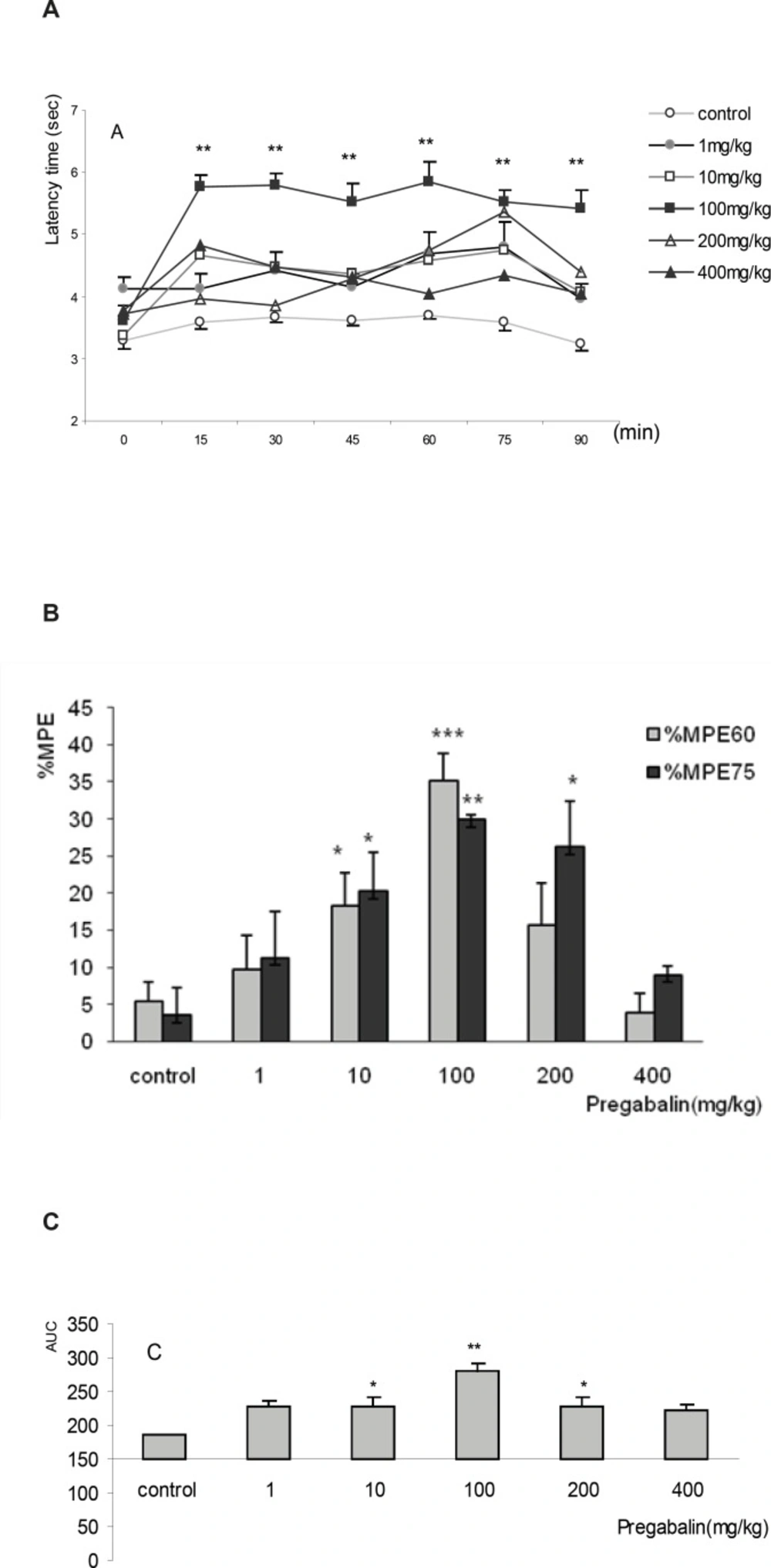
The results of this study showed the antinociceptive effect of pregabalin in tail flick test for the first time. The latency time increased from post injection time and the peak effect was observed at the 60
th and 75
th minutes. Maximum effect observed by 100 mg/Kg of pregabalin in terms of %MPE
60, was comparable to%MPE
60 of 50 and 80 mg/Kg of tramadol. The antinociception in this acute model of pain was not dose-dependent, although initially it increased as the dose was increased;however, subsequently, the antinociceptive effect reduced to the controlled levels. The decreased time response curve in tail flick test or the reduction of antinociceptive effect of pregabalin seen at 400 mg/kg could be due to its toxicity effect seen also in human clinical setting (
3,
6,
10). Effectively, the highest dose used in previoussimilar studies of pain assessment was 100 or at maximum 200 mg/kg in hot plate test (
7,
21-
22,
24-
27). Analgesic effect of pregabalin above these doses probably presents the same anomalies like decreased antinociceptionwhich we have also reportedin our study, although the nature of reflexive response mechanism of tail-flick may also be responsible. The explanation of this bimodal activity will be possible only after furtherstudies on pharmacokinetics and site of action of pregabalin.
