

1. Background
Attention-deficit/hyperactivity disorder (ADHD) is a neurodevelopmental condition characterized by chronic symptoms, affecting approximately 8% of children and adolescents globally, with prevalence rates in Iran ranging from 9.5% to 17% (1, 2). The disorder is marked by symptoms such as inattention, hyperactivity, and impulsivity (3), which indicate issues with distractibility or cognitive flexibility (CF). These symptoms are associated with deficits in executive function, including working memory, inhibitory control, and CF. Cognitive flexibility typically develops between ages 4 and 5, reaching adult levels by ages 8 to 10. This ability is crucial for effective learning and problem-solving and is linked to social competence and career success. Deficits in CF lead to increased behavioral issues and challenges in emotional regulation. While some studies indicate that children with ADHD may display average CF, other studies demonstrate specific deficits depending on the tasks involved (4-6).
Children with ADHD often exhibit heightened emotional sensitivity, resulting in intense reactions to minor incidents, complicating ER. Approximately half of these children have difficulty managing their emotions, negatively affecting their academic performance and peer relationships (7). Studies reveal that between 24% and 50% of individuals with ADHD struggle with regulating negative emotions, and there is also evidence of dysregulation in positive emotions (8). The relationship between emotion dysregulation and deficits in attention control and CF in ADHD is complex and not fully understood. Cognitive and emotional processes interact in ADHD, suggesting that emotion dysregulation may stem from difficulties in attention switching and control (9, 10). Children with ADHD often find it challenging to shift their attention effectively, especially when emotional stimuli demand their focus, leading to attention issues in non-emotional tasks (11).
Interventions designed to enhance cognitive performance, including computerized training and physical activities, show inconsistent effectiveness. Although some programs result in short-term gains in specific executive functions (12), these improvements often do not extend beyond the training context. Notably, the Unstuck and On Target program has increased cognitive and problem-solving skills in children. However, other studies suggest that cognitive training frequently lacks lasting effects across diverse executive functions (13, 14). Game-based training might boost motivation and support the transfer of skills to other academic domains, presenting a promising direction for more effective interventions. From childhood through adulthood, the links between CF, executive functions, and ER are well-established (7). Despite the high rates of emotional regulation difficulties among children with ADHD, conventional treatments like stimulant medications and behavioral parent training may not adequately address these challenges (15). While much research has focused on working memory and inhibitory control, CF has received less attention despite its crucial role in emotional regulation.
Emerging research suggests that cognitive rehabilitation, including movement-based and digital interventions, can improve both ER and executive function (12). However, findings regarding the effectiveness of such programs have been mixed (5, 16). One study demonstrated that the ARAM program, developed by an Iranian researcher (17), positively affects one index of executive functions, specifically metacognition (12). However, no significant impact was observed on another index, which is behavioral regulation. Unlike other interventions, ARAM employs computer-based, game-like tasks designed to boost cognitive functions without requiring reading or writing skills, making it accessible to young children. Our current study aims to evaluate ARAM’s effectiveness specifically on CF and ER, building upon prior research focused on selective executive functions or specific populations (12, 18).
While there is significant evidence linking executive functions and ER in ADHD, the underlying mechanisms connecting targeted cognitive training with improvements across these domains remain unclear. Guided by models of executive function development and neuroplasticity (19, 20), interventions that focus on CF may induce neural adaptations that enhance emotional regulation. The premise is that strengthening CF can improve attention shifting and response modulation, ultimately reducing emotional dysregulation. Our study adopts this theoretical framework, hypothesizing that game-based training can foster both cognitive and emotional gains by reinforcing interconnected neural pathways involved in these processes.
2. Objectives
The present study investigates the potential of engaging, game-based computer tasks to enhance CF and ER in children with ADHD. Improving CF is essential for augmenting their capacity to shift attention and control responses — skills that are critical for effective emotion management. By targeting these interconnected abilities, we propose that training in CF can lead to improved emotional regulation, offering a promising strategy to address some of the most significant challenges encountered by children with ADHD.
3. Methods
The present study employed a quasi-experimental design with pre-test and post-test assessments, a control group, and a 5-week follow-up to evaluate the effectiveness of the ARAM computer game-based program on children with ADHD. Conducted in 2022, the research involved children aged 7 to 11 years, selected through convenience sampling from two psychological clinics. A final sample of 30 children diagnosed with combined-type ADHD was derived from a cohort of 60 referred children, based on the Conners Rating Scale (parent form). The study’s sample size of 30 participants is relatively small, which may affect its statistical power and the generalizability of the results. However, the presence of a control group, along with pre- and post-testing, provides a robust framework for evaluating the effectiveness of the interventions. Additionally, the five-week duration of the study enhances its credibility.
