (2, 3). Evidence from diverse settings further indicates that telemedicine can strengthen emergency response, disaster management, infectious disease control, and long-term follow-up for chronic conditions through virtual visits and remote monitoring (4, 5).
Despite these benefits, telemedicine implementation is not merely a technical deployment. It represents a multidimensional health system change that requires alignment across governance, financing, human resources, service processes, legal/ethical safeguards, and digital infrastructure (6-8). Earlier health information systems were often limited to administrative functions and localized institutional use (9), but advances in communication technologies have enabled service delivery beyond physical boundaries and across organizational networks (10). Consistent with the World Health Organization’s definition, telemedicine involves delivering health services through the exchange of diagnostic and therapeutic information and supporting workforce development using information and communication technologies (11). This definition underscores that telemedicine success depends on system readiness and coordinated service design, not technology alone.
Iran provides a salient case for international audiences because it reflects common constraints faced by many developing health systems, including unequal distribution of specialized services, high costs of patient transfers, and persistent access gaps outside major cities. However, telemedicine initiatives in such contexts often underperform not simply due to “need,” but because implementation remains fragmented, typically emphasizing isolated elements (e.g., infrastructure or individual applications) without a unified, prioritized strategic framework that links service planning, resources, coordination mechanisms, and quality control (8, 12). In Iran, this fragmentation contributes to discontinuity between policy intent and operational delivery, weak institutional coordination, and underspecified accountability mechanisms for financing, standards, and workforce preparation—conditions that increase the likelihood of partial adoption and program discontinuation (12, 13). In addition, limited strategic communication and digital health marketing to build public awareness and normalize telemedicine use may further exacerbate fragmented adoption and reduce uptake in Iran (30).
1.1. Related Works and Research Gap
Prior studies in Iran and comparable settings have identified multiple determinants of telemedicine development, including infrastructure readiness, legal considerations, cultural acceptance, and organizational capacity. For example, meta-syntheses and descriptive frameworks have reported extensive indicator lists and dimensions for telemedicine deployment (14). Other works conceptualize telemedicine as a dynamic process shaped by stakeholder networks and evolving life-cycle stages, emphasizing the importance of coordination among actors and resources (15-18). Sector-specific studies have also demonstrated telemedicine’s effectiveness in different medical domains and crisis contexts, including the COVID-19 period (19, 20). Recent evidence further reinforces the systemic and contextual nature of telemedicine implementation. Studies highlight the central role of financing, incentives, and intersectoral collaboration in healthcare responsiveness (21), alongside user- and provider-level barriers such as insurance coverage, digital literacy, and guideline gaps in specialized services such as teleoncology (22). Evidence from telecardiology and heart failure programs shows mixed clinical impacts, particularly in the short term (23, 24). Consensus-based frameworks stress monitoring and evaluation while revealing unresolved challenges related to reimbursement and change management (25). Moreover, patterns of service overutilization linked to chronic conditions and insurance design underline the importance of aligning telemedicine policies with utilization management strategies (26). Nevertheless, much of this literature remains descriptive or focuses on single dimensions and does not provide decision-ready guidance on (i) how these components causally interact and (ii) which factors should be prioritized first to improve access.
2. Objectives
To address this gap, telemedicine implementation is framed as an interdependent decision problem requiring a method capable of capturing cause–effect relationships and deriving stable priority weights within a networked system. Therefore, the present study employs a mixed-methods design to (a) identify components through expert interviews and thematic analysis and (b) causally structure and prioritize these components using the DANP approach (DEMATEL-based ANP), which integrates DEMATEL influence mapping with ANP weighting under interdependence (27). Accordingly, the primary objective of this study is to develop a comprehensive telemedicine framework and prioritize its components using a hybrid MCDM approach (DANP) to enhance access to health services in Iran. This objective aligns directly with the paper’s title (“Developing and Prioritizing”) and yields implementable priorities for policymakers and health managers.
3. Methods
3.1. Research Design
This applied study adopted a mixed exploratory (QUAL→QUAN) design. The qualitative phase aimed to identify context-specific telemedicine components affecting access to health services in Iran, whereas the quantitative phase prioritized these components using the DEMATEL-based Analytic Network Process (DANP), which is appropriate for interdependent multi-criteria decision problems.
3.2. Ethical Considerations
This study was approved by the Research Ethics Committee of Islamic Azad University (ethical approval code: IR.IAU.SRB.REC.1400.279) and involved human participants through professional expert interviews. No patients, clinical interventions, or personal health records were involved. Before data collection, all participants received written information regarding the study objectives, the voluntary nature of participation, confidentiality safeguards, and their right to withdraw at any time. Written informed consent was obtained from all participants before the interviews were conducted.
3.3. Qualitative Phase
3.3.1. Expert Selection and Inclusion Criteria
Experts were selected through purposive snowball sampling based on the following strict inclusion criteria:
1) A minimum of 10 years of professional experience in health services management, e-health/telemedicine, health policy, or healthcare systems governance;
2) Direct involvement in telemedicine or e-health implementation, evaluation, regulation, or strategic planning at hospital, university, or Ministry of Health levels;
3) Holding a senior managerial, policy-making, or academic position with decision-making or advisory responsibilities.
Experts without direct telemedicine-related strategic or managerial experience were excluded.
The final panel included experts in healthcare management, health policy, and e-health. Although all participants were male, this reflects the current gender distribution in senior decision-making positions accessible within the study context and is explicitly acknowledged as a limitation.
3.3.2. Sample Size and Theoretical Saturation
A total of 10 in-depth semi-structured interviews were conducted. Theoretical saturation was defined as the point at which no new codes, themes, or dimensions emerged and subsequent interviews yielded only confirmatory evidence. In this study, saturation was observed by interview 9; interview 10 was conducted to confirm the stability of the codebook and thematic structure.