It can be expected that the antinociceptive effect of 100 and 200 mg/Kgdoses of pregabalin are likely to decrease locomotor activity of mice. As well, it has been reported that pregabalin, at the doses over 100 mg/Kg (SC) or 200 mg/Kg (p.o.), significantly decreases the time spent on rota-rod in other rodents such as rats (
21,
27). However, this wasnot of interest inour study and we considered that the reduction of locomotor activity did not affect antinociceptive assessment in this model of acute pain. Since tail flick response is not largely influenced by light anesthesia and also the dose in which the locomotion should be drastically reduced (400 mg/Kg), none of the antinociception indexes increased.
The commencement of antinociception of pregabalin in this study occurred almost one hour after the injection (IP). The time to reach maximum antinociceptive effect is very different in other experimental models of pain. In inflammatory pain stimulated by formalin and in allodynia induced by trinitrobenzene sulfonic acid in rats, the peak effect of pregabalin happened within thirty minutes (
21,
24). While, in colorectal distention model of visceral pain and in allodynia induced by the chronic constriction injury in mice, the peak result was achieved in one hour (
25,
28). Interestingly, antihyperalgesic activity of pregabalin induced by carrageenan in rats took two hours to happen (
7) and the effect of oral doses lasted for four hours (
27). Finally, in hot-plate model of acute pain which is the nearest model to tail flick test, maximum peak effect was achieved atthe 60
th min which is comparable to the results of this study (
22). All these inconsistencies among peak effects obviously depended on the assumed method, species, route of administration and procedure rather than curve of plasma concentration for pregabalin which holds maximum concentration level at either 0.5 or 2 h in rats (
27).
Other researchers implementing different models of experimental pain, recommended similar dose range of pregabalin. Pregabalin reduced nociceptive scores in the second phase of inflammatory pain and like our study, this effect occurred atdoses of 10, 30 to 100 mg/Kg (
7,
21,
25). The effective dose range used in our study is in complete agreement with previous studies that have investigated the inhibitory effect of pregabalin on colorectal distention response and also on declining colonic nociceptive threshold of visceral pain in sensitized rat (
24,
27-
28).
The general beliefpointed out for the effectiveness of gabapentinoids on pathological pain associated with central sensitizationsuch as neuropathic, postoperative or inflammatory pain while having no antinociceptive effect in acute physiological pain (
3,
25,
29-
30). Nonetheless, gabapentin, the prototype of gabapentinoids, showed antinociceptionin acute pain model of tail flick test and in acetic acid induced visceral pain in intact nervous system (
16,
31). It was clearly shown in this study that the antinociception produced by 100 mg/Kg of pregabalin (%MPE
60=35%) is almost similar to that of 50 mg/Kg of tramadol (%MPE
60= 30%). Thus, our result and that of the recent study on hot plate (
16,
22,
31) set forth that pregabalin is likely to have antinociceptive effect on transient model of pain in non-sensitized nervous system, even though dose-dependency of this effect has not been observed on a regular basis.