Participants were eligible if they had parental consent, showed willingness to participate, had an IQ of 85 or above, and did not use any stimulant medications other than Ritalin (methylphenidate). Children with additional neurodevelopmental disorders were excluded. Thirty eligible participants were matched for age, education, and IQ, then evenly divided into experimental and control groups. The experimental group participated in 10 sessions of the ARAM program (45 - 60 minutes each), while the control group played “Brain Boost” games. These games are engaging brain-training activities designed to enhance skills like attention, memory, and problem-solving. They are colorful, with sounds and rewards to maintain participant motivation. The games adapt to each person’s skill level, becoming more challenging, which helps keep the activity interesting and effective. In this study, the control group’s use of “Brain Boost” games served as an active control activity intended to match the experimental group’s engagement duration and cognitive effort, without specifically targeting the core constructs addressed by the ARAM program. This approach helps isolate the effects of the specific intervention from general cognitive activity or placebo effects.
Evaluations were conducted after the intervention and again during a 5-week follow-up using the Wisconsin Card Sorting Test (WCST) and the Emotion Regulation Checklist (ERC), with assessments performed in a blinded manner by the research assistant to reduce bias. The Conners Rating Scale, developed by Conners in 1997, comprises 27 items rated on a 4-point Likert scale and assesses five domains related to ADHD. The scale exhibits strong construct validity and reliability, with a t-score of 70 indicating a diagnosis of ADHD. The reliability of the scale is reported to be 0.90, featuring a test-retest correlation of 0.58 and a Cronbach’s alpha of 0.73 for the overall score. A t-score of 70 or above on this scale signifies a diagnosis of ADHD (21).
Raven’s progressive matrices (RPM) is a nonverbal intelligence tool designed to evaluate cognitive abilities independent of language, culture, and educational background. First published in 1938, the RPM consists of two forms: One for individuals aged 9 years and older and another for children aged 5 to 9 years and adults with suspected low intelligence. The adult version includes 60 black-and-white geometric figures where participants identify logical patterns to complete matrices, while the child version consists of 36 colored geometric figures divided into three sections, each requiring the selection of an appropriate pattern to complete an incomplete shape. Raw scores from both forms are reported as IQ scores, with a mean of 100 and a standard deviation of 15. Correlations with other intelligence scales, such as the Stanford-Binet Intelligence Scales and the Wechsler Intelligence Scale for Children, are 0.40 and 0.76, respectively (22).
The WCST (Grant and Berg, 1948) evaluates cognitive functions such as CF, problem-solving, and concept formation. In this task, participants sort cards with various geometric shapes and colors while adapting to changing rules. The WCST shows a satisfactory reliability coefficient of 0.90 (23). In this study, both assessments were conducted individually to measure CF and executive functions in children. However, it is important to recognize its limitation when considering ecological validity — the extent to which WCST performance reflects real-world behaviors.
The ERC (Shields and Cicchetti, 1997) is designed to assess ER in children aged 7 to 11 years. It consists of 24 items divided into two components: Adaptive emotion regulation (AER) and lability/negativity (L/N). The Adaptive component includes eight items focusing on emotional expression, empathy, and self-awareness, while the L/N component comprises 16 items that assess temperament instability and inappropriate emotional expression. Responses are rated on a four-point Likert scale, with overall scores indicating levels of ER: Scores above 60 suggest very strong regulation, 40 - 60 indicate moderate regulation, and below 40 reflect very weak regulation. The assessment demonstrates high reliability, with a Cronbach’s alpha of 0.96 for L/N and 0.83 for AER (24).
All assessments, including the WCST and ERC, were conducted by a research assistant who was blinded to the participants’ group allocations. The assessor was kept unaware of treatment conditions by scheduling evaluations without revealing group assignments, and participants were instructed not to disclose their group to the assessor. Standardized scoring was applied to ensure objectivity, thereby aiming to minimize potential bias and enhance the reliability of our evaluation results. These measures aimed to enhance the validity of our findings by reducing the risk that evaluators’ expectations could influence the assessment outcomes.
