


1. Introduction
2. Case Presentation
2.1. Case 1
| Parameters | Case 1 | Case 2 | Case 3 |
|---|---|---|---|
| Hemoglobin (g/dL) | 10.7 | 11.9 | 11.7 |
| WBC (/µL) | 13,000 | 9,500 | 11,400 |
| WBC diff count | Monocyte 10% | Lymphocyte 47% | Within normal range |
| Platelets (/µL) | 591,000 | 673,000 | 389,000 |
| ASTO (IU/mL) | 800 | 800 | 400 |
| Electrolyte: K, Na, Cl, Ca (mmol/L) | Normal | Normal | K 5.8 |
| Blood urea (mg/dL) | Normal | Normal | 82 |
| Creatinine (mg/dL) | Normal | Normal | 1.5 |
| C-reactive protein | (+) | (+) | -- |
| Others | -- | -- | Albumin: 2.7 g/dL; urinalysis; haematuria 3+, proteinuria 1+ |
Abbreviation: WBC, white blood cells.
a Normal value: Hemoglobin = 12.0 - 15.0; WBC = 4,500 - 13,400; platelets = 150,000 - 450,000; monocyte = 2 - 8%; lymphocyte = 20 - 40%; ASTO ≤ 200; blood urea = 14.9 - 35.9; creatinine = 0.73 - 1.18; albumin = 3.5 - 5.2.
 and left ventricular (LV) dilatation, global normokinetic, and severe mitral regurgitation (MR). Excessive motion in flail anterior mitral leaflet (AML) with suspicion of distal tip restriction or thickening and impinged towards LV outflow tract during diastole (green arrow).")
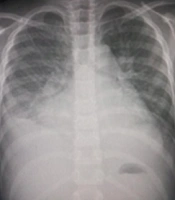
A, case 1 chest x-ray showed cardiomegaly and pulmonary congestion; B, echocardiography PLAX showed left atrial (LA) and left ventricular (LV) dilatation, global normokinetic, and severe mitral regurgitation (MR). Excessive motion in flail anterior mitral leaflet (AML) with suspicion of distal tip restriction or thickening and impinged towards LV outflow tract during diastole (green arrow).
2.2. Case 2
, and left ventricular (LV) dilatation, global normokinetic, and mitral regurgitation (MR) severe with suspected vegetation on the anterior mitral leaflet (AML) (blue arrow).")
A, case 2 chest x-ray showed cardiomegaly and pulmonary congestion; B, echocardiography PLAX one month ago showed RA, left atrial (LA), and left ventricular (LV) dilatation, global normokinetic, and mitral regurgitation (MR) severe with suspected vegetation on the anterior mitral leaflet (AML) (blue arrow).
2.3. Case 3
 and severe tricuspid regurgitation (TR), without any excessive motion and no thickening or impingement (red arrow).")
A, case 3 chest X-ray showed cardiomegaly, pulmonary congestion, and pleural effusion; B, echocardiography PLAX showed four chamber dilatation and global hypokinetic, slight pericardial effusion, severe mitral regurgitation (MR) and severe tricuspid regurgitation (TR), without any excessive motion and no thickening or impingement (red arrow).