









1. Introduction
The caspase recruitment domain containing protein 9 (CARD9) deficiency is a primary immunodeficiency disorder affecting the innate immune system, resulting in increased susceptibility to fungal infections (1). The innate immune system is the first line of defense against a wide spectrum of fungal pathogens and initiates the production of cytokines by polymorphonuclears (PMNs), which leads to a Th1/Th17 cell response (2-4). Several C-type lectin receptors (CLRs) including, dectin-1, dectin-2, and macrophage-inducible C-type lectin (Mincle) lead to the activation of NF-κB family of transcriptional factors through Syk or CARD9 pathways for cytokine production (5).
Mutations in numerous key genes involved in CLR signaling pathways have been demonstrated to cause primary immunodeficiencies in humans (6). CARD9 is essential for signal transduction in CLR pathways. Analysis of a murine Card9−/− model showed a loss of function mutation that impairs innate signaling from the antifungal pattern recognition receptor that identifies the β-glucan component of fungal cell walls (7). CARD9 deficiencies are clinically indistinguishable and patients with CARD9 defects are susceptible to recurrent and severe fungal infections, including chronic mucocutaneous candidiasis (CMC), dermatophytosis, phaeohyphomycosis, aspergillosis, and protothecosis (3, 8-12). We described progressive disseminated phaeohyphomycosis caused by a melanized fungus in a 26-year-old previously healthy female with inherited CARD9 deficiency to highlight one presentation of this disorder.
2. Case Presentation
A 26-year-old healthy Iranian female was admitted to the Department of Infectious Diseases, Tehran University of Medical Sciences, Tehran, Iran, with cutaneous lesions and localized dermatitis affecting the neck and face (Figure 1A and 1B). A singular, well-defined lesion with purulent secretions had developed gradually over a period of eight years. The initial diagnosis was sarcoidosis at that time and empirical treatment with a steroid (triamcinolone (4 mg/day)) was started for one month during the hospitalization. The infection deteriorated leading to severe dissemination of lesions to the skin of face, chest, and legs. Skin biopsies examined in KOH 10% showed septate and pigmented hyphae, but no muriform cells or granules (hallmark of chromoblastomycosis and mycetoma, respectively).
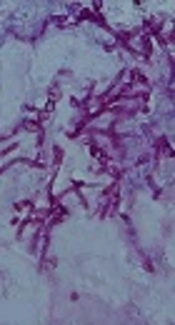
, × 400)")
A and B, Clinical manifestation of the current case; C, a granulomatous infiltrate with irregular, branched and melanized septated hyphae (hematoxylin and eosin (H and E), × 400)
Despite surgical excision and antifungal therapy, the number of the lesions increased nine months prior to admission (Figure 1A and 1B). On admission, full blood analysis revealed Hb 10.5 g/dl, WBC 17,100/mm3, RBC 3.2 × 106/mm3, HCT 23.7%, MCV 73.37 fL, MCH 23.22 pg, RBC ratio to Hb: 1/3, and MCHC 31.65 g/L. Serum electrolytes and liver functions were within normal ranges. In addition, HIV and hepatitis C antibodies were negative. There were no clinical signs and symptoms of neurological involvement. The patient did not remember any history of trauma or puncture at the sites of infection.
The tissue samples were inoculated onto Sabouraud Dextrose Agar (SDA, Difco) and brain heart infusion agar with 5% sheep blood (BHI; Oxoid Ltd., Basingstoke, Hampshire, England) and incubated at 27°C and 37°C for two weeks in the dark but cultures remained negative. Other biopsies prepared for histopathology showed a granulomatous infiltrate with irregular branched and melanized septated hyphae (Figure 1C). The diagnosis of severe fungal infection due to melanized fungi was made on the basis of the clinical and histopathological findings.
Treatment with intravenous amphotericin B deoxycholate (0.5 mg/kg/day) combined with oral voriconazole (400 mg/day) was started. However, her condition deteriorated rapidly with aphasia, dysphoria, and a worsening of the right limb weakness. Due to the absence of immunosuppressive conditions, treatment failure with potent antifungal drugs, and history of consanguineous marriage, a primary or secondary immune dysfunction was considered. Written informed consent was obtained from the patient’s next of kin for whole exome sequencing. Genomic DNA was extracted from peripheral venous blood samples using the Gentra Puregene Blood DNA isolation kit (Qiagen, Hilden, Germany) according to the manufacturer’s instructions. Polymerase chain reaction (PCR) amplification and sequencing were performed by Sanger sequencing on an ABI 3730 DNA sequencer (Applied Biosystems, Torrance, California, USA). A homozygous c.C883T mutation in exon 6 at codon 295, a nonsense variant (Q295X) was identified.