Although prior methodological studies suggest that saturation often occurs between 12 - 17 interviews, recent qualitative research emphasizes that saturation is context-dependent and influenced by sample homogeneity, expert-level knowledge, and focused research questions. Given the high level of expertise, a shared policy context, and a targeted scope of inquiry, saturation was achieved with a smaller but information-rich expert panel (28).
3.3.3. Data Analysis and Qualitative Rigor
All interviews were audio-recorded with permission, transcribed verbatim, and analyzed using thematic analysis supported by MAXQDA (version 2018). The analysis followed a systematic six-step process:
1) Familiarization with the data through repeated reading;
2) Open coding to extract meaning units;
3) Axial coding to merge related codes into organizing themes;
4) Selective coding to finalize higher-order categories;
5) Development of a codebook defining each code, theme, and indicator;
6) Validation and reporting of themes aligned with the research question.
To enhance trustworthiness, the following strategies were used:
Credibility: Member checking was conducted by returning summarized findings and extracted themes (not raw transcripts) to participants for confirmation and clarification.
Dependability: An audit trail documented all coding decisions and refinements.
Confirmability: Reflexive memos and peer debriefing with an independent researcher were used to minimize subjective bias.
Transferability: A thick description of the context, expert profiles, and analytical procedures was provided.
Given resource constraints, formal inter-coder reliability statistics (e.g., Cohen’s Kappa) were not calculated; however, peer review of the codebook and thematic structure served as a methodological control.
3.4. Quantitative Phase: DANP Analysis
Based on the qualitative results, 24 indicators across five dimensions were analyzed using the DANP method. Experts evaluated the influence of factor i on factor j using a five-point linguistic scale (0 = no influence to 4 = very high influence). Mean values were used to construct the direct-relation matrix (M).
3.4.1. DEMATEL Procedure
The normalized direct-relation matrix (N) was calculated as:
The total-relation matrix was computed as:
A threshold value (α), equal to the average of the elements of matrix T, was applied to filter weak relationships and construct the Network Relationship Map (NRM). Indicators with (D−R) > 0 were classified as the cause group, and those with (D−R) < 0 as the effect group.
3.4.2. ANP Procedure and Convergence
Using the interdependencies derived from DEMATEL, the initial supermatrix was constructed and transformed into a weighted supermatrix. The weighted supermatrix was exponentiated until convergence, which was achieved at power k = 23, yielding a stable limit supermatrix. Final normalized weights were extracted from this matrix.
Because DANP relies on DEMATEL-derived influence matrices rather than traditional AHP pairwise preference judgments, the consistency ratio (CR) is not applicable in the same manner as in classic AHP. To mitigate respondent fatigue, experts evaluated influence relationships (rather than full reciprocal pairwise comparisons), substantially reducing the cognitive burden.
Full DEMATEL matrices, supermatrices, and convergence diagnostics are provided as supplementary materials (S1–S4) to ensure transparency and reproducibility.
3.4.3. Reliability and Validity
To assess reliability and stability, Equation 1 is used, where n denotes the number of criteria and p represents the number of experts. The aggregated value at level
4. Results
4.1. Qualitative Results
4.1.1. Coding Logic and Aggregation
Interview transcripts were first segmented into meaning units and assigned initial codes (open coding). Codes reflecting the same underlying concept (e.g., “patient privacy”, “data protection”, “cyber risk”) were merged during axial coding and labeled as a candidate indicator (e.g., Ensuring patient safety in cyberspace (E3)). Indicators were then grouped into organizing themes (e.g., E1–E4 → Service coordination (E)) through selective aggregation, guided by conceptual similarity and direct relevance to the research question (telemedicine components that improve access). This process yielded 24 indicators nested under five main categories (A–E) (Table 1 and Figure 1).
Table 1.
Demographic Characteristics of the Expert Participants
| Variables and Category | No. (%) |
|---|---|
| Age (y) | |
| 40 - 50 | 3 (30.0) |
| 50 - 60 | 5 (50.0) |
| 60 and above | 2 (20.0) |
| Gender | |
| Male | 10 (100.0) |
| Work experience (y) | |
| 10 - 20 | 5 (50.0) |
| 20 - 30 | 2 (20.0) |
| ≥ 30 | 3 (30.0) |
| Total | 10 (100.0) |

Figure 1.
Final output of qualitative data analysis of research components and indicators
4.1.2. Interpretation of Frequency Patterns
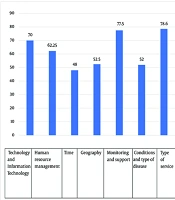
The frequencies in Tables 2 and 3 represent the salience and recurrence of concepts across expert narratives (i.e., how consistently experts emphasized a category/indicator) and were used to support theme stability and saturation, not to replace DANP weights. In Table 2, Service planning (Σ = 121) emerged as the most frequently referenced category, indicating that experts viewed planning activities (public education, ethical guidance, bandwidth readiness, needs assessment, goal-setting, and equity) as the most recurrent prerequisites for improving telemedicine access. Service coordination (Σ = 109) ranked second, reflecting strong emphasis on system-level alignment (legal gaps, standards, cybersecurity, and cost-related coordination). In contrast, Organizing (Σ = 85) and Resource allocation (Σ = 83) had lower cumulative frequencies, suggesting that while governance and financing are necessary, experts discussed them more as enabling conditions than planning and coordination.
Table 2.
