1. Background
The global burden of sedentariness has been compared to that of obesity and smoking. Evidence has shown that physical inactivity contributes to more than 5.3 million deaths worldwide (1). Report cards on physical activity (PA) for children and youth indicate a worldwide trend of children becoming less active (2-4). Sedentary activities have contributed to the reduction of PA among children, with the most common sedentary activities identified as watching television and playing video games. Pratchett (2005) reported that 75% of UK children and adolescents play three to seven 1.9 hour sessions of video games per week (5).
This mass appeal for video games among children has led to exergaming, technology designed to capitalize on the reinforcing effects of video games to increase PA through a variety of body movements such as jumping, kicking, punching, and ducking (6). The physical effects (energy expenditure, heart rate, and perceived exertion) of exergaming have been compared to moderate-intensity walking (5.7 kilometers per hour (km/h)) in normal weight children (10-13 years) (7).
Furthermore, unlike traditional exercise, exergaming has been linked to stimulating feelings of enjoyment that may contribute to greater adherence in a PA program, often a PA barrier among overweight and obese populations. Jakobsson (2011) explains that exergaming stimulates feelings of enjoyment through virtual rewards that provide a perception of competence, leading to feelings of accomplishment (8). This is in line with a study in Canada that demonstrated that participants in the exergaming group attended 30% more frequently than participants in the traditional training group (9).
The unique benefits of exergaming have been well documented in the literature; however, it remains unclear whether exergaming can induce favorable health-related outcomes among overweight and obese children.
2. Objectives
The purpose of the current study is to investigate the effects of a six-week exergaming program on body composition and cardiovascular fitness among overweight and obese children.
3. Methods
3.1. Participants
Thirty-one overweight and obese children (11.40 ± 0.86 years) were recruited from three primary schools in KwaZulu Natal, South Africa. Participants were randomly assigned to either an exergaming group (n = 11), a traditional gaming group (n = 10), or a control group (n = 10) using a schedule generated from a random numbers table. Eligible participants were between 9 and 12 years old with a body mass index (BMI) above the 85th percentile. Signed informed assent and consent forms were obtained from the participants, and their parents or guardians and participants were allowed to discontinue participation at any time. This investigation was approved by the Institutional Review Board at the University of Zululand and abided by the guidelines set out by the declaration of Helsinki.
3.2. Procedures
Participants were screened prior to inclusion in the study to ensure that the requirements of being classified as overweight or obese were met (10). Eligible participants’ body composition variables (body mass, body mass index, waist-to-hip ratio) and cardiovascular fitness variables (resting heart rate, resting systolic blood pressure, and peak oxygen consumption) were measured at baseline and the week after completing the six-week intervention by the same technician.
Each participant’s resting heart rate (RHR) and resting blood pressure were measured in the seated position after a five-minute rest with the auscultatory method according to the standards established by the American College of Sports Medicine using a sphygmomanometer and a stethoscope (Nantong Honsun (Co. Ltd, China)). Participants were weighed in kilograms (kg) (to the nearest 0.1 kg) on a calibrated medical scale (Mettler DT Digitol, Mettler-Toledo AG, Ch-8606 GreiFensee, Switzerland) wearing only running shorts. Each participant’s stature was measured in centimeters (cm) (to the nearest 0.1 cm) via a standard wall-mounted stadiometer. Each participant's body mass and stature were used to calculate BMI, which was defined as the ratio of body mass to stature squared, expressed in kilograms per square meter (kg.m-2). Participants completed a 20-meter shuttle run test to obtain indirect VO2peak values (11). Participants were encouraged and guided through the test up to the point where they could not complete the specific level of the test. The latter was recorded as the final result. Peak oxygen consumption (VO2peak) was calculated as VO2peak = 31.025 + 3.238 Speed (km/h) – 3.248 Age (years) + 0.1536 Speed × Age (11). All measurements were taken twice, with the reported value being the average of the measurements.
