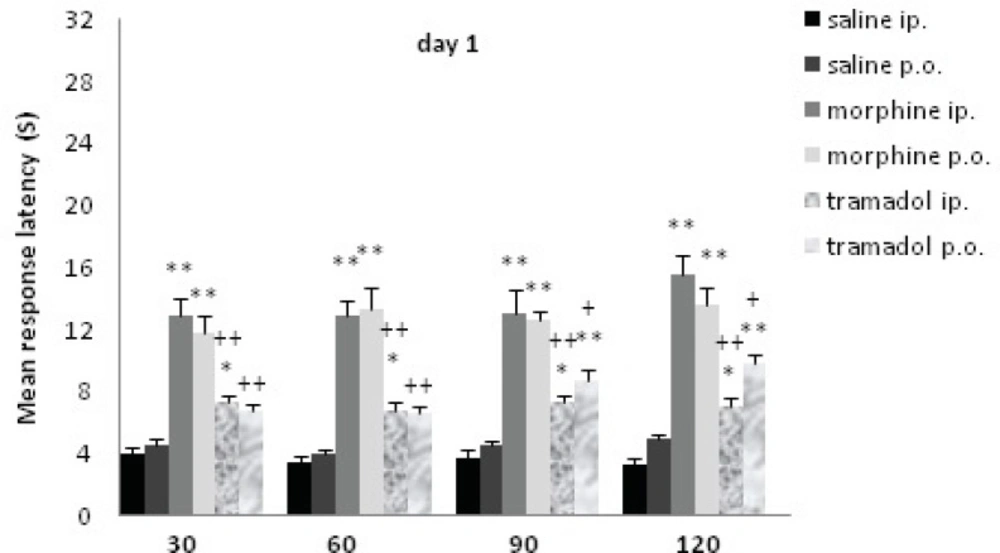
In the present study, the antinociceptive effect of tramadol, and morphine was investigated by using different methods of administrations at different time points. At d1 (acute dose 20 mg/Kg), while IP antinociceptive effect was greater than PO, there was no significant difference between method of drug administration (IP and PO) for morphine or tramadol groups. According to the previous findings, after intramuscular or subcutaneous injections, morphine plasma levels reach the peak in approximately 20 min, but after oral administration, its levels reach the peak in approximately 30 min(
40). Following oral administration of tramadol, it is rapidly and almost completely absorbed (
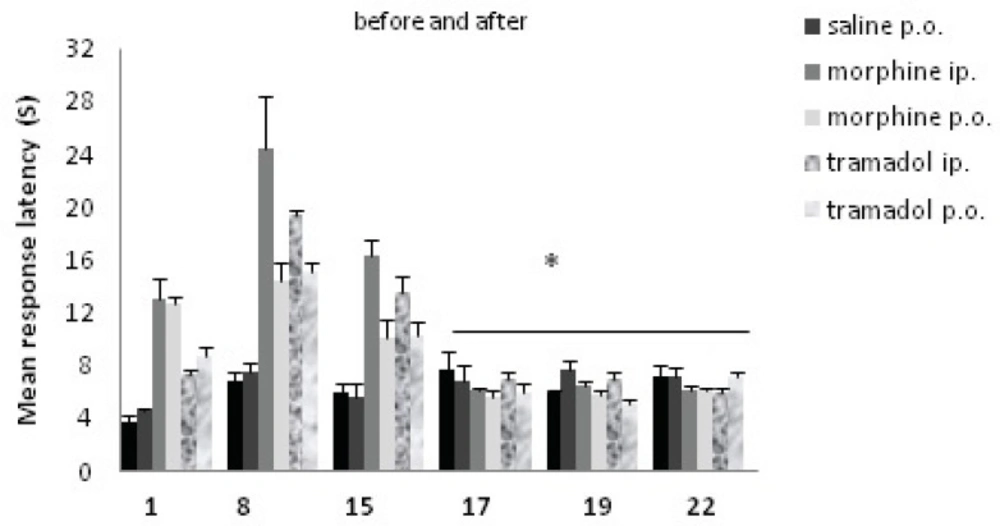
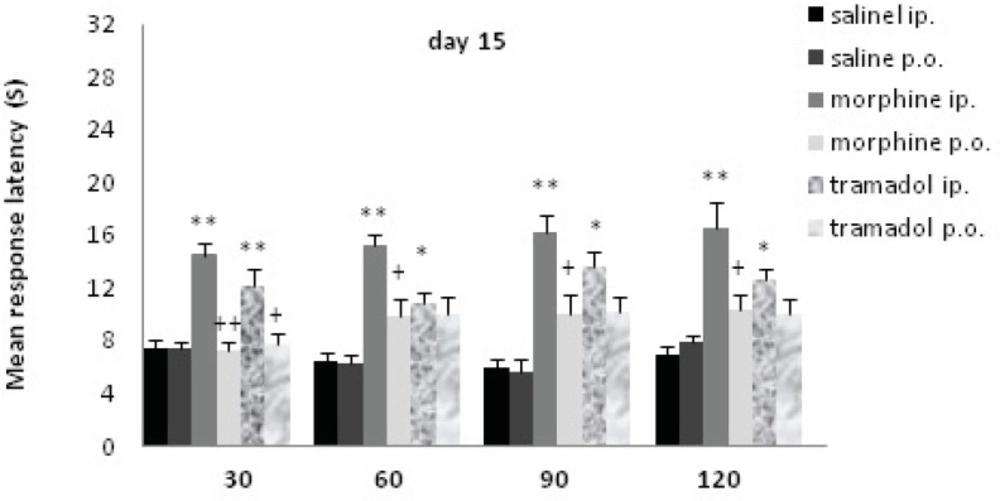
12). At d8 and d15, there was a significant difference between method of drug administration (IP and PO) for morphine or tramadol groups; IP administration showed an increase in the time of response latency comparing to the PO one.