Frequency Distribution of Coded Concepts in the Qualitative Analysis
| Code System | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | Σ (Sum) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Organizing | 7 | 14 | 25 | 4 | 6 | 10 | 5 | 2 | 3 | 9 | 85 |
| Proper allocation of financial and human resources | 10 | 3 | 5 | 4 | 1 | 2 | 6 | 7 | 21 | 24 | 83 |
| Service control | 7 | 14 | 10 | 11 | 6 | 3 | 14 | 2 | 11 | 9 | 87 |
| Service planning | 14 | 22 | 7 | 3 | 7 | 11 | 19 | 17 | 10 | 11 | 121 |
| Service coordination | 8 | 9 | 15 | 14 | 15 | 11 | 14 | 8 | 10 | 5 | 109 |
| Σ (Sum) | 46 | 62 | 62 | 36 | 35 | 37 | 58 | 36 | 55 | 58 | 485 |
Table 2 presents the aggregated coding results derived from the thematic analysis. Among the five main categories, Service Planning recorded the highest cumulative frequency (Σ = 121), followed by Service Coordination (Σ = 109) and Service Control (Σ = 87). The lowest frequencies corresponded to Proper Allocation of Financial and Human Resources (Σ = 83) and Organizing (Σ = 85). These findings indicate that experts perceived planning and coordination as the most critical components in developing a telemedicine framework to improve access to healthcare services in Iran
At the indicator level (Table 3), the high frequency of Identifying legal gaps and removing obstacles (E2; Σ = 45) indicates that legal/regulatory constraints were repeatedly framed as a bottleneck to scalable telemedicine access. Similarly, Explaining ethical guidelines (D2; Σ = 30) and Strengthening the image of telemedicine (A1; Σ = 29) highlight the perceived importance of trust-building mechanisms (ethics, legitimacy, and public confidence). Collectively, these patterns justify why the subsequent DANP phase focused on clarifying interdependencies among planning, coordination, and resource mechanisms rather than treating qualitative frequencies as priorities in themselves.
Table 3.
Theoretical Saturation Table of Indicators for the Design of the Telemedicine Service Management Model in Iran
| Code System | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | Σ (Sum) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Strengthening the image of telemedicine services | 4 | 9 | 6 | – | – | 7 | – | – | – | 3 | 29 |
| Cost-effectiveness of telemedicine services | – | – | 8 | 4 | 3 | – | 2 | 2 | – | 1 | 20 |
| Gaining patients' trust | 3 | 4 | 6 | – | – | – | 3 | – | – | 5 | 21 |
| Improving the culture of utilizing medical services among the general public | – | 1 | 5 | – | 3 | 3 | – | – | 3 | – | 15 |
| Financing services | – | – | – | – | – | – | 5 | 3 | 4 | 4 | 16 |
| Program-based budgeting | 4 | 1 | – | – | – | 2 | 1 | – | 6 | 4 | 18 |
| Considering incentives and bonuses for doctors and patients | 2 | 2 | 5 | 4 | 1 | – | – | – | – | – | 14 |
| Cost-effectiveness of programs | – | – | – | – | – | – | – | – | 4 | 14 | 18 |
| Reducing healthcare costs | 4 | – | – | – | – | – | – | 4 | 7 | 2 | 17 |
| Indirect monitoring of the quality and health of the services provided | 3 | – | 2 | 4 | 4 | – | – | – | 1 | 1 | 15 |
| Training doctors and telemedicine service providers | 4 | 8 | 4 | – | – | – | – | – | – | 3 | 19 |
| Improving customer satisfaction | – | 1 | 1 | 1 | – | 3 | 7 | 2 | 3 | 5 | 23 |
| Strengthening communication with customers in order to monitor services | – | 2 | 2 | – | 1 | – | 7 | – | 3 | – | 15 |
| Updating telemedicine facilities and services | – | 3 | 1 | 6 | 1 | – | – | – | 4 | – | 15 |
| Public education and awareness-raising regarding telemedicine | 3 | 1 | 2 | – | – | – | 1 | 3 | 2 | 2 | 14 |
| Explaining ethical guidelines in the field of telemedicine | 3 | 1 | 5 | 1 | 2 | 3 | 7 | 2 | 3 | 3 | 30 |
| Providing the required bandwidth in healthcare and medical centers | 4 | – | – | – | – | – | 2 | 5 | 3 | 3 | 17 |
| Consumer and customer needs assessment | 3 | 5 | – | – | – | 8 | 2 | 3 | 2 | – | 23 |
| Visioning and setting the right goals in the field of providing medical services | 1 | 14 | – | – | 5 | – | – | – | – | 1 | 21 |
| Increasing equity in access to medical services | – | 1 | – | 2 | – | – | 7 | 4 | – | 2 | 16 |
| Reducing the costs of telemedicine technology | 2 | – | 5 | 6 | 1 | – | 3 | 1 | – | 1 | 19 |
| Identifying potential legal gaps and removing obstacles to online medical services | – | 1 | 5 | 5 | 9 | 5 | 6 | 3 | 9 | 2 | 45 |
| Ensuring patient safety in cyberspace | 6 | 1 | 4 | – | 3 | – | 5 | 4 | 1 | 2 | 26 |
| Providing services based on existing service standards | – | 7 | 1 | 3 | 2 | 6 | – | – | – | – | 19 |
| Σ (Sum) | 46 | 62 | 62 | 36 | 35 | 37 | 58 | 36 | 55 | 58 | 485 |
As shown in Table 4, all respondents were male experts with considerable experience in health management or policy. “All experts were male, reflecting the accessible pool of senior managerial/policy roles during sampling; therefore, transferability should be considered with caution, and future studies should replicate the DANP panel with gender-diverse experts.”
Table 4.