3.3. Intervention
The exergaming group participants were required to play for 15 minutes at both the Nintendo WiiTM boxing and Nintendo WiiTM hula hooping stations three days per week for six weeks. While a PlayStation 2TM gaming console was made available to the traditional video gaming group participants. The traditional video gaming group had the option to play either a football game (Madden NFL 10TM) and/or a boxing game (Knockout KingsTM) on the gaming console. The latter two games are hand-controlled games that require only finger and wrist movements. Participants in the traditional gaming group were required to play for 30 minutes, three days a week for six weeks. Participation from both intervention groups were monitored using a participation log that each participant had to sign along with the time they started and finished each session. Participants in the control group did not take part in any form of physical activity and were instructed to continue with their usual activities of daily living. This was monitored through regular follow-ups with each control group participant.
3.4. Statistical Analysis
Statistical analysis of the data was completed using the Statistical Package for Social Sciences (SPSS) for Windows version 20.0 (SPSS Inc., Chicago, IL, USA). Analysis of the data consisted of means and standard deviations and t-tests to determine if any significant changes occurred pre- versus post-test within each group. P values ≤ 0.05 were considered statistically significant in the interpretation of the results.
4. Results
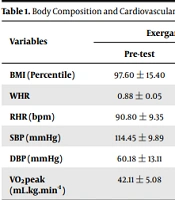
Eleven exergaming (n = 11) and ten traditional video gaming (n = 10) participants completed 18 out of the 18 sessions. The average age at enrollment was 11.40 ± 0.86 years. Table 1 outlines the changes found in each variable from pre- to post-test among the groups.
Table 1.
Body Composition and Cardiovascular Fitness Variables at Pre- and Post-test of Exergaming, Traditional Video Gaming and Control Groups a
| Variables | Exergaming (n = 11) | Traditional Video Gaming (n = 10) | Control (n = 10) | |||
|---|---|---|---|---|---|---|
| Pre-test | Post-test | Pre-test | Post-test | Pre-test | Post-test | |
| BMI (Percentile) | 97.60 ± 15.40 | 98.00 ± 13.23 | 99.50 ± 15.43 | 99.50 ± 14.95 | 99.10 ± 18.20 | 99.20 ± 21.78 |
| WHR | 0.88 ± 0.05 | 0.77 ± 0.18 b | 0.81 ± 0.05 | 0.81 ± 0.06 | 0.83 ± 0.06 | 0.82 ± 0.06 |
| RHR (bpm) | 90.80 ± 9.35 | 81.00 ± 8.30 b | 90.60 ± 11.39 | 85.20 ± 10.70 | 101.45 ± 10.09 | 99.91 ± 9.34 |
| SBP (mmHg) | 114.45 ± 9.89 | 113.00 ± 13.93 | 119.60 ± 13.60 | 117.80 ± 9.65 | 118.30 ± 7.73 | 120.70 ± 5.33 |
| DBP (mmHg) | 60.18 ± 13.11 | 76.00 ± 5.46 | 77.33 ± 10.44 | 73.50 ± 7.84 | 69.00 ± 5.68 | 77.60 ± 11.45 |
| VO2peak (mL.kg.min-1) | 42.11 ± 5.08 | 42.11 ± 5.76 | 39.64 ± 4.04 | 40.32 ± 3.90 | 44.57 ± 3.82 | 42.11 ± 3.92 |
Abbreviations: SD, Standard deviation; WHR, Waist-to-hip ratio; bpm, beats per minutes; RHR, Resting heart rate; mmHg, millimeters mercury; SBP, Systolic blood pressure; DBP, Diastolic blood pressure; VO2peak, Peak oxygen uptake; mL.kg.min-1, milliliters per kilogram per minute.
aValues are expressed as means ± SD.
