1. Background
Hepatitis A virus (HAV) is a single-stranded, non-enveloped RNA virus from the Hepatovirus genus of the Picornaviridae (1, 2). HAV replicates in liver cells and disturbs liver function, which leads to an immune response and consequently inflammation in liver. HAV is transmitted either by direct contact with an infected individual or contaminated food or water ingestion. The incubation period lasts for nearly 28 days. The HAV fecal shedding rate is greatest in the late incubation period, some days prior to or shortly after the onset of symptoms (3).
Low socioeconomic status, large household size, rural area residence, ethnicity, and unsatisfactory access to healthy water and sanitation facilities are some predictors of past or recent HAV infection (4). The course of HAV infection is age-dependent (5, 6). Young children with an acute infection are conventionally non-specific or asymptomatic and are not diagnosed as HAV infected because of the lack of jaundice. Adults with acute infection could develop mild disease or serious complications. Approximately 80 – 95% of children under 5 years old versus 10 – 25% of adults experience asymptomatic infections (7).
Serum anti-HAV immunoglobulin M (IgM) antibodies, which can be detected immediately after infection and remain detectable for about 6 months or longer, could determine current or recent infection. Past infection can be determined by serum HAV IgG antibodies, which are detectable soon after the onset of symptoms and bring about long-term or even lifelong immunity.
The anti-HAV seroprevalence is declining worldwide (8). The declining rate of HAV infection could be explained in terms of various factors, including enhanced socioeconomic status, increased availability of clean water, and less commonly, a hepatitis A vaccine developed in the 1990s (4). Delayed viral exposure has caused a significant susceptible population to be at risk, as well as outbreaks of hepatitis A. Because the infection severity intensifies as age advances, implementing vaccination programs for certain subpopulations (often children) could be an appropriate strategy for populations with a high proportion of susceptible adults (9). Investigation of hepatitis A seroprevalence is critical in evaluating the appropriateness of a strategy for infection control in a population (10, 11). The hepatitis A vaccine is recommended for children in areas with high and intermediate endemicity, as well as those in the communities at high risk of infections and epidemics (12-14). The hepatitis A vaccination has not been yet incorporated into the routine vaccination programs in Iran. To develop an HAV vaccination protocol in Iran, the seroepidemiology of HAV has been investigated in different regions of the country.
In Tehran, Iran, the seroprevalence of HAV was found to be 61.5% in children (15). Moreover, the seroprevalence rates of HAV in young adults in northeastern Iran and Kashan, central Iran, were reported as 86.8% and 3.9%, respectively (16, 17). In a study of Isfahan, 8.09% of children were seropositive for HAV (18). In addition, studies of Zanjan and Fars obtained HAV seroprevalence rates of 44.3% (in 7 – 10 year-old children) and 88.2%, respectively (19, 20). Saneian et al. demonstrated that 75.3% of first-year medical students at the Isfahan University of Medical Sciences, Iran tested positive for IgG antibody against HAV (5). Moreover, Hoseini et al. showed that the rate of HAV seroprevalence in a group of Iranian young adults was 64% (6).
2. Objectives
In Shahrekord, Chaharmahal and Bakhtiari, southwestern Iran, no data on the seroepidemiology of HAV have been gathered. Therefore, this study was conducted to investigate the seroprevalence and risk factors of HAV in Shahrekord, Iran.
3. Patients and Methods
3.1. Study Population
In this descriptive, analytical, population-based study, a total of 501 participants aged 15 years and older were enrolled from Shahrekord, a city in southwest Iran, during 2013. The study population included both 25 urban and 7 rural areas, with an inclusion criterion for the participants of 15 years and older. Five milliliter blood samples were collected from individuals who met the inclusion criteria using cluster sampling method. The blood samples were centrifuged and the same number of obtained serum samples were kept at -20°C for the next serological experiments.
Demographic characteristics and risk factors, including age, gender, type of residence (rural vs. urban), place of residence, education level, job, number of family members, and sanitation wastewater disposal, were collected using a questionnaire. The study protocol was confirmed by Ethical Committee of Shahrekord University of Medical Science (ethics code: 90-7-5).
3.2. Serological Assay
Serum samples were tested for HAV IgG antibodies using a commercial enzyme-linked immunosorbent assay (ELISA) kit (General Biological Corp, Hsinchu, Taiwan), with a sensitivity and specificity of more than 96%. Serum samples with antibody levels of more than that of the cut-off point were considered positive. All tests were performed by one person.