Previous findings showed that in childhood, acute low dose of morphine (5 µg/Kg) subcutaneously inducted a significant antinociceptive responses, with a peak at 30 min, while in adulthood greater doses of morphine (5 mg/Kg) IP inducted a significant antinociceptive responses, at 30 and 60 min (
41). Also, it showed that in childhood repeated low dose of morphine (5 µg/Kg) subcutaneously inducted a significant antinociceptive responses, at 30, 60 and 90 min, while in adulthood repeated greater doses of morphine (5 mg/Kg) IP could not induct a significant antinociceptive responses(
41). Maintained study showed that all of the age, time, dose, method and repetition may be involved on morphine antinociceptive responses. Also, it has been demonstrated that morphine and tramadol have a dose-dependent effect that varies in different time points after drug administration (
41-
43). In this regard, there is also evidence that, the duration of analgesic effect of a single oral dose of tramadol 100 mg is about 6 hours (
44), peak analgesic effect is observed at 3.7 h (
43). Our study showed that at d1 (acute), while antinociceptive effect of tramadol IP did not change at two hours, PO administration showed a time-dependent effect (in 90 and 120 min). At d8 and d15 (chronic), PO administration of morphine and tramadol showed a time-dependent increase, an increase after 30 min, and this increase for tramadol inducted a significant difference between IP and PO administration after 30 min. So, it indicated that probably tramadol PO is more time-dependent than morphine and tramadol IP. At d8, the analgesic effect of morphine and tramadol (both IP and PO) was the most powerful one comparing to the other experimental days. Additive administration of the drugs is one reason for this effect at d8 comparing to d1 (
41). Also, in the rats and cats, over activation of opioid receptors have been observed to cause non-opioid receptor mediated hyperalgesia (
45). There is considerable evidence that the central pharmacological effects of morphine and tramadol can be interpreted as an interaction with one or more central transmitters; the synergy between antinociception effects of monoamines and opioids is well known (
46). In the rat, the threshold to nociceptive stimuli and its alteration by morphine is, in some way, depended on a dynamic balance of the concentrations of nor-adrenaline, and serotonin (5-HT) in the brain. Morphine stimulates 5-HT release via a supraspinal action (
47) 5-HT depletion in the CNS decreases the analgesic effect of morphine (
48), and nor-adrenaline antagonizes the antinociceptive effects of morphine. After tramadol administration, it increases the concentration of nor-adrenaline and 5-HT in brain areas (
23,
31). Our data is in line with these literatures, as it showed that analgesic effect of morphine and tramadol at d8 is stronger than d1. Our study indicated that, with the increasing of doses, there may not be tolerance at d8 to these drugs, but probably at d15 there would be a tolerance to them. There are several hypotheses about how morphine tolerance develops, including opioid receptor
phosphorylation which changes the receptor conformation, functional decoupling of receptors from
G-proteins which leads to receptor desensitization(
49), μ-opioid receptor internalization, receptor down-regulation, and up-regulation of the
cAMP pathway (
50). There is also evidence that long-term use of high doses of tramadol can induce
physical dependence, withdrawal syndrome, and tramadol-induced tolerance (
51,
52).At d17, d19, and d22, there was no antinociceptive effect for morphine or tramadol, and their effect has been disappeared. It seems that repeated morphine or tramadol administration for a moderately long period could not influence the antinociceptive effect of these drugs after their withdrawal. Therefore, there is no significant effect of either morphine or tramadol in 48 h or longer after withdrawal. By the cessation of morphine and tramadol, after 48 h, the drugs were effectively excreted from the body, and expectedly they do not show any analgesic effect. Confirming this data, morphine half-life is approximately 1.5 hours (
53). Urinary excretion of morphine and conjugation of morphine in the liver leads to 83% of the drug excretion from the body after the first day of use, with 11–14% of morphine later excreted in the bile(54). While for tramadol, the central analgesic effect of tramadol 100 mg orally is only partially reversed by the opioid antagonist naloxone, while α
2-adrenoceptor antagonism reverses tramadol effects, these point to the significant role of monoaminergic modulation and combination of μ-opioid agonist effects in tramadol antinociception after a single oral dose in human (
16). In previous studies challenge dose of tramadol 24 hours after chronic doses of tramadol (15 to 120 mg/Kg, s.c.) showed that chronic tramadol was still able to reduce [
3H]-5-HT uptake parameter by 42%. In contrast, 72 h after drug withdrawal, [
3H]-5-HT uptake in rats chronically-treated with tramadol did not differ significantly from control rats (
55).
In conclusion, our study indicated that analgesic effect of morphine and tramadol in acute dose (20 mg/Kg) was not significantly related to the method of administration (IP or PO), but after a chronic exposure, the method of administration showed significant difference (d8 and d15). Repeated morphine and tramadol administration inducted an increase in analgesic effect, it might gradually decrease and reach to the level compatible to d1 (at d15). Therefore, analgesic effect of morphine and tramadol was time-and-dose dependent, which was more visible in tramadol PO. Meanwhile, the present data indicated that chronic exposure to opiates might not lead to an altered nociceptive response until one week after drugs withdrawal. In case of chronic use of these drugs (as a pain killer), more caution must be paid in clinical administration.