Coding of Interview Outputs for Telemedicine Components and Improving Access to Health Services in Iran
| Symbol and Main Category | Subcategory |
|---|---|
| A | |
| Organizing | |
| A1 | Strengthening the image of telemedicine services |
| A2 | Cost-effectiveness of telemedicine services |
| A3 | Gaining patients' trust |
| A4 | Improving the culture of utilizing medical services among the general public |
| B | |
| Proper allocation of financial and human resources | |
| B1 | Financing services |
| B2 | Program-based budgeting |
| B3 | Considering incentives and bonuses for doctors and patients |
| B4 | Cost-effectiveness of programs |
| B5 | Reducing healthcare costs |
| C | |
| Service control | |
| C1 | Indirect monitoring of the quality and health of services provided |
| C2 | Training doctors and telemedicine service providers |
| C3 | Improving customer satisfaction |
| C4 | Strengthening communication with customers to monitor services |
| C5 | Updating telemedicine facilities and services |
| D | |
| Service planning | |
| D1 | Public education and awareness-raising regarding telemedicine |
| D2 | Explaining ethical guidelines in the field of telemedicine |
| D3 | Providing the required bandwidth in healthcare and medical centers |
| D4 | Consumer and customer needs assessment |
| D5 | Visioning and setting the right goals in providing medical services |
| D6 | Increasing equity in access to medical services |
| E | |
| Service coordination | |
| E1 | Reducing the costs of telemedicine technology |
| E2 | Identifying potential legal gaps and removing obstacles to online medical services |
| E3 | Ensuring patient safety in cyberspace |
| E4 | Providing services based on existing service standards |
Half of the respondents had 10 - 20 years of professional experience, whereas 20% had 20 - 30 years and 30% had over 30 years of experience.
This table presents the frequency distribution of 24 key indicators extracted from expert interviews. The results show that ethical and legal considerations—particularly explaining ethical guidelines, strengthening the image of telemedicine, and addressing legal gaps—were identified as the most influential factors in designing an effective telemedicine services management model in Iran.
After achieving theoretical saturation in the interviews, the qualitative data analysis was finalized. All coding, categorization, and thematic analysis processes were conducted using MAXQDA (version 2018). The final results included the extraction and classification of key components and indicators related to the telemedicine model and the enhancement of access to healthcare services in Iran.
The qualitative findings revealed five main components and twenty-four associated indicators that collectively represent the structural foundation of the proposed telemedicine service management model. These components were identified based on experts’ perspectives and validated through thematic saturation. The detailed outcomes of this analysis are summarized in Tables 2 and 3, which illustrate the frequency and significance of each component and indicator derived from the experts’ responses.
Figure 2- Final output of qualitative data analysis of research components and indicators
Analysis of interviews with ten health and medical experts led to the identification of a set of components that play a decisive role in shaping the telemedicine model and enhancing access to health services in Iran. These components were extracted through thematic coding and validated using expert consensus. The identified main categories and their corresponding subcategories are presented in Table 1.
4.2. Quantitative Results
After finalizing the qualitative coding process, the extracted components were analyzed quantitatively using the DANP technique to determine their interrelationships and relative importance.
The linguistic variables provided by the experts were first converted into corresponding numerical values. Aggregated expert opinions were obtained by calculating the arithmetic mean of their responses. The direct relationship matrix was normalized using the equation N = sM, where s represents the reciprocal of the maximum row or column sum, calculated from the experts’ average judgments. Subsequently, the total relationship matrix was derived based on the established interrelationships among the components. The results of this stage are presented in Table 5.
Table 5.
Results of the Full Correlation Matrix
