A previously healthy five-year-old boy from a Syrian refugee camp in northern Jordan was transferred to our neurosurgical center from a primary healthcare clinic. Initially, he presented with fever and was diagnosed with bacterial tonsillitis at the camp clinic, where he received a five-day course of intravenous antibiotics. However, his condition worsened, with persistent fever, headaches, and recurrent vomiting.
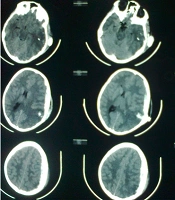
Upon admission to our center, his symptoms included fever, worsening headaches, and vomiting. Hematological investigations revealed a white blood cell count of 19.47 × 103/mm3 with 92% neutrophils, hemoglobin of 12.80 g/dL, platelet count of 485.0 × 103/mm3, elevated ESR (85 mm/hr), and elevated CRP (20.62 mg/L). Other parameters, including renal and liver function tests, were within normal limits. A brain CT scan was performed, showing a deep-seated hypodense lesion in the left thalamus. Subsequent brain MRI characterized the lesion as ring-enhancing and diffusion-restricted, indicative of a brain abscess, with no significant edema or mass effect, and displaying intraventricular extension.
A detailed medical history revealed a possible foreign body aspiration event months earlier. A high-resolution chest CT scan identified a 0.8 × 0.6 × 0.4 cm foreign body in the right main bronchus, later confirmed to be a piece of nut, which was successfully removed via bronchoscopy (
Figure 1).
Initial brain CT and MRI of the thalamic lesion, and chest CT-scan. A, initial axial non-enhanced brain CT scan; B, axial T1-weighted MRI with contrast showing a deep-seated, ring enhancing lesion within the left thalamus; C, axial and coronal chest CT scan, showing the foreign body in the right main bronchus.
The patient underwent frameless stereotactic aspiration of the abscess, yielding 12 cc of pus, which proceeded uneventfully and was followed by an excellent recovery. Microbiological evaluations, including aerobic and anaerobic blood cultures, Gram stain, acid-fast stain, fungal stains, urine culture, sputum culture, and pus cultures, were all negative. Stereotactic aspiration, coupled with a month-long regimen of broad-spectrum IV antibiotics, led to significant improvement in his clinical condition.
Upon admission, initial antibiotic therapy was started immediately with broad-spectrum intravenous antibiotics: Vancomycin 300 mg every 6 hours, ceftriaxone 750 mg every 12 hours, and metronidazole 250 mg every 8 hours. Given the negative pus culture results and the slow response in terms of persistent fever, ceftriaxone was switched to meropenem 600 mg every 8 hours. IV antibiotics were continued for 6 weeks, resulting in a favorable response, with fever resolution, improved headache symptoms, and excellent radiological findings.
A follow-up brain CT scan and MRI performed one month post-surgery confirmed complete resolution of the abscess (
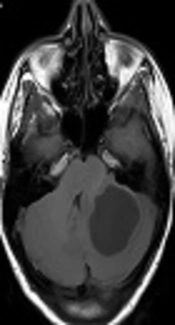
Figure 2). However, on the 36th day of hospitalization, the patient developed sudden onset of right-sided weakness, aphasia, worsening headaches, and recurrent vomiting. An emergency brain CT scan and MRI revealed severe edema in the left temporal lobe, with a 1.5 cm midline shift and signs of uncal herniation (
Figure 3).
Postoperative brain MRI and CT scan: Abscess Resolution. A-C, postoperative MRI scan 1 month after the initial surgery shows complete resolution of the brain abscess [A, T2; B, T1; C, DWI]; D, axial contrast-enhanced CT scan 1-month postsurgery showing complete resolution of the abscess.
Brain CT and MRI at day 36: Temporal lobe edema A, urgent brain CT on the 36th day of hospitalization, depicting massive temporal lobe edema with a midline shift and uncal herniation. B, T2-weighted MRI; C, axial T1-weighted MRI with contrast on the 36th day of hospitalization, depicting massive temporal lobe edema with a midline shift and uncal herniation, with no evidence of abscess recurrence.
Immediate medical management was initiated with administration of dexamethasone, mannitol, and Lasix to control brain edema. However, the patient’s clinical condition deteriorated rapidly, with a decline in consciousness that necessitated intubation, mechanical ventilation, and subsequent left decompressive craniectomy.
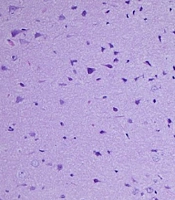
Further extensive investigations, including enhanced brain MRI, magnetic resonance angiography (MRA), and magnetic resonance venography (MRV), ruled out abscess recurrence, arterial or venous abnormalities, and cerebritis. Multiple cerebrospinal fluid (CSF) samples were analyzed and cultured, all yielding negative results. A brain biopsy was taken from the edematous area during the decompressive craniectomy. Histopathological examination ruled out cerebritis, autoimmune encephalitis, and other pathologies, and it was negative for infectious microorganisms on PAS special staining (
Figure 4).
Brain biopsy histopathology histology of H&E stained brain biopsy, showing cortical brain tissue and white matter with no significant pathological changes.
Despite all medical and surgical interventions, cerebral edema persisted, with progressive brain herniation through the craniectomy defect over the following 2 months. This situation necessitated the insertion of a cystoperitoneal shunt in the area of cystic encephalomalacia in the left temporal region, followed by cranioplasty. These procedures significantly improved brain herniation and led to a marked recovery in the patient’s right-sided weakness and aphasia (
Figure 5), resulting in an excellent long-term functional outcome in terms of motor function, speech, and cognitive abilities.
CT and MRI post decompressive craniectomy; A, axial CT scan immediate post decompressive craniectomy; B, axial CT scan 1 month post decompressive craniectomy; C, axial T2-weighted MRI scan 2 months post decompressive craniectomy. Showing progression of the brain edema and herniation of brain tissue through the craniectomy defect; D, axial CT scan post cranioplasty and cystoperitoneal shunt insertion.



![Postoperative brain MRI and CT scan: Abscess Resolution. A-C, postoperative MRI scan 1 month after the initial surgery shows complete resolution of the brain abscess [A, T2; B, T1; C, DWI]; D, axial contrast-enhanced CT scan 1-month postsurgery showing complete resolution of the abscess.](https://brieflands.com/journals/archcid/articles/148927/figures/archcid-148927-g002-F2-preview.webp "Postoperative brain MRI and CT scan: Abscess Resolution. A-C, postoperative MRI scan 1 month after the initial surgery shows complete resolution of the brain abscess [A, T2; B, T1; C, DWI]; D, axial contrast-enhanced CT scan 1-month postsurgery showing complete resolution of the abscess.")