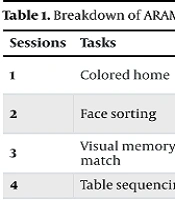
The ARAM program (Table 1) comprises ten sessional progressive tasks specifically designed to strengthen core cognitive domains (25) based on Baddeley’s working memory model (26). Tasks like colored home target sustained and selective attention by requiring children to identify targets amid distractors; face sorting promotes attention shifting and divided attention through flexible categorization; and activities such as visual memory match and letter sequencing aim to enhance visuospatial and phonological working memory, respectively. Tasks involving acronym formation and color recall specifically target inhibitory control and updating, fundamental components of executive functioning (17). The tasks increase in difficulty across sessions to ensure continuous challenge and motivation, with performance-based adjustments to individualize difficulty levels. This tailored approach differentiates ARAM from more general brain-training games. Unlike many traditional digital interventions that focus on repeating single skills, ARAM takes a more holistic approach by combining activities targeting attention, working memory, CF, and emotional regulation — all within engaging, fun games. Plus, the gamified format boosts engagement and keeps children coming back, promoting better long-term results (27). In short, ARAM offers a more comprehensive, engaging, and flexible approach — merging cognitive, emotional, and motivational strategies — to better support children with ADHD than many existing digital tools (25). Children need to answer at least 80% correctly to advance to more difficult levels, ensuring tailored difficulty. To control for confounding variables such as engagement, session duration, and task difficulty, all computer tasks and games are matched in interaction time (35 - 45 minutes) and systematically adjusted based on performance. The intervention emphasizes stimulating stimuli to maintain motivation equally across groups. Researcher supervision was limited to observing adherence, minimizing influence on performance, and this setup aims to isolate the effects of the ARAM program and strengthen causal inferences.
| Sessions | Tasks | Goals | Activity Details |
|---|---|---|---|
| 1 | Colored home | Improve sustained and selective attention | Identify a target among similar images; increasing difficulty with color variations and distractors |
| 2 | Face sorting | Enhance attention shifting, divided attention | Arrange falling faces based on features like skin or hair color; difficulty rises with speed and complexity |
| 3 | Visual memory match | Strengthen visuospatial working memory | Match hidden image pairs within a grid; complexity escalates with more items and similar shapes |
| 4 | Table sequencing | Develop spatial memory span | Select matching tables following cues; increasing cue complexity and delay |
| 5 | Fragment assembly | Boost visuospatial memory updating | Reassemble images from fragments after a delay; difficulty varies with fragments and complexity |
| 6 | Acronym formation | Improve phonological processing and inhibitory control | Create words from initials; challenges increase with length and similarity |
| 7 | Color recall | Enhance updating skills | Choose the last color in a sequence; difficulty increases with sequence length |
| 8 | Animal search | Strengthen spatial working memory | Find animals in different locations guided by directional cues |
| 9 | Image repetition | Improve updating ability | Spot repeated images; task difficulty adjusts with complexity and similarity |
| 10 | Letter sequencing | Enhance phonological span and control | Match first and last letters in sequences; difficulty varies with length and speed |
3.1. Statistical Analysis
Data were analyzed using both descriptive and inferential statistics. Descriptive statistics included means and standard deviations. Inferential analyses involved the chi-square test, Mann-Whitney U test, Mauchly’s test of sphericity, and repeated-measures ANOVA. All analyses were conducted using SPSS, version 25. To gain a better understanding of individual response patterns, responder analyses were performed to identify subgroups of participants and explore response variability across the sample. These analyses provided deeper insights into the data and facilitated the interpretation of differential effects observed among participants.
4. Results
The experimental group had an average age of 9.20 years (SD = 1.14), compared to 8.47 years (SD = 1.50) in the control group. Mann-Whitney U tests showed no significant differences between groups in IQ (U = 105, P = 0.754), age (chi-square = 33.3, P = 0.504), or education levels (chi-square = 4.60, P = 0.467), indicating that the groups were well matched at baseline (Table 2).
| Factors and Groups | Mean ± SD | t-Score | Percentile Rank |
|---|---|---|---|
| Conduct problems | |||
| Experimental | 20 ± 1 | 62 | 87 |
| Control | 21 ± 1 | 63 | 89 |
| Learning problems | |||
| Experimental | 8 ± 1 | 60 | 86 |
| Control | 9 ± 1 | 63 | 89 |
| Psychosomatic symptoms | |||
| Experimental | 10 ± 2 | 66 | 93 |
| Control | 8 ± 1 | 61 | 86 |
| Impulsivity-hyperactivity | |||
| Experimental | 11 ± 3 | 68 | 94 |
| Control | 10 ± 1 | 65 | 92 |
| Anxiety | |||
| Experimental | 9 ± 1 | 61 | 86 |
| Control | 9 ± 2 | 61 | 86 |
| Overall score | |||
| Experimental | 58 ± 13 | 69 | 94 |
| Control | 57 ± 11 | 69 | 94 |
Abbreviations: M, mean; SD, standard deviation.
