1. Context
Coronaviruses constitute a large family of viruses causing various diseases ranging from the common cold to more severe diseases such as Middle East respiratory syndrome coronavirus (MERS-CoV) and severe acute respiratory syndrome coronavirus (SARS-CoV). The new coronavirus (nCoV) is the latest strain not recognized in individuals in the past (1). Coronaviruses are RNA viruses that spread widely among humans, birds, and mammals that make diseases in the liver and intestinal, respiratory, and nervous systems. Coronaviruses are zoonotic pathogens and are transmitted between animals and humans. Comprehensive examinations discovered that MERS-CoV was transmitted from dromedary camels and SARS-CoV from civet cats to humans. Some identified coronaviruses are transmitted between animals, which have not infected humans yet (2, 3). General signs of the disease involve a fever, shortness of breath, cough, respiratory symptoms, and breathing problems. The infection can make severe acute respiratory syndrome, kidney failure, pneumonia, and even death in more severe cases (1, 4).
On 31 December 2019, some cases with severe acute respiratory infections were reported in Wuhan City, Hubei Province of China. Based on primary observations, it seemed that the patients had a history of work in the fish and seafood market. The market was closed immediately on 1 January 2020, and environmental sanitation and disinfection were carried out there completely. A few days later, after the rejection of the diagnosis of seasonal influenza, avian influenza, adenovirus, SARS coronavirus, and MERS coronavirus, some other pathogens were identified. On 9 January, a virus was diagnosed as a causative agent of the disease in 15 out of 59 hospitalized patients with Sarbecovirus, which raised great concern. The new coronavirus shares about 50% of the genetic identity with SARS and is a subset of Sarbecovirus (5).
The virus has been briefly named nCoV-2019 to find out more information. On 11 January 2020, the first deaths from the virus were reported from China and the reports of positive cases from other countries such as Thailand, Japan, South Korea, and the United States by 20 January and Person-to-person transfer to medical staff made the situation even more complicated. Yet, there is no appropriate vaccine or treatment for 2019-nCoV, and therefore, having a high clinical suspicion and questioning the history of travel and contact with febrile patients and patients with respiratory symptoms have a very important role in the prevention and control of the disease (6). Standard precautions to avoid the spread of the infection involve covering the nose and mouth while sneezing and coughing, frequent hand washing, boiling eggs and meat thoroughly, and keeping away from close contact with anyone showing the signs of respiratory disease like sneezing and coughing.
2. Methods
As the number of incidences, remedies, and deaths from the disease is changing daily and is being updated based on the rates of diagnosis and reports from different countries, the data in this article are based on the statistics of the reports recorded by the WHO (30 April 2020) to examine the relationship between the incidence rate of the disease and its relation to HDI in different countries (7).
2.1. Human Development Index
The human development index (HDI) that is released by the World Bank gives the newest information on universal growth and involves national, regional, and universal estimations. Based on the human development report, countries are classified into four categories based on human development, including very high, high, moderate, and low classes. The HDI gives a value between zero and one. The human development index allows comparisons between countries. The HDI is a review of measures in human advance. The HDI determines the average success in a nation in three major aspects of human progress, including long and healthy life, access to knowledge, and living standards (8-10).
2.2. Statistical Analysis
The extracted data were analyzed by the bivariate correlation method to evaluate the correlation between the two variables of the prevalence of coronavirus disease and the HDI. The level of significance was set at less than 0.05. The data were analyzed by Stata version 14 software.
3. Results
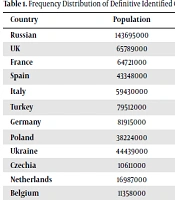
Appendix 1 in Supplementary File shows the number of confirmed cases, new cases, and deaths by country. As can be seen, most cases of coronavirus disease reported by 30 April were in the United States of America (1,003,947 cases), Spain (212,917 cases), Italy (203,591 cases), the United Kingdom (165,225 cases), and Germany (159,119 cases), in sequence.
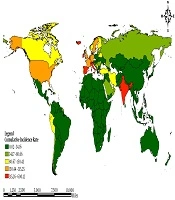
Figure 1 shows the incidence of coronavirus disease per 100,000 population in different countries of the world.