| A1 | A2 | A3 | A4 | B1 | B2 | B3 | B4 | B5 | C1 | C2 | C3 | C4 | C5 | D1 | D2 | D3 | D4 | D5 | D6 | E1 | E2 | E3 | E4 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| A1 | 0.05 | 0.05 | 0.06 | 0.06 | 0.07 | 0.07 | 0.06 | 0.06 | 0.07 | 0.06 | 0.07 | 0.06 | 0.07 | 0.05 | 0.07 | 0.07 | 0.07 | 0.08 | 0.07 | 0.08 | 0.09 | 0.08 | 0.06 | 0.08 |
| A2 | 0.05 | 0.05 | 0.07 | 0.05 | 0.07 | 0.07 | 0.08 | 0.07 | 0.07 | 0.07 | 0.07 | 0.06 | 0.07 | 0.05 | 0.07 | 0.07 | 0.07 | 0.07 | 0.08 | 0.08 | 0.09 | 0.07 | 0.05 | 0.07 |
| A3 | 0.06 | 0.07 | 0.05 | 0.06 | 0.08 | 0.08 | 0.08 | 0.06 | 0.07 | 0.08 | 0.08 | 0.06 | 0.08 | 0.06 | 0.08 | 0.08 | 0.08 | 0.08 | 0.08 | 0.08 | 0.09 | 0.07 | 0.06 | 0.08 |
| A4 | 0.06 | 0.06 | 0.06 | 0.04 | 0.07 | 0.06 | 0.06 | 0.05 | 0.07 | 0.06 | 0.06 | 0.06 | 0.07 | 0.05 | 0.07 | 0.07 | 0.07 | 0.07 | 0.07 | 0.07 | 0.08 | 0.07 | 0.05 | 0.07 |
| B1 | 0.10 | 0.09 | 0.10 | 0.09 | 0.07 | 0.09 | 0.09 | 0.09 | 0.10 | 0.10 | 0.10 | 0.08 | 0.10 | 0.08 | 0.10 | 0.10 | 0.11 | 0.11 | 0.11 | 0.10 | 0.12 | 0.10 | 0.07 | 0.10 |
| B2 | 0.09 | 0.09 | 0.09 | 0.08 | 0.08 | 0.06 | 0.08 | 0.08 | 0.08 | 0.09 | 0.08 | 0.07 | 0.08 | 0.07 | 0.09 | 0.09 | 0.10 | 0.09 | 0.09 | 0.09 | 0.11 | 0.09 | 0.07 | 0.10 |
| B3 | 0.08 | 0.09 | 0.09 | 0.07 | 0.08 | 0.09 | 0.06 | 0.07 | 0.09 | 0.09 | 0.09 | 0.07 | 0.08 | 0.06 | 0.09 | 0.09 | 0.09 | 0.09 | 0.09 | 0.10 | 0.10 | 0.09 | 0.07 | 0.10 |
| B4 | 0.06 | 0.06 | 0.06 | 0.05 | 0.06 | 0.06 | 0.06 | 0.04 | 0.06 | 0.07 | 0.07 | 0.06 | 0.07 | 0.05 | 0.07 | 0.07 | 0.06 | 0.07 | 0.07 | 0.08 | 0.07 | 0.07 | 0.04 | 0.08 |
| B5 | 0.11 | 0.11 | 0.12 | 0.11 | 0.11 | 0.11 | 0.11 | 0.11 | 0.09 | 0.12 | 0.11 | 0.10 | 0.12 | 0.09 | 0.12 | 0.13 | 0.13 | 0.13 | 0.13 | 0.13 | 0.14 | 0.12 | 0.09 | 0.14 |
| C1 | 0.09 | 0.09 | 0.10 | 0.08 | 0.09 | 0.09 | 0.09 | 0.09 | 0.10 | 0.06 | 0.09 | 0.07 | 0.09 | 0.06 | 0.09 | 0.10 | 0.10 | 0.10 | 0.10 | 0.10 | 0.12 | 0.10 | 0.07 | 0.11 |
| C2 | 0.08 | 0.09 | 0.09 | 0.08 | 0.09 | 0.08 | 0.08 | 0.09 | 0.09 | 0.09 | 0.06 | 0.06 | 0.08 | 0.06 | 0.09 | 0.09 | 0.09 | 0.09 | 0.09 | 0.10 | 0.11 | 0.09 | 0.07 | 0.10 |
| C3 | 0.04 | 0.05 | 0.06 | 0.05 | 0.05 | 0.05 | 0.05 | 0.05 | 0.06 | 0.05 | 0.04 | 0.03 | 0.05 | 0.04 | 0.06 | 0.07 | 0.06 | 0.07 | 0.06 | 0.07 | 0.07 | 0.06 | 0.04 | 0.07 |
| C4 | 0.08 | 0.08 | 0.10 | 0.08 | 0.09 | 0.09 | 0.08 | 0.09 | 0.09 | 0.08 | 0.08 | 0.06 | 0.06 | 0.06 | 0.09 | 0.09 | 0.09 | 0.09 | 0.09 | 0.10 | 0.11 | 0.09 | 0.07 | 0.10 |
| C5 | 0.06 | 0.05 | 0.05 | 0.04 | 0.05 | 0.05 | 0.05 | 0.05 | 0.04 | 0.04 | 0.04 | 0.04 | 0.04 | 0.03 | 0.05 | 0.06 | 0.06 | 0.07 | 0.06 | 0.06 | 0.07 | 0.05 | 0.04 | 0.05 |
| D1 | 0.12 | 0.11 | 0.11 | 0.10 | 0.12 | 0.11 | 0.11 | 0.11 | 0.12 | 0.11 | 0.11 | 0.10 | 0.11 | 0.10 | 0.08 | 0.12 | 0.13 | 0.13 | 0.12 | 0.13 | 0.14 | 0.11 | 0.10 | 0.14 |
| D2 | 0.11 | 0.12 | 0.11 | 0.11 | 0.12 | 0.11 | 0.12 | 0.11 | 0.12 | 0.11 | 0.11 | 0.11 | 0.11 | 0.09 | 0.11 | 0.09 | 0.12 | 0.12 | 0.12 | 0.13 | 0.14 | 0.11 | 0.10 | 0.13 |
| D3 | 0.12 | 0.13 | 0.12 | 0.12 | 0.14 | 0.13 | 0.12 | 0.12 | 0.14 | 0.13 | 0.12 | 0.12 | 0.13 | 0.11 | 0.14 | 0.13 | 0.10 | 0.14 | 0.14 | 0.14 | 0.16 | 0.13 | 0.11 | 0.15 |
| D4 | 0.13 | 0.13 | 0.13 | 0.12 | 0.14 | 0.12 | 0.13 | 0.12 | 0.14 | 0.13 | 0.13 | 0.12 | 0.13 | 0.11 | 0.14 | 0.14 | 0.14 | 0.10 | 0.15 | 0.15 | 0.16 | 0.14 | 0.10 | 0.15 |
| D5 | 0.13 | 0.13 | 0.13 | 0.13 | 0.14 | 0.13 | 0.13 | 0.13 | 0.15 | 0.13 | 0.13 | 0.12 | 0.13 | 0.11 | 0.15 | 0.15 | 0.15 | 0.15 | 0.10 | 0.15 | 0.17 | 0.13 | 0.12 | 0.16 |
| D6 | 0.12 | 0.11 | 0.11 | 0.11 | 0.12 | 0.11 | 0.12 | 0.10 | 0.13 | 0.11 | 0.11 | 0.10 | 0.12 | 0.10 | 0.12 | 0.13 | 0.12 | 0.12 | 0.14 | 0.09 | 0.13 | 0.12 | 0.10 | 0.14 |
| E1 | 0.12 | 0.12 | 0.13 | 0.12 | 0.14 | 0.13 | 0.12 | 0.12 | 0.14 | 0.13 | 0.13 | 0.11 | 0.13 | 0.11 | 0.13 | 0.14 | 0.14 | 0.14 | 0.14 | 0.14 | 0.11 | 0.12 | 0.09 | 0.14 |
| E2 | 0.08 | 0.09 | 0.09 | 0.09 | 0.09 | 0.09 | 0.09 | 0.09 | 0.09 | 0.09 | 0.09 | 0.07 | 0.10 | 0.07 | 0.09 | 0.10 | 0.10 | 0.11 | 0.09 | 0.10 | 0.11 | 0.06 | 0.07 | 0.10 |
| E3 | 0.08 | 0.07 | 0.08 | 0.07 | 0.07 | 0.07 | 0.07 | 0.07 | 0.09 | 0.08 | 0.08 | 0.07 | 0.07 | 0.07 | 0.09 | 0.08 | 0.09 | 0.09 | 0.09 | 0.09 | 0.09 | 0.07 | 0.04 | 0.09 |
| E4 | 0.12 | 0.12 | 0.12 | 0.11 | 0.12 | 0.12 | 0.12 | 0.12 | 0.14 | 0.12 | 0.12 | 0.11 | 0.12 | 0.10 | 0.14 | 0.13 | 0.14 | 0.14 | 0.14 | 0.14 | 0.15 | 0.12 | 0.10 | 0.10 |
To enhance transparency and reproducibility, the Expert Opinions, the direct-relation matrix (M), and the normalized direct-relation matrix (N) are provided as Supplementary Tables (S1–S12). The initial, weighted, and converged (limit) supermatrices are also reported as Supplementary Table (S13-S15). In the main manuscript, Table 5 presents the total influence structure used to build the NRM and to generate ANP weights summarized in Table 6.