As shown in Table 2, both groups demonstrated comparable scores across all domains of the Conners Rating Scale, indicating similar levels of symptom severity in behavioral, learning, emotional, impulsivity, and anxiety-related domains at baseline. The differences in means, standard deviations, and percentiles were minimal, supporting the equivalence of the groups prior to intervention.
Results in Table 3 reveal that the experimental group showed significant improvements in CF, ER, AER, and L/N from pre-test to post-test and during the follow-up period. Conversely, the control group did not demonstrate notable changes. The repeated-measures ANOVA confirmed that the data were normally distributed (P > 0.05), although Mauchly’s test of sphericity was violated, necessitating the application of the Greenhouse-Geisser correction. After adjustments, analyses confirmed the ability to compare CF, ER, AER, and L/N across groups and time points confidently (Table 4).
| Variables and Groups | Pre-test | Post-test | Follow-up |
|---|---|---|---|
| CF | |||
| Experimental | 113.15 ± 13.22 | 85.83 ± 12.75 | 86.08 ± 13.19 |
| Control | 96.47 ± 18.27 | 94.38 ± 17.39 | 95.47 ± 18.83 |
| ER | |||
| Experimental | 168.41 ± 3.16 | 137.25 ± 24.23 | 138 ± 23.46 |
| Control | 148.46 ± 29.52 | 149.46 ± 29.52 | 149.53 ± 29.14 |
| AER | |||
| Experimental | 114.24 ± 14.25 | 124.76 ± 13.89 | 145.22 ± 25.55 |
| Control | 131.49 ± 19.25 | 146.22 ± 28.47 | 155.29 ± 30.14 |
| L/N | |||
| Experimental | 97.52 ± 19.47 | 131.06 ± 11.52 | 134.58 ± 22.78 |
| Control | 147.11 ± 38.25 | 145.72 ± 29.37 | 143.55 ± 28.41 |
Abbreviations: CF, cognitive flexibility; ER, emotion regulation; AER, adaptive emotion regulation; L/N, lability/negativity.
a Values are expressed as mean ± SD.
| Variables and Source of Change | SS | df | MS | F Statistics | P-Value | ɳ2 |
|---|---|---|---|---|---|---|
| CF | ||||||
| Time | 1123.004 | 1.19 | 972.236 | 19.625 | < 0.001 | 0.47 |
| Group | 1161.548 | 1.19 | 981.174 | 20.517 | < 0.001 | 0.56 |
| ER | ||||||
| Time | 1853.42 | 1.15 | 1609.32 | 13.27 | < 0.001 | 0.467 |
| Group | 1864.003 | 1.15 | 1628.74 | 13.23 | < 0.001 | 0.468 |
| AER | ||||||
| Time | 1871.01 | 1.23 | 1457.24 | 13.26 | < 0.001 | 0.474 |
| Group | 1869.28 | 1.23 | 1486.04 | 13.12 | < 0.001 | 0.458 |
| L/N | ||||||
| Time | 1878.03 | 1.70 | 1825.02 | 13.01 | < 0.001 | 0.463 |
| Group | 1869.37 | 1.70 | 1841.11 | 13.24 | < 0.001 | 0.471 |
Abbreviations: CF, cognitive flexibility; ER, emotion regulation; AER, adaptive emotion regulation; L/N, lability/negativity; SS, sum of square; df, degree of freedom; MS, mean of square; ɳ2, Eta quotient.