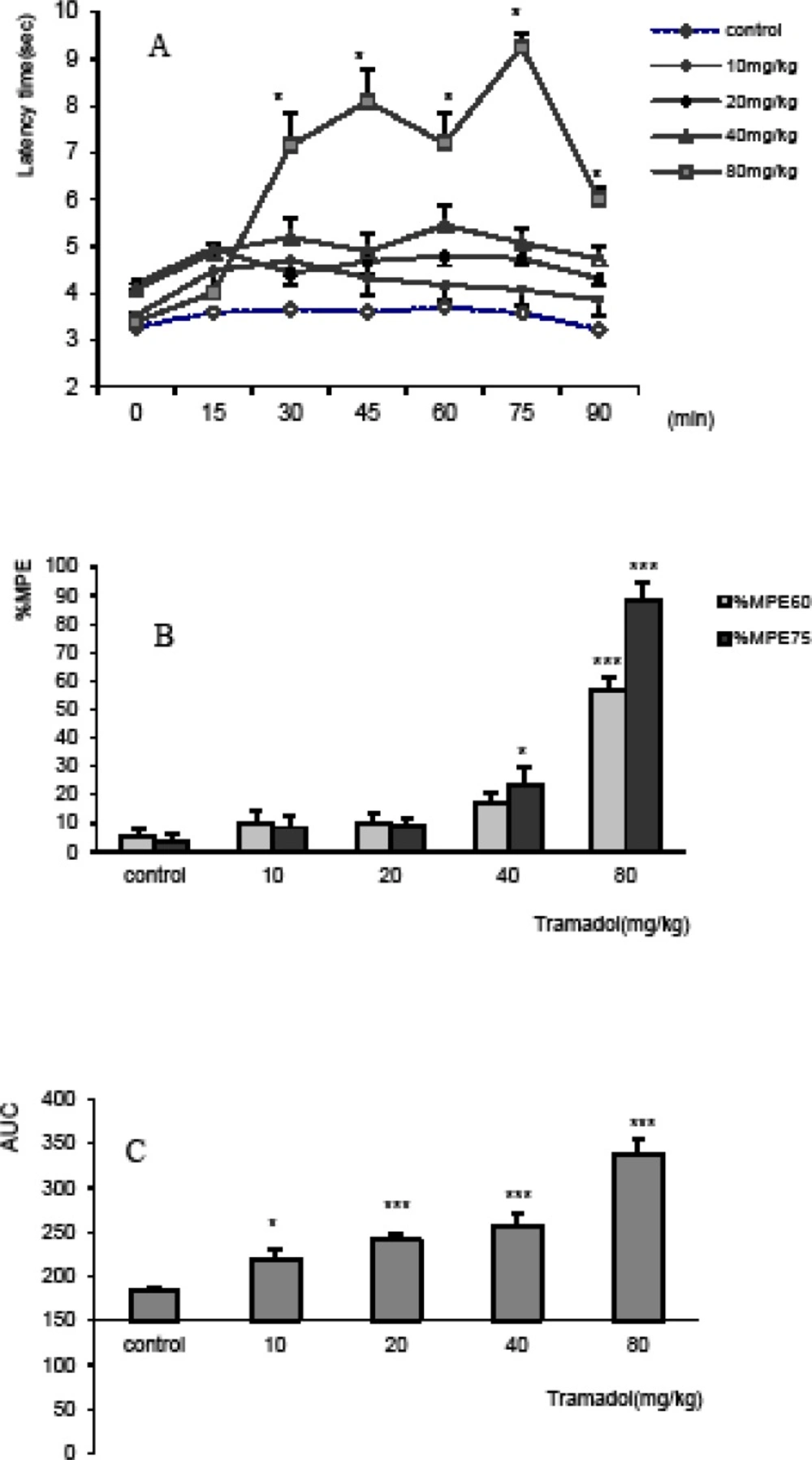
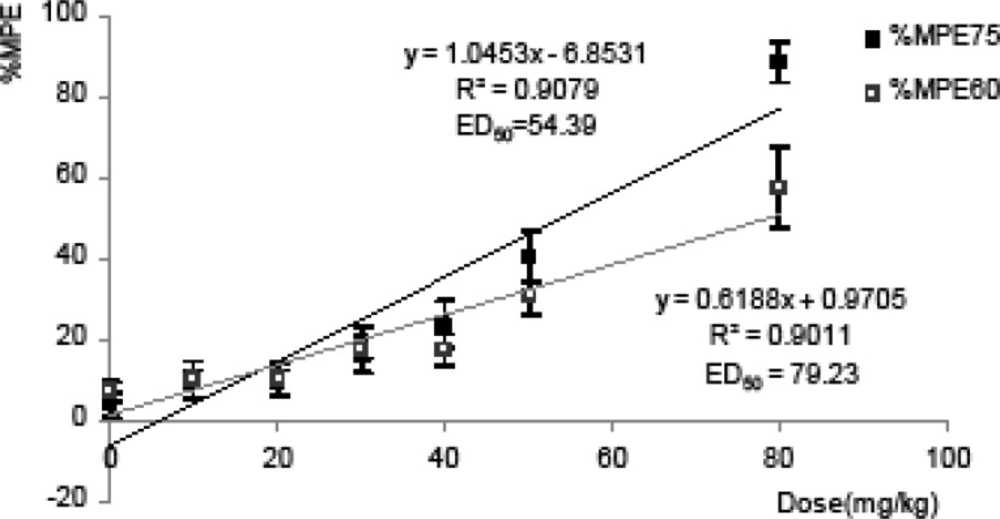
Unlike pregabalin, tramadol produced an evident dose-dependent effect in tail flick test at dose ranges of 10 to 80 mg/Kg as shown in time response curve, %MPE
75,60 and AUC. The induced dose-dependent antiociceptive effect of tramadol was discussed in previous studies using different models of acute pain such as hot-plate, visceral pain induced by acetic acid and the inflammatory pain induced by formalin (
11,
18-
19).The results of our study particularly confirm to the results of another study, in which tramadol increased latency time in tail flick in a dose-dependent manner and also the calculated ED
50which was 59.2 mg/Kg (
32). In accordance, based on previous studies, tramadol produces dose-dependent antinociception at doses of 5 to 40 mg/Kg in rats (
33) and similarly the sub-analgesic dose of 10 mg/Kg has no effect on pain threshold (
34).