")
Figure 1.
The global map presenting of incidence COVID-19 until 30 April 2020 (7)
Figure 2 shows the incidence of COVID-19 in some countries with high incidence during the last week of April. As can be seen, in all countries, the incidence of the disease is increasing, and the increasing slope in Qatar, and in other countries, the slope is gentle and increasing.
")
Figure 2.
The trend of Incidence of COVID-19 in some countries from 1 to 30 April 2020 (7)
Figure 3 shows the status of COVID-19 disease from 30 December 2019 to 30 April 2020 by WHO region.
")
Figure 3.
Epidemic curve of definite COVID-19 based on the date of the information and WHO districts by 30 April 2020 (7)
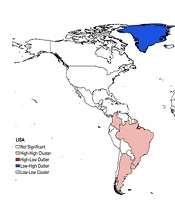
The results demonstrated a significant positive correlation between the Incidence of COVID-2019 and the HDI in the world (r = 0.470, P < 0.0001) (Figure 4).
")
Figure 4.
Correlation between the HDI and COVID-19 incidence on 30 April 2020 (7)
4. Discussion
Human coronavirus is one of the main respiratory pathogens. As two highly pathogenic viruses, MERS-CoV and SARS-CoV cause a severe respiratory syndrome in individuals while four other human coronaviruses (HCoV-HKU1, HCoV-229E, HCoV-NL63, and HCoV-OC43) make mild upper respiratory disease. The main SARS-CoV epidemic infected 8,422 patients between 2002 and 2003 and extended to 29 countries worldwide (11, 12). MERS-CoV spread in the Middle East in 2012 (13, 14).
Phylogenetic analysis revealed that 2019-nCoV belongs to the genus betacoronavirus, which includes (SARS-CoV, bats such as SARS CoV and others) discovered in humans, bats, and other wild animals. In a study carried out in China, patients with COVID-19 had a fever, dry cough, indigestion, and lung involvement in CT scans. Few patients with 2019-nCoV infection showed symptoms in the upper respiratory tract (e.g., rhinorrhea, sneezing, and sore throat) (15).
According to the studies done in China, patients initially presented with a mild cough and low-temperature recurrent fever without any evidence of pneumonia in chest radiography. These nonspecific and mild symptoms in the early clinical period of 2019-nCoV infection may not be clinically detectable from many common infectious diseases of winter (4, 15).
Studies in China showed that 2019-nCoV infections are more common in men . MERS-CoV and SARS-CoV have also been observed more in men than in women (16, 17). The lower susceptibility of women to the viral infection may be related to the protection of the X chromosome and gender hormones that play a considerable role in natural immunity (18). Moreover, about half of 2019-nCoV-infected patients had chronic diseases, mostly cerebrovascular and cardiovascular diseases, and diabetes; it is similar to MERS-CoV in this aspect (16).
Host immune status is also an important factor. Aging, obesity, and comorbidities may be associated with increased mortality. Populations with a poor immune function such as the elderly, diabetics, HIV sufferers, individuals with a long history of using immunosuppressive drugs, and pregnant women are more likely to become infected with 2019-nCoV infection. The immediate use of antibiotics to avoid infection and boost the immune system may reduce the complications, morbidity, and mortality of the disease (19). In laboratory tests, the absolute amount of lymphocytes decreases in most patients. This shows that 2019-nCoV, similar to SARS-CoV, may affect lymphocytes, especially T lymphocytes.
The virus causes a series of immune reactions and changes in white blood cells and immune cells, such as lymphocytes. In some patients with ARDS and septic shock, it progressed rapidly, eventually resulting in multiple organ failure. Therefore, early detection and timely therapeutic actions are extremely important for critical cases (4). The studies showed that saliva contains live viruses and may cause transmission. Respiratory viruses can be transmitted from an individual to another via direct or indirect contact. Saliva is spread through the cough and virus-containing respiratory droplets are found even during normal breathing. Thus, 2019-nCoV may be transmitted directly or indirectly through the saliva even from patients without cough or other respiratory symptoms. Therefore, the use of a mask can be considered a control action (20, 21). Infection control measures should be implemented and health authorities should be informed of cases suspected of COVID-19 (22).