bIndicates a significant difference (P ≤ 0.05) between pre- and post-test;
No significant improvements were observed in BMI percentile among the exergaming group (P = 0.25), traditional gaming group (P = 0.06) and control group (P = 0.25). Waist-to-hip ratio significantly decreased by 12.50% following exergaming (P = 0.050), while in the traditional gaming group (P = 0.060) and control group (P = 0.200) remained unchanged. The six-week intervention resulted in a significant improvement in RHR of 10.79% in the exergaming group (P = 0.010), compared to the traditional gaming group (P = 0.280) and control group (P = 0.720). After six weeks, no significant improvements were noted in resting SBP following exergaming (P = 0.790), traditional video gaming (P = 0.730) and in the control group (P = 0.610). Diastolic blood pressure did not significantly improve in any of the experimental (exergaming: P = 0.070; traditional video gaming: P = 0.360) or control groups (P = 0.100). VO2peak did not significantly change from pre- to post-test in the exergaming group (P = 0.830), traditional gaming group (P = 0.710) or control group (P = 0.450).
5. Discussion
The purpose of this study was to investigate the effects of six weeks of exergaming and traditional video gaming on body composition and cardiovascular fitness variables among overweight and obese children. The findings indicated that six weeks of exergaming induced favorable decreases in WHR and RHR but not BMI, resting SBP, resting DBP, and VO2peak among overweight and obese children.
Staiano et al. (12) reported comparable findings for body composition in 41 overweight and obese girls (14 to 18 years) who participated in 12 weeks, three hours a week dance exergaming sessions. Similarly, Madsen et al. (13) reported to have found no changes in BMI among 30 overweight children after a six-month Dance Dance Revolution (DDR)TM intervention program. In contrast, Christison and Khan (14) found significant improvements in BMI after 10 weeks of 120 minutes of DDRTM, Nintendo WiiTM tennis, and boxing. The positive effects of exergaming on body composition in the studies by Christison and Khan (14) and Staiano et al. (15) may be attributed to longer interventions (10-weeks and 20-weeks, respectively) compared to this study’s six-week intervention. Furthermore, despite the lack of improvement in BMI percentile in the current study, WHR did significantly improve in the exergaming group. This improvement in WHR in the exergaming group may be ascribed to an increased energy expenditure generated by the exergaming intervention.
The findings on the effect of exergaming on the cardiovascular fitness variables are in line with the findings of Staiano et al. (12), who conducted a 12-week, three hours a week dance exergaming sessions. The significant decrease in RHR is significant since it indicates a heart that functions more economically. Moreover, RHR has previously been correlated with SBP in a large cross-sectional study of 1231 adolescents (16), which demonstrated the importance of decreasing RHR. This is more so vital in overweight and obese children that are prone to developing hypertension.
The non-significant changes found in VO2peak in the present study were similar to the findings of Christofaro et al. (16), who conducted 60 minutes of exergaming training (Sony PlayStation EyeToyTM) on most days of the week for 12 weeks on overweight and obese children). On the contrary, Goldfield et al. (17) found that two 60-minute sessions per week (Sony PlayStation 2TM) resulted in significant improvements in VO2peak after 10 weeks in obese adolescents. The 30 minutes of training used in the present study might not have been a sufficient stimulus to bring about improvements in VO2peak in overweight and obese children. This is confirmed by pediatric guidelines that recommend 60 minutes of daily physical activity to improve cardiorespiratory fitness (18). Also, exercise intensity was not monitored during the exergaming intervention, which could have resulted in the participants training below the intensity threshold required for improving VO2peak.
5.1. Limitations
The current study did not measure exercise intensity during the interventions since it relied on the games themselves to illicit physical activity.
5.2. Conclusions
The findings of this study indicated that six weeks of exergaming induced favorable changes in waist-to-hip ratio and RHR among overweight and obese children. Thereby demonstrating that non-traditional modes of exercise such as exergaming can be used as an alternative to traditional modes of exercise to induce some body composition and cardiovascular changes.