3.3. Data Analysis
Data were analyzed using SPSS 17 (SPSS Inc., Chicago, IL, USA). The Pearson’s chi-square test and independent t test were run to examine the association between HAV and the study variables. A P value of < 0.05 was considered statistically significance. Logistic regression used to calculate odds ratios (ORs) with 95% confidence intervals (CIs).
4. Results
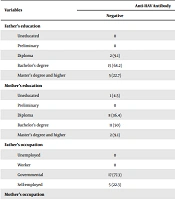
It was found that 455 out of 501 (90.8 %) of the serum samples tested positive for HAV-specific IgG antibody (mean age: 38.9 ± 15.4 years, age range: 15 – 86 years). In this study, 201 out of 501 (42.1%) of individuals were males and 290 out of 501 (57.9%) were females; the HAV seropositivity rates in females and males were 89% and 93.4%, respectively (OR = 0.57 CI: 0.298 – 1.10). There was no statistically significant difference between the seropositivity rate linked to sex (P = 0.096). The mean age of the individuals in the seropositive group was 40.5 ± 15.1 years, while that in the seronegative group was 23.3 ± 8.5 years (P < 0.001). The rate of HAV seropositivity was higher in individuals over 35 years of age (96.0%) than in younger individuals (P < 0.001). It was also higher in married (95.5%) than in the single (76.7%) individuals (P < 0.001, Table 1). The HAV seroprevalence rates among the three ethnic groups-Turk (95.7%), Lur (98%), and Fars (87.8%)-were significantly different (P < 0.05). The rates of anti-HAV-specific antibody in different educational categories, including uneducated, less than a diploma, diploma, more than a diploma, were 97.7%, 93.4 %, 86.9% (OR = 0.156, CI: 0.035–0.687), and 83.3% (OR = 0.118, CI: 0.024–0.568), respectively. There was a significant association between the HAV seropositivity rate and level of education (P < 0.05). The seropositivity rates in urban and rural areas were 89.9% and 94.9% (OR = 2.1, CI: 0.63–6.98), respectively. There was no significant difference between HAV seropositivity and life situation, sanitation, or family size in the individuals studied (P > 0.05).
Table 1.
Seroprevalence and ORs of the HAV Antibody According to Demographic Characteristics and Risk Factorsa
| Demographic Characteristics | Seropositive | Seronegative | Total | Odds Ratio (CI95%) | P Value b |
|---|---|---|---|---|---|
| Gender | |||||
| Male | 197 (93.4) | 14 (6.6) | 211 (42.1) | 1 | Ref |
| Female | 258 (89) | 32 (11) | 290 (57.9) | 0.573 (0.298, 1.103) | 0.096 |
| Age group, y | |||||
| 15 – 24 | 70 (68) | 33 (32) | 103 (20.7) | 1 | Ref |
| 25 – 34 | 126 (94) | 8 (6) | 134 (27) | 7.42 (3.25, 16.95) | < 0.001 |
| 35 – 44 | 93 (98.9) | 1 (1.1) | 94 (18.9) | 43.8 (5.85, 328.3) | < 0.001 |
| 45 – 54 | 76 (98.7) | 1 (1.3) | 77 (15.5) | 35.8 (4.77, 268.9) | 0.001 |
| > 54 | 87 (97.7) | 2 (3.3) | 89 (12.5) | 20.5 (4.75, 88.4) | < 0.001 |
| Type of residence | |||||
| Urban | 383 (89.9) | 43 (10.1) | 426 (87.8) | 1 | Ref |
| Rural | 56 (94.9) | 3 (5.1) | 59 (12.2) | 2.1 (0.63, 6.98) | 0.108 |
| Marriage | |||||
| Single | 89 (76.7) | 27 (23.3) | 116 (23.7) | 1 | Ref |
| Married | 357 (95.5) | 17 (4.5) | 374 (76.3) | 6.37 (3.32, 12.2) | < 0.001 |
| Education | |||||
| Uneducated | 85 (97.7) | 2 (2.3) | 87 (17.6) | 1 | Ref |
| Less than diploma | 142 (93.4) | 10 (6.6) | 152 (30.8) | 0.334 (0.072, 1.561) | 0.163 |
| Diploma | 133 (86.9) | 20 (13.1) | 153 (31) | 0.156 (0.035,0.687) | 0.014 |
| More than diploma | 45 (83.3) | 9 (16.7) | 54 (11) | 0.118 (0.024, 0.568) | 0.008 |
| Bachelor’s degree or higher | 42 (89.4) | 5 (10.6) | 47 (9.5) | 0.198 (0.037, 1.062) | 0.059 |
| Ethnicity | |||||
| Fars | 280 (87.8) | 39 (12.2) | 319 (65.6) | 1 | Ref |
| Turks | 111 (95.7) | 5 (4.3) | 116 (23.9) | 3.09 (1.19, 8.05) | 0.021 |
| Lurs | 49 (98) | 1 (2) | 50 (10.3) | 6.8 (0.92, 50.8) | 0.061 |
| Sanitation wastewater | |||||
| Yes | 405 (90.4) | 43 (9.6) | 448 (91.2) | 1 | Ref |
| Disposal | |||||
| No | 40 (93) | 3 (7) | 43 (8.8) | 1.42 (0.42, 4.77) | 0.575 |
aValues are expressed as No. (%) unless otherwise indicated.