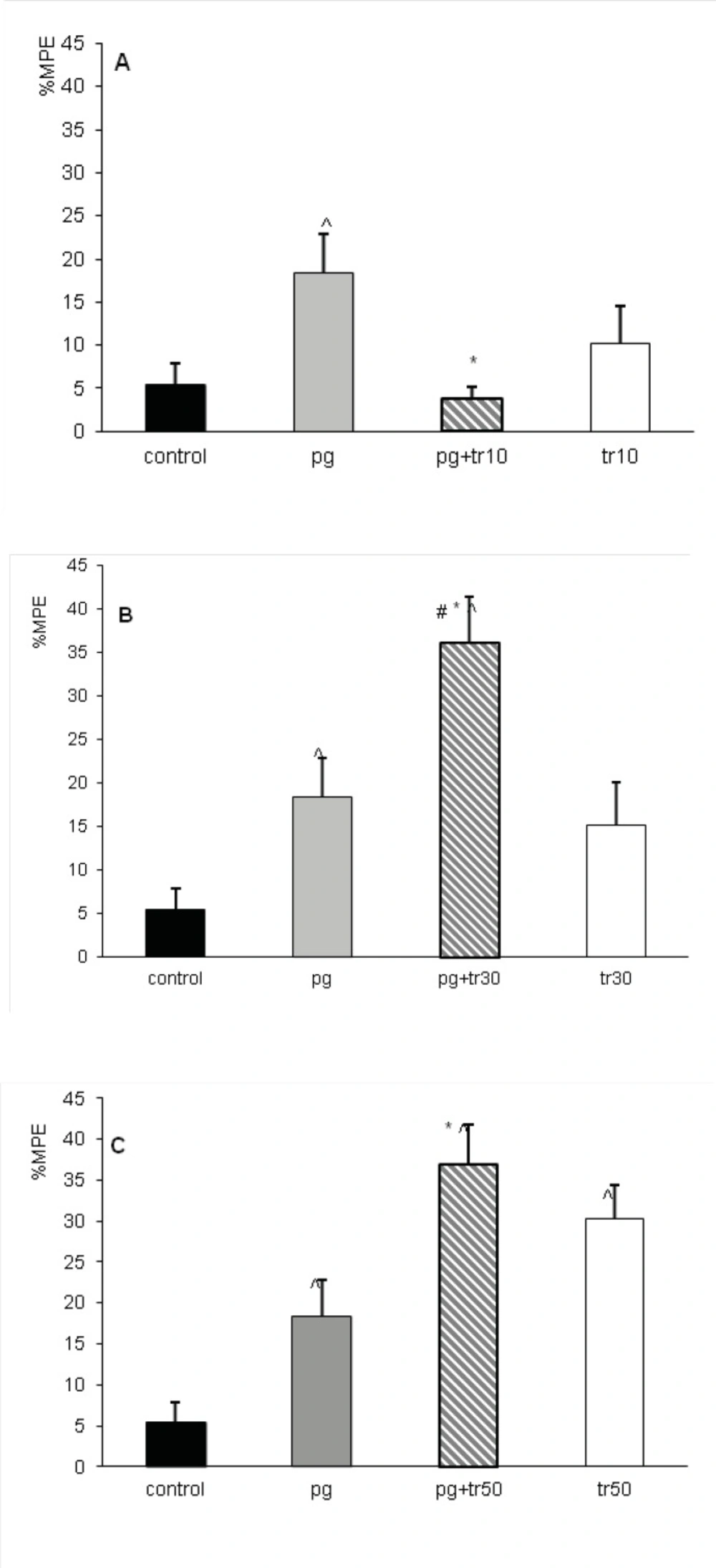
The antinociceptive effect of combination treatment of pregabalin with tramadol varied using different doses of tramadol. The %MPE
60 of combinational group of pg+tr10 decreased when non-analgesic dose of tramadol was added to the sub-analgesic dose of pregabalin;however, in combination group of pg+tr30, the interaction seemed to be supra-additive and in case of combination group ofpg+ tr50, it was nearly additive (
Figure 4) .