Table 6.
Final Global Normalized Weights of Categories and Indicators Organizing Telemedicine and Improving Access to Health Services in Iran a
| Symbol | Main Category | Category Weight | Category Rank | Symbol | Subcategory | Subcategory Weight | Subcategory Rank |
|---|---|---|---|---|---|---|---|
| A | Organizing | 0.1894 | 4 | A1 | Strengthening the image of telemedicine services | 0.0473 | 6 |
| A2 | Cost-effectiveness of telemedicine services | 0.0480 | 5 | ||||
| A3 | Gaining patients' trust | 0.0496 | 4 | ||||
| A4 | Improving the culture of utilizing medical services among the general public | 0.0445 | 7 | ||||
| B | Proper allocation of financial and human resources | 0.1985 | 3 | B1 | Financing services | 0.0404 | 9 |
| B2 | Program-based budgeting | 0.0392 | 13 | ||||
| B3 | Considering incentives and bonuses for doctors and patients | 0.0386 | 15 | ||||
| B4 | Cost-effectiveness of programs | 0.0376 | 17 | ||||
| B5 | Reducing healthcare costs | 0.0426 | 8 | ||||
| C | Service control | 0.1838 | 5 | C1 | Indirect monitoring of the quality and health of services provided | 0.0394 | 12 |
| C2 | Training doctors and telemedicine service providers | 0.0388 | 14 | ||||
| C3 | Improving customer satisfaction | 0.0342 | 23 | ||||
| C4 | Strengthening communication with customers to monitor services | 0.0399 | 11 | ||||
| C5 | Updating telemedicine facilities and services | 0.0315 | 24 | ||||
| D | Service planning | 0.2189 | 1 | D1 | Public education and awareness-raising regarding telemedicine | 0.0352 | 22 |
| D2 | Explaining ethical guidelines in the field of telemedicine | 0.0360 | 21 | ||||
| D3 | Providing the required bandwidth in healthcare and medical centers | 0.0365 | 19 | ||||
| D4 | Consumer and customer needs assessment | 0.0371 | 18 | ||||
| D5 | Visioning and setting the right goals in providing medical services | 0.0365 | 20 | ||||
| D6 | Increasing equity in access to medical services | 0.0377 | 16 | ||||
| E | Service coordination | 0.2093 | 2 | E1 | Reducing the costs of telemedicine technology | 0.0612 | 1 |
| E2 | Identifying potential legal gaps and removing obstacles to online medical services | 0.0508 | 3 | ||||
| E3 | Ensuring patient safety in cyberspace | 0.0403 | 10 | ||||
| E4 | Providing services based on existing service standards | 0.0570 | 2 |
a Cause–effect structure (NRM) based on (D-R).
After establishing the full correlation matrix, the initial supermatrix was constructed to represent the interrelationships among all criteria and sub-criteria within the telemedicine model. Subsequently, the weight matrix was calculated and multiplied by the initial supermatrix to obtain the weighted supermatrix. By raising the weighted supermatrix to successive powers and multiplying it by itself repeatedly, convergence was achieved, enabling extraction of the final normalized weights for each criterion. This iterative process continued until stability in the weight values was observed. The final results derived from this computation are summarized in Table 6. Based on the Reliability and Validity formula, the inconsistency rate was calculated as 0.0399, and because it is below the acceptable threshold of 0.05, the results demonstrate satisfactory reliability and stability.
Table 7presents the final DEMATEL results, where D denotes the influencing power (sum of row effects) and R represents the influenced degree (sum of column effects). Accordingly, D + R reflects the overall prominence (centrality) of each criterion within the system, whereas D − R identifies its net causal role: criteria with positive D − R values are classified as cause (driving) factors, and those with negative values are categorized as effect (dependent) factors. Based on these results, the cause group includes B5 (Reducing healthcare costs), D1 (Public education and awareness-raising regarding telemedicine), D2 (Explaining ethical guidelines in telemedicine), D3 (Providing the required bandwidth in healthcare and medical centers), D4 (Consumer and customer needs assessment), D5 (Visioning and setting the right goals in providing medical services), D6 (Increasing equity in access to medical services), E1 (Reducing the costs of telemedicine technology), E3 (Ensuring patient safety in cyberspace), and E4 (Providing services based on existing service standards). In contrast, criteria such as A3 (Gaining patients’ trust), C2 (Training doctors and telemedicine service providers), C5 (Updating telemedicine facilities and services), and E2 (Identifying potential legal gaps and removing obstacles to online medical services) fall into the effect group, indicating that they are more strongly influenced by other factors within the network. Finally, the DEMATEL influence matrix was filtered using a threshold value of 0.0931, retaining only relationships stronger than this cut-off for constructing the final causal diagram
Table 7.