bP value is significant at the 0.05 level.
5. Discussion
In this descriptive study, we investigated the seroprevalence of HAV among individuals older than 15 years from both urban and rural areas of Shahrekord, Chaharmahal and Bakhtiari province, southwest Iran. We found a general seroprevalence of 90.8% in the studied population, which is nearly consistent with the studies of other parts of Iran (5, 6, 19, 21-23). In a cross-sectional study of Fars province, the HAV IgG antibody was reported to be positive in 88.2% of the studied population (19). In a population-based study, HAV seroprevalence rates of 85%, 99%, and 96% were obtained in the northern, central, and southern regions of Iran, respectively (23). A study in northeastern Iran showed a seroprevalence of 86.8% in young adults (16). The seroprevalence of HAV in a group of Iranian teenagers aged 10 - 18 years was 64% (6).
Developed countries have low anti-HAV rates, while Latin America, Asia, and the Middle East have relatively high anti-HAV seroprevalence (4). Socioeconomic variables are thought to be associated with this seroprevalence. Rapidly improving life conditions and sanitation are associated with a rapid decrease in anti-HAV prevalence. Access to clean water, a higher human development index, and greater per capita gross domestic product are negatively associated with HAV infection rates (8).
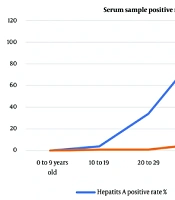
We observed that the younger age groups had a significantly lower prevalence in Shahrekord. In a prevalence study in Iranian with age ranged 10 - 18 years, the seroprevalence of HAV increased sharply from 14·8% at age 10 years to 72.9% at age 13 years, without a significant increase up to age 18 years (6). In Fars province, a seropreva-lence was 79.3% in participants under 20 years of age, 91.3% at 20 - 30 years, and 99% at over 30 years of age (19). Moreover, the seroprevalence of HAV in children increased in older ages in Tehran (15). In this study, we did not include the population of children younger than 15 years old, but the HAV seropositivity has been reported to be 3.9% in children aged 1 - 15 years in Kashan (17). In an investigation of Isfahan, 8.09% of children were found to be HAV seropositive (18), and in Zanjan, the seroprevalence of HAV was 44.3% in 7 - 10 year-old children in 2007 (20).
We also determined the seroprevalence of HAV in five educational groups in this study. The seroprevalence of HAV antibody was lower in participants with higher educational levels. A high prevalence of HAV has frequently been considered indicative of poor hygiene and/or low socioeconomic status (4, 8). It is sensible that higher education level would lead to better socioeconomic status and stricter adherence to health recommendations, resulting in a lower likelihood of exposure to HAV.
Another finding of this study was that a significantly higher rate of HAV seropositivity was evident in married individuals. Previous studies in Iran have failed to consider such an association, with the exception of Merat et al.’s population-based study, in which a higher seroprevalence of HAV was found in married individuals than in single ones (23). This could be explained by the fact that married individuals usually have more social and household contacts; hence, they are expected to have greater exposure to HAV.
Based on our results, the high HAV seroprevalence of 90.8% indicates that a vaccination program is not necessary in our region at the moment. However, more comprehensive data on HAV seroprevalence in relation to demographic characteristics in Chaharmahal and Bakhtiari provinces seem to be required to determine the policy for future HAV preventive measures.