No simple explanation exists for the interaction between pregabalin and tramadol or for the variation of interaction especially when different mechanisms account for each drug. The proportion of combined drugs might change the interaction from antagonism to synergism especially when a drug has multimodal mechanism. Indeed, in the combination of tramadol and dexketoprofen, only with potency ratio of 1:1 the synergisms was verified and with any other proportion for the combination this result was not evident (
19).
The increased antinociceptive effect occurred in the combination groups of (pg+tr30) and (pg+tr50) can be explained by the complementary action of pregabalin and tramodol. It has been well established that the main mechanism of anticonvulsant and analgesic action of pregabalin is through binding to alpha-2-delta subunits of voltage dependent Ca
+2 channels decreasing the release of norepinephrine, serotonin and dopamine and particularly glutamate (
10,
25-
26,
29). Since the antagonists of NMDA glutamate receptor enhances mu opioid antinociception (
35), one can deduce that pregabalin by decreasing glutamate release (
29) can increase the thermal antinociception of tramadol. There are other neuromodulators involved in pain transmission that are influenced by tramadol and pregabalin. Indeed, pregabalinreducessubstance P after inflammation in spinal cord slices (
30), and reducesthe formalin- induced release of glutamate in spinal cord of dorsal horn (
26). Whereas, tramadol decreasesthe effect of glutamate and substance P by inhibiting both ionotropic and metabotropic glutaminergic receptors (
36). This additive effect (
Figure 4B, C) was similarly reported in tail flick test in mice when gabapentin (prototype) at dose of 15 mg/Kg(%MPE =10% which is equal to %MPE produced by 10 mg/Kg of pregablin) enhanced the antinociception of tramadol (
32).The synergistic interaction between tramadol and gabapentin has been proved previously using isobolographic study in inflammatory pain model in rats (
11).
However the analgesic effect of these two drugs in combination therapy depends also on the level of the effect produced by each drug. Indeed the interaction of pregabalin with tramadol changed to antagonism when non analgesic dose of tramadol (10 mg/ Kg) that produced 15% of effect was co-administrated in (prg+tr10) group
(Figure 4A). Same results were observed in the combination of metamizol and tramadol. At low level of antinociception (below 25%) produced by each drug, the interaction was antagonistic while at 50% effect or higher all combinations resulted supra-additive (
37). Another hypothesis in this regard might be the concurrent effect of tramadol and pregabalin on decreasing substance P and glutamate effect on pain transmission mentioned above (
26,
30), occurringin a dose-dependent manner (
36). Since this positive effect of tramadol happens above 50 mg/Kg, probably the dose of 10 mg/Kg of tramadol used in this study was insufficient for theinhibition of glutaminergic receptors. Therefore, non analgesic dose of tramadol was not able to increase the antinociceptive effect in prg+tr10 group. Other pathways and receptors might explain this non-enhanced antinociceptive effect in prg+tr10 group. For example; alpha (
2) antagonists increased the antinociception of tramadol in tail flick test of mice while the antinociception of pregabalin was decreased by same agents removing the inhibitory influence of locus coeruleus after nerve injury (
38-
39).
In conclusion, our results demonstrated that pregabalin is likely to have comparable antinociceptive effect to tramadol even though no dose dependent relationship was observed similar totramadol. Withregard to interaction between tramadol and pregabalinand contrary to general beliefthat lower dose of each drug produces lesser side effect and is preferable in combination therapy,the addition of analgesic doses of tramadol increases the antinociceptive effect while non analgesic doses reduced the antinociceptive effect in combined groups. Thusin these multimodal analgesics the effect of combination changes with ratio and level of the effect produced, the fact that is relevant when attempting to use their combination in pain treatment. Thus, more caution should be paid in use of tramadol and pregabalin at very low doses in clinical practice. Isobolographic study will add valuable information in interpreting the statement of this combination, and also more investigations are recommended to establish the modality and correct proportion of co-administration for clinical applications.