Final Cause–Effect Matrix Indices
| Subcategory | D | R | D+R | D-R | type |
|---|---|---|---|---|---|
| A1 | 1.61 | 2.14 | 3.75 | -0.52 | effect |
| A2 | 1.63 | 2.16 | 3.79 | -0.54 | effect |
| A3 | 1.75 | 2.22 | 3.97 | -0.47 | effect |
| A4 | 1.53 | 2.01 | 3.53 | -0.48 | effect |
| B1 | 2.28 | 2.25 | 4.53 | 0.03 | cause |
| B2 | 2.05 | 2.17 | 4.22 | -0.13 | effect |
| B3 | 2.02 | 2.15 | 4.16 | -0.13 | effect |
| B4 | 1.50 | 2.10 | 3.60 | -0.60 | effect |
| B5 | 2.76 | 2.37 | 5.13 | 0.39 | cause |
| C1 | 2.17 | 2.19 | 4.35 | -0.02 | effect |
| C2 | 2.05 | 2.16 | 4.20 | -0.11 | effect |
| C3 | 1.30 | 1.92 | 3.22 | -0.62 | effect |
| C4 | 2.05 | 2.21 | 4.26 | -0.16 | effect |
| C5 | 1.21 | 1.77 | 2.99 | -0.56 | effect |
| D1 | 2.75 | 2.33 | 5.08 | 0.42 | cause |
| D2 | 2.72 | 2.39 | 5.11 | 0.34 | cause |
| D3 | 3.08 | 2.42 | 5.51 | 0.66 | cause |
| D4 | 3.14 | 2.45 | 5.59 | 0.69 | cause |
| D5 | 3.24 | 2.42 | 5.66 | 0.82 | cause |
| D6 | 2.78 | 2.49 | 5.26 | 0.29 | cause |
| E1 | 3.03 | 2.72 | 5.75 | 0.31 | cause |
| E2 | 2.16 | 2.26 | 4.42 | -0.09 | effect |
| E3 | 1.87 | 1.81 | 3.67 | 0.06 | cause |
| E4 | 2.95 | 2.54 | 5.50 | 0.41 | cause |
The DANP results (reported in the appendix) indicate that Service Planning (D = 0.2189) emerged as the most influential main component in the telemedicine system, followed closely by Service Coordination (E = 0.2093) and Proper Allocation of Financial and Human Resources (B = 0.1985). This ranking highlights the dominant role of forward-looking planning and coordinated service mechanisms over organizational and control-related dimensions. Overall, the findings emphasize that strategic planning and coordination functions are the core drivers shaping the effectiveness and sustainability of telemedicine development.
5. Discussion
This study employed a mixed-methods DANP approach not only to rank telemedicine components but also to uncover their causal structure within Iran’s health system. Unlike descriptive frameworks that list determinants of telemedicine success, the present findings clarify which factors drive others and how leverage points can be strategically sequenced. Accordingly, the discussion moves beyond reporting weights to interpreting systemic dynamics and situating them within the literature.
5.1. Planning as a Structural Driver Rather Than a Procedural Step
The predominance of Service Planning as the highest-priority and strongest causal dimension suggests that telemedicine implementation in Iran is primarily a governance and system-design challenge rather than a technological one. This aligns conceptually with the WHO telemedicine implementation guide (11), which emphasizes readiness, infrastructure alignment, and strategic integration into health systems. However, while the WHO provides normative guidance, our findings empirically demonstrate—through causal modeling—that planning-related indicators (D1–D6) function as upstream drivers influencing nearly all other dimensions.
Similarly, prior Iranian meta-analytic frameworks (e.g., Farah Abadi et al. (14)) identified multiple determinants of telemedicine deployment but did not specify their interdependencies or relative leverage. By contrast, our DANP results reveal that needs assessment (D4) and visioning/goal-setting (D5) exert the strongest causal effects, indicating that misalignment between telemedicine initiatives and population health priorities may be a primary explanation for program fragmentation reported in earlier national studies (1, 8). This finding extends the literature by shifting the focus from “what factors matter” to “which factors condition the effectiveness of others.”
Bandwidth availability (D3) further supports global evidence that digital infrastructure is a prerequisite for scalable telemedicine. Studies in telecardiology and digital heart failure management (23, 24) reported mixed clinical impacts in the short term, often linked to infrastructural constraints. Our results suggest that such variability may stem from insufficient upstream planning and infrastructure investment rather than limitations inherent to telemedicine itself.
5.2. Coordination as the Enabler of System Coherence
The second-ranked dimension, Service Coordination, indicates that affordability, standardization, and cybersecurity are enabling conditions for sustainable digital care. The high global weights of reducing technology costs (E1) and standard-based service provision (E4) suggest that economic and technical harmonization directly shape trust and adoption rates. This interpretation is consistent with Granja et al. (12), who found that lack of interoperability and coordination contributes significantly to eHealth failure.
However, our causal analysis refines this understanding by showing that cost reduction functions not merely as an economic factor but as a structural enabler that indirectly conditions legal compliance, patient trust, and service continuity. In resource-constrained environments, affordability becomes a gateway condition for legitimacy and scalability.
Legal gaps (E2), although frequently emphasized in qualitative narratives, were categorized as effect factors in the DEMATEL analysis. This nuance supports findings from change management research in telemedicine (27), which argues that regulatory reform alone rarely drives implementation success unless embedded within broader system planning and intersectoral coordination. Thus, the present model clarifies why isolated legal reforms often fail to produce large-scale transformation.
5.3. Resource Allocation and Control as Reinforcing Mechanisms
Contrary to some consensus-based telemedicine frameworks that prioritize monitoring and evaluation mechanisms (25), the present study finds that financial allocation and service control are largely responsive dimensions. Financing, incentives, training, and monitoring are essential for sustainability; however, their impact depends on prior clarity in goals, infrastructure readiness, and coordination mechanisms.