Table 4 shows significant differences between the experimental and control groups in all targeted areas across the three assessment points. Effect size estimates (eta-squared) ranged from 0.47 to 0.56, indicating that the intervention explained a substantial proportion of variance in these variables, supporting our hypotheses. Further statistical details, including independent t-tests at each time point, are summarized in Table 5.
| Variables and Time | t | df | P-Value | Mean Difference | Confidence Interval 0.95 |
|---|---|---|---|---|---|
| CF | |||||
| Pre-test | 1.74 | 28 | 0.23 | 5.74 | -7.23 to 14.32 |
| Post-test | 3.25 | 23 | 0.315 | -8.45 | -21.74 to 5.12 |
| Follow-up | 4.14 | 23 | 0.425 | -6.85 | -21.62 to 6.45 |
| ER | |||||
| Pre-test | 1.52 | 27 | 0.528 | 6.15 | -12.62 to 25.54 |
| Post-test | 4.23 | 23 | 0.286 | -12.42 | -32.47 to 10.12 |
| Follow-up | 4.41 | 23 | 0.341 | 9.62 | -32.81 to 11.41 |
| AER | |||||
| Pre-test | 1.57 | 26 | 0.242 | 5.41 | -13.84 to 25.32 |
| Post-test | 4.02 | 23 | 0.336 | -7.14 | -33.21 to 12.14 |
| Follow-up | 4.07 | 23 | 0.548 | 8.75 | -33.84 to 12.63 |
| L/N | |||||
| Pre-test | 1.23 | 29 | 0.781 | 7.41 | -11.29 to 25.98 |
| Post-test | 4.51 | 23 | 0.325 | -5.36 | -31.02 to 13.24 |
| Follow-up | 4.49 | 23 | 0.473 | 9.94 | -31.84 to 13.41 |
Abbreviations: CF, cognitive flexibility; ER, emotion regulation; AER, adaptive emotion regulation; L/N, lability/negativity.
Finally, Table 5 indicates no significant differences in CF and ER between groups at baseline (P > 0.1), suggesting that initial characteristics were similar. Both groups showed further improvements post-intervention and at follow-up, implying sustained effects of the program.
5. Discussion
Attention-deficit/hyperactivity disorder is a common and persistent childhood condition that adversely affects self-control, academic success, and social relationships. This study evaluated the impact of a computer game-based intervention on CF and ER in children aged 7 to 11 with combined-type ADHD. The findings revealed notable improvements in CF within the experimental group, consistent with previous research (6, 16, 28-30). The highly engaging nature of the games likely enhanced children’s motivation and interest. Structured task progression and a variety of exercises, carefully designed to adhere to game rules, specifically targeted CF by encouraging adaptability and flexible thinking (17). Cognitive flexibility is fundamentally linked to executive functions such as working memory and inhibitory control, which facilitate adaptability (6). During childhood, the brain’s neuroplasticity allows for significant reorganization and improvement of these skills (29). Activities involving computer-based games stimulate neural pathways through neuroplasticity, as evidenced by studies measuring brain-derived neurotrophic factor (BDNF) levels before and after neurorehabilitation (13). Cognitive training tasks, like those employed in the ARAM program, are believed to promote neural repair and reorganization, particularly within neural circuits involved in executive function and CF. Additionally, improvements in executive functions are interconnected, creating an environment that enhances attention and response times (4).
Although our present findings are promising, we acknowledge that additional research is necessary to directly investigate these neurobiological processes. Further studies employing neuroimaging or neurophysiological techniques, such as MRI or EEG, could elucidate how game-based interventions induce neural changes, including neuroplasticity, reward system engagement, and neural adaptation. Grounded in models of executive function development and neuroplasticity (19, 20), targeted CF training may facilitate neural changes that support both emotional regulation and attentional control. Better understanding these processes could help us see how such interventions lead to lasting benefits for children with ADHD, not just in attention, but also in regulating emotions.
Additionally, the WCST is widely regarded as a reliable measure of CF and executive functioning (23). While the WCST captures essential components of flexibility, such as adapting to changing rules and problem-solving in a controlled setting, these skills may not directly translate to the dynamic, context-rich environments children encounter daily. For instance, real-life situations often involve social nuances, emotional factors, and multitasking that are not fully encapsulated by this test. Understanding this gap is crucial when interpreting our findings, as improvement on the WCST does not necessarily guarantee improved flexibility in everyday life. Future studies should consider supplementing neuropsychological assessments with ecological momentary assessments or real-world behavioral observations to better gauge the practical implications of CF interventions.
