







1. Background
The number of runners increases every year, with overuse injuries of the lower extremity and higher rates of injury being reported compared to other body regions (1), with up to 92% of runners experiencing some form of lower limb injury from running (2). A systematic review showed that the most common site of lower extremity injuries was the knee (7.2 to 50.0%), lower leg (9.0 to 32.2%), the foot (5.7 to 39.3%), and the upper leg (3.4 to 38.1%) (2). The most common overuse injuries reported are patellar tendinopathy, plantar fasciitis, Achilles tendinopathy, and medial tibial stress syndrome (3).
The etiology of running-related injuries (RRI) is multifactorial; and can be divided into three categories, including training (running frequency, duration, intensity, speed, and distance), anatomical (foot type, ankle range of motion, and leg length discrepancy), as well as biomechanical factors (4); with changes in the biomechanics of running being primarily suggested as key factors for RRI (5, 6). From a systematic review of biomechanical factors, evidence supporting the mechanisms of RRI are inconsistent when considering the injuries reported (7). However, ground reaction forces (GRFs) have been speculated as the most important factor associated with RRI (8). Higher impact loading rates during the early loading phase have been reported in injured runners who had been medically diagnosed with injuries when compared to runners without any current or history of injuries (6, 9). In addition, plantar pressure during running is a biomechanical measure that was suggested as a predictive parameter of sustaining an overuse injury (10). This can be explained in part by excessive foot pronation resulting in higher pressure on the medial side of the foot, which in turn has been related to lower leg injuries (11, 12), in particular on the medial aspect of the lower extremities (13) and the plantar fascia (14). Greater foot pronation may be associated with a greater navicular drop which contributes to medial tibial stress syndrome (15). Moreover, low-arched runners seem to experience greater rearfoot eversion excursion, velocity, and a ratio of eversion to tibial internal rotation that could lead to overuse injuries on the medial side of the lower limb (16).
Running is a cyclic movement and requires a bilateral symmetry between lower limbs to reduce injury risk (17), and overloading of one leg will likely occur if there is an asymmetry during running (18, 19). However, Bredeweg et al. (20) reported no differences in the loading between injured and noninjured limbs in novice runners. Furthermore, Hanley and Tucker (21) studied asymmetry of lower limb movements during a 10 km treadmill run. They reported a 1.2% greater symmetry angle which was defined as differences in; step length, step frequency, contact time, flight time, and impact force.
Assessments of side-to-side differences are frequently performed to detect functional deficits by health professionals (22, 23), and the monitoring of the progression of side-to-side differences has also been used to observe the effectiveness of different treatments and rehabilitation programs when considering