This interpretation resonates with Khanpoor et al. (21), who emphasized responsiveness and intersectoral collaboration in health systems. However, our model adds explanatory depth by demonstrating that such responsiveness mechanisms are conditionally activated by strong planning structures. In other words, resource mobilization without strategic alignment risks inefficiency.
5.4. Organizing and Trust as Downstream Outcomes
The relatively lower causal weight of the Organizing dimension, including trust-building and cultural acceptance, should not be misinterpreted as indicating insignificance. Rather, it suggests that, in Iran’s centralized and regulation-sensitive context, trust is not an initial driver but a consequence of visible system credibility. This aligns with findings from teleoncology research (22), where patient acceptance increased in environments with clear insurance coverage, clinical guidelines, and institutional backing.
International literature—especially from high-income settings—often highlights provider attitudes and organizational culture as primary adoption barriers. However, the present findings suggest that, in developing and infrastructure-variable systems, structural and governance factors precede cultural readiness. Trust appears to follow reliability, affordability, and regulatory clarity, not the other way around.
5.5. Contribution to the Broader Literature
Overall, this study both corroborates and extends prior research. It confirms that infrastructure, regulation, financing, and user acceptance matter, as widely reported (11, 12, 25). However, it advances the literature by empirically modeling their causal hierarchy. While previous studies have mapped determinants or proposed monitoring frameworks, few have quantified interdependencies and identified high-leverage intervention points in developing health systems.
By integrating qualitative insight with DEMATEL–ANP causal network analysis, this research demonstrates that telemedicine governance in contexts such as Iran requires a shift from fragmented, technology-driven initiatives toward integrated, planning-led system transformation. The findings therefore provide not only prioritization but also strategic sequencing, clarifying which reforms should precede others to maximize systemic impact.
5.6. Conclusions
This study developed and validated a context-specific telemedicine implementation framework for Iran using a mixed-methods design and DANP-based causal prioritization. The findings indicate that Service Planning is the most influential dimension for improving access, followed by Service Coordination and Resource Allocation, highlighting the primacy of upstream planning and system-level alignment in fragmented health systems. At the indicator level, the highest priorities were reducing telemedicine technology costs (E1), ensuring compliance with service standards (E4), addressing legal gaps and barriers (E2), and strengthening patient trust (A3). DEMATEL results further suggest that several planning and coordination indicators act as causal drivers, whereas trust, workforce training, and service updating are largely effect-oriented and improve once core structural conditions are addressed.
Based on these results, policymakers should prioritize needs assessment and goal-setting, bandwidth readiness, cost-reduction strategies, and national standardization, alongside targeted legal reforms and operational cybersecurity requirements. In parallel, the Ministry of Health should implement focused public education and trust-building programs, establish dedicated financing mechanisms, and deploy structured training and monitoring systems to sustain quality and equitable access. Overall, the proposed framework offers an evidence-based decision-support tool to guide phased, high-leverage telemedicine implementation in Iran and comparable developing health systems.
5.7. Practical Recommendations
Based on the prioritized DANP results and the causal structure of the model, the following high-leverage policy actions are recommended:
5.7.1. Strengthen Upstream Planning and Infrastructure Readiness
Institutionalize systematic needs assessment, clear strategic goal-setting, and equity-oriented planning, alongside prioritized investment in broadband and digital infrastructure for public hospitals and rural health centers.
5.7.2. Reduce Technology Costs and Standardize Services
Promote cost-reduction strategies through context-appropriate technology procurement (e.g., low-bandwidth solutions) and mandate national service standards and interoperability requirements to ensure scalability and quality.
5.7.3. Implement Targeted Legal and Ethical Reforms
Establish a coordinated regulatory task force to address legal gaps in online prescriptions, cross-regional practice, liability frameworks, and reimbursement mechanisms, while formalizing mandatory ethical and cybersecurity standards.
5.7.4. Establish Dedicated Financing and Incentive Mechanisms
Create ring-fenced telemedicine budget lines within national health plans and introduce incentive structures for providers to encourage sustainable adoption.
5.7.5. Develop Differentiated Capacity-Building Programs
Introduce structured training and certification programs for physicians, technical staff, and administrators, integrating telemedicine competencies into continuing medical education (CME) systems.
5.7.6. Institutionalize Monitoring, Trust-Building, and Public Engagement
Deploy centralized performance dashboards integrating patient feedback and service indicators, while implementing region-specific telemedicine literacy and communication strategies to enhance public trust and cultural acceptance.
5.8. Limitations and Future Research
This study has several limitations that should be considered when interpreting the findings. First, the qualitative coding process and the DANP method rely on expert judgment; despite triangulation and consensus procedures, some degree of subjectivity may have influenced the prioritization outcomes. Second, the expert panel consisted of ten participants, reflecting an in-depth exploratory design but limiting statistical generalizability. All experts were male due to access constraints to senior decision-making roles, which may restrict the transferability of the results to more gender-diverse contexts. Third, the cross-sectional design captures perceptions at a single point in time and does not account for evolving regulatory, technological, or policy dynamics that may alter telemedicine priorities. Finally, the limited availability of comparable national studies constrained opportunities for external validation and benchmarking.
Future research should replicate the proposed framework with larger and more diverse expert panels, including clinicians, informatics specialists, policymakers, and female healthcare leaders. Longitudinal studies are recommended to assess how telemedicine priorities shift over time in response to reforms or crises. Integrating hybrid decision-support methods (e.g., simulation modeling or machine learning approaches) could further enhance analytical robustness. Comparative cross-country studies would also help evaluate the contextual stability and adaptability of the model in different health system environments.
AI Use Disclosure: The authors declare that no generative AI tools were used in the creation of this article.