



1. Background
Gallstone is a common problem with a prevalence rate ranging from 11% to 36% (1). The incidence rate of this problem is related to age, sex, and ethnicity, with a higher rate among female subjects (1). The association between gallstone and Helicobacter pylori (H. pylori) infection is controversial (1-6). Determining the association between gallstone and H. pylori infection would help to better plan preventive programs (2, 7-10). Cholecystitis is a common surgical procedure usually due to gallstone (11). Female gender, older age, and obesity are important risk factors for cholecystitis (11, 12), but it may be seen without gallstone in nearly 10% of cases (13). Gallstone is related to both environmental and genetic factors (14). Gallstone may even be seen in asymptomatic patients, and further workup with a special focus on the etiological factors is required (15, 16). Helicobacter pylori is an important infectious factor besides the other related diseases such as peptic ulcer, dyspepsia, and cancer (17); it is observed in 70.1%, and 86.2% of patients with gastritis and gastric ulcer, respectively (18), and positive antibody is seen in 86.3 - 91% of Iranian patients (19).
2. Objectives
3. Methods
This observational study was performed as a descriptive-comparative cross-sectional survey. We participated 169 consecutive patients with H. pylori gastritis that had dyspepsia and epigastric pain and were admitted to Imam-Hossein Hospital, Tehran, Iran, in 2018; the required data was recorded in a checklist. The exclusion criteria were the use of antibiotics with anti-H. pylori effects such as metronidazole, ciprofloxacin, levofloxacin, amoxicillin, bismuth, tetracycline, and clarithromycin, besides PPI use.
This study was approved by the local ethics committee with the code of ethics BMSU13971617. Informed consent was not required, but confidentiality of the data was respected. All the ethical considerations were adhered to, and we had no intervention in this study. Biopsy samples were assessed to establish H. pylori infection and gastritis, and they were stained by Hematoxylin and Eosin. In positive cases for H. pylori infection, gallstone frequency rate was determined by ultrasound assessment and compared with other variables.
Data analysis was performed by SPSS version 25.0. The numerical data was reported as mean and standard deviation, and frequency and percentage were reported for categorical variables. chi-square test and Fisher’s exact test were run to analyze the data. A P-value of less than 0.05. was considered significant.
4. Results
Among the subjects, 64.5% were female, 18.9% were under 40 years old, and 23.7% were over 60 years old. The residence location was cities other than Tehran in 23.1% of the patients. Body mass index (BMI) was underweight, normal, overweight, and obese in 3%, 37.3%, 24.3%, and 35.3%, respectively. Gallstone was diagnosed in 8.3% of cases, family history was positive in 28 (16.6%) of cases, and gastritis was mild, moderate, and severe in 21.3%, 65.7%, and 13% of cases respectively. Among the subjects, 85 (50.3%) patients had high amounts of H. pylori. Gallstone history was positive in 5 (3%) patients.
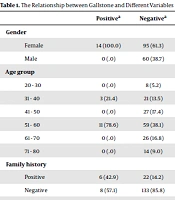
As shown in Table 1, gender and gallstone were interrelated (P = 0.002). Also, age was related to gallstone (P = 0.029). There was no significant association between gallstone and residence location (P = 1.000), BMI (P = 1.000), and gastritis severity (P = 0.176).
| Positivea | Negativea | P-Value | |
|---|---|---|---|
| Gender | 0.002 | ||
| Female | 14 (100.0) | 95 (61.3) | |
| Male | 0 (0) | 60 (38.7) | |
| Age group | 0.029 | ||
| 20 - 30 | 0 (0) | 8 (5.2) | |
| 31 - 40 | 3 (21.4) | 21 (13.5) | |
| 41 - 50 | 0 (0) | 27 (17.4) | |
| 51 - 60 | 11 (78.6) | 59 (38.1) | |
| 61 - 70 | 0 (0) | 26 (16.8) | |
| 71 - 80 | 0 (0) | 14 (9.0) | |
| Family history | 0.014 | ||
| Positive | 6 (42.9) | 22 (14.2) | |
| Negative | 8 (57.1) | 133 (85.8) | |
| Self-gallstone history | 0.0001 | ||
| Positive | 5 (35.7) | - | |
| Negative | 9 (64.3) | 155 (100) | |
| Helicobacter pylori | 0.561 | ||
| High | 6 (42.9) | 79 (51.0) | |
| Low | 8 (57.1) | 76 (49.0) |
a Values are expressed as No. (%).
There was a significant association between gallstone and family history (P = 0.014) and between gallstone and self-history of gallstone. However, there was no significant association between gallstone and H. pylori gastritis (P = 0.561).
5. Discussion
In this study, gallstone frequency in patients with H. pylori gastritis was determined. We also evaluated the factors contributing to gallstone and the treatment of gastritis due to H. pylori that may prevent stone formation and subsequent surgical complications. In this study, 8.3% of the patients with H. pylori gastritis had gallstone in ultrasound assessment. However, the severity of gastritis was not related to gallstone. Older age, female gender, and gallstone history were related to gallstone in the current study.
The study by Attaallah et al. (1) revealed that 37% of patients with symptomatic gallstone had H. pylori infection, but this rate was lower in our study. Zhang et al. (2) reported that the incidence rates of gallstone in patients with positive helicobacter, eradicated helicobacter, and negative helicobacter status were 9.47%, 9.02%, and 8.46%, respectively, showing no significant association. Sabbaghian et al. (3) studied 36 patients under cholecystectomy and noted that 33.3% were positive for H. pylori in PCR; this rate was lower in our study.
The study by Lee et al. (4) among 58 cases under cholecystectomy found that H. pylori was positive in four cases with gallstones, six cases with biliary secretions, and five patients with positive biliary tissue. The reported rates were higher than those obtained in our study. Monstein et al. (5) reported that 55% of patients with cholesterol gallstone had a positive status for H. pylori, this rate was higher in comparison with our finding. Takahashi et al. (6) reported that the prevalence rates of gallstone in cases with negative helicobacter status, eradicated conditions, and positive cases were 3.81%, 4.37%, and 6.08%, respectively, while the rate in our study was higher.
The study by Stathopoulos et al. (7) showed that 20.54% of cases with gallstone had positive results for H. pylori infection in gastric biopsy samples, which was higher than our finding. Deeba et al. (8) studied 75 patients with gallstone symptoms, which showed that IgG was positive against H. pylori; this rate was higher than our results. Abro et al. (9) demonstrated that H. pylori infection was observed in the biliary tissue of 55% of cases with chronic cholecystitis. Fikry et al. (10) reported a contributing rate of 63%, which is higher than our obtained results.
In sum, gallstone frequency in patients with H. pylori gastritis is low, and there is no statistically significant association between these two conditions. However, further studies with larger sample sizes are required to corroborate our results.