The study also demonstrated that the computer game-based program significantly improved ER, consistent with earlier research (7, 9, 31). The structured and engaging design — progressing from simple to more complex tasks — appears to foster motivation. Children with ADHD often struggle with engagement due to factors like suboptimal arousal (leading to under-stimulation or over-reactivity), altered reward sensitivity favoring immediate rewards, and higher thresholds for motivation. These challenges hinder sustained attention and task completion. The engaging nature of game-based activities can effectively counteract these motivational barriers, enabling children to function more like their typically developing peers when suitably stimulated (7). To address motivation and engagement challenges, enhancing reward structures and providing instant positive feedback can significantly improve arousal regulation and focus (31). Our results show that these tasks boost AER by fostering motivation and adaptability, aligning cognitive efforts with real-world situations (30). The incremental design — progressing toward greater speed, accuracy, and attention — coupled with immediate feedback, encourages children to monitor and modulate their emotional responses, thereby improving ER. The bidirectional relationship between CF and ER suggests that practicing flexibility can directly enhance emotional control (11). Consistent with previous research, improvements in the L/N Index further support these findings (9, 17, 31). Enhancing executive functions like CF appears to positively influence emotional stability, potentially leading to better emotional control and more adaptive behavior.
While our results suggest that the tasks may influence both CF and ER, we acknowledge a key limitation: We did not directly examine how improvements in one relate to the other. Our findings show that strategies like immediate feedback and incremental difficulty helped children better monitor and regulate their emotions, aligning with theories about the close link between these processes (11, 30, 31). However, without specific statistical analyses connecting changes in these areas, we cannot confirm how strongly they are related within our sample. Future research should explore this connection directly, as understanding it could inform more targeted interventions for children with ADHD.
Importantly, we found that gains in CF and ER persisted over a five-week follow-up, indicating lasting effects of the ARAM intervention. While this is promising, we should differentiate between statistical significance and real-world impact. Just because changes are statistically reliable does not mean they translate into meaningful improvements in daily life, such as social interactions or overall well-being. Future studies should assess the practical significance of these gains to capture their true benefit.
Our results also highlight the roles of motivation and arousal in maintaining engagement and emotional control, providing insights into how game-based interventions like ARAM function. Such approaches might generate enduring benefits beyond initial training effects, though several alternative explanations must be considered. Factors such as placebo effects, individual motivation, and natural development could influence outcomes. Controlling for these variables in future research will help clarify the specific impact of our intervention.
A limitation we did not fully address involves the neural mechanisms underlying these changes. Future work should investigate processes like neuroplasticity, executive functioning, and reward processing to better understand how game-based interventions facilitate improvements. The COVID-19 pandemic posed additional challenges by disrupting intervention delivery and participant engagement, which should be carefully considered in future studies. Our sample was non-random and relied heavily on parent reports, which may introduce bias, and many children were on medication — factors that complicate interpreting the results. Although we included children on stable medications, we did not analyze how medication interacts with the intervention’s effects; existing evidence suggests medication can influence cognitive domains targeted by ARAM, and combined treatments might have additive benefits (32, 33).
We focused solely on boys because ADHD is diagnosed more frequently in males — about two to three times more often — which helped us maintain a more uniform sample and facilitate clearer interpretation. We plan to include girls in future studies to explore potential gender differences. While we believe in the safety and engagement value of this virtual approach, some children might experience frustration or overstimulation initially, especially without supervision. Extended use could also reduce physical activity or face-to-face interactions, so caregiver monitoring is essential. Future research should examine these interactions more systematically to optimize the integration of medication and behavioral interventions.
Finally, we recognize that individual differences — such as ADHD subtypes, medication status, baseline characteristics, and environmental factors — may influence how children respond to ARAM (34). These moderating factors can confound outcomes and should be studied systematically. Enhancing ARAM with adaptive difficulty, real-time feedback, and personalized content, along with training caregivers to support skill transfer, could improve its efficacy. Comparing subtypes and considering medication use will help tailor the intervention further, ultimately moving toward more personalized, effective, game-based treatments for children with ADHD.
5.1. Conclusions
Building on our findings, future implementation of game-based interventions like ARAM should focus on identifying which components most effectively target neural and cognitive processes — particularly CF and ER. Customizing these programs to accommodate individual differences, such as ADHD subtypes and baseline traits, will likely increase their effectiveness in educational and clinical settings. Furthermore, understanding how medication interacts with intervention responses can inform the development of combined approaches that optimize both behavioral and learning outcomes. Creating evidence-based guidelines for integrating ARAM into classrooms will empower teachers and clinicians to deliver personalized, impactful support tailored to each child’s needs. These programs should be designed to foster high motivation and arousal, which are critical for engaging children and enhancing their emotional regulation, attention, and cognitive skills. Ultimately, thoughtfully developed educational interventions that address both cognitive and emotional deficits will promote comprehensive development and lead to better educational and life outcomes for children with ADHD.