Ultimately, despite combination antifungal therapy, the patient died 38 days after admission because of respiratory failure. No therapeutic drug monitoring was performed. To obtain an etiological diagnosis, DNA was extracted from a formalin-fixed paraffin-embedded tissue using the tissue DNA isolation kit (Qiagen) according to the manufacturer’s instructions. PCR amplification and sequencing were performed for ITS rDNA and D1/D2 regions (9), but due to the lack of sufficient tissue for examination, we failed to identify the cause of the phaeohyphomycosis despite extensive efforts.
3. Discussion
Inherited CARD9 deficiency is a well-known primary immunodeficiency disease, which leads to defects in antifungal defense mechanisms. Unusual and severe fungal infections can be a sign or complication of CARD9 deficiency. It commonly presents with deep dermatophytosis and invasive Candida infections (8, 10). This study described a case of progressive disseminated phaeohyphomycosis in a 26-year-old healthy woman with a nonsense Q295X mutation (c.883C>T) in the caspase recruitment domain protein. There are more reported cases of fungal infection with CARD9 deficiency from Iran (n = 10) than from other Asian countries (9, 13, 14, 15). The total number of Iranian patients has been summarized in Table 1.
| No. | Age/Sex | Year | Fungal Infection | Length of Infection | Causative Agent(s) | Nucleotide Change | Amino Acid Change | Treatment | Clinical Evolution | Reference |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 19/M | 2009 | Oral candidiasis | 16 y | Candida albicans | c.883C>T | HMZ Q295X | KCZ | Cured | (9) |
| 2 | 19/M | 2009 | Candida meningitis | 18 y | Candida albicans | c.883C>T | HMZ Q295X | - | Died | |
| 3 | 50/F | 2009 | Vaginal candidiasis, dermatophytosis | 8 y, 5 y | Candida albicans, Dermatophyte spp. | c.883C>T | HMZ Q295X | - | - | |
| 4 | -/F | 2009 | Oral and vaginal candidiasis, tinea corporis | - | Candida albicans, Dermatophyte spp. | c.883C>T | HMZ Q295X | - | Cured | |
| 5 | -/M | 2009 | Dermatophytosis | - | - | c.883C>T | HMZ Q295X | - | Cured | |
| 6 | 15/F | 2009 | Chronic and invasive candidiasis | -, 2 y | - | c.883C>T | HMZ Q295X | - | Died | |
| 7 | 15/F | 2009 | Chronic candidiasis and Candida meningoencephalitis | -, 0.5 y | - | c.883C>T | HMZ Q295X | - | Died | |
| 8 | 26/F | 2015 | Disseminated phaeohyphomycosis | 8 y | Exophiala spinifera | c.GAG967-969del | HMZ E323del | - | Cured | (13) |
| 9 | 28/M | 2015 | Meningoencephalitis | 11 y | Candida glabrata | c.G104A | HMZ R35Q | FCZ, ICZ | Cured | (14) |
| 10 | 26/F | - | Disseminated phaeohyphomycosis | 8 y | Melanized fungus | c.883C>T | HMZ Q295X | VCZ, AMB | Died | Current case |
Overview of 10 Reported Cases of Severe Fungal Infection Related to CARD9 Deficiency
Consanguineous marriages may be the reason for the high prevalence of CARD9 deficiencies in Iran. Although consanguineous marriages are common in the Middle East (16), severe fungal infections related to CARD9 deficiency were only reported from Iran and Turkey (13, 14). The higher incidence of this immunodeficiency with fungal infection in comparison to other Middle Eastern countries might be associated with rapid population growth, large family size, and the availability of diagnostic facilities.
The homozygous nonsense mutation, Q295X, is the most frequent among Iranian patients (n = 8, 80 %). Although Iranian patients with the Q295X mutation are highly susceptible to candidiasis (n = 7) and dermatophytosis (n = 3), our patient is the first report of phaeohyphomycosis related to Q295 mutation. The relationship between CARD 9 mutations and fungal infections is important in better understanding the pathogenic mechanisms underlying these infections. Severe opportunistic fungal infections are a major cause of mortality in patients with primary immunodeficiency disease. Therefore, patients with prolonged or severe fungal infections without other explanations should be evaluated for CARD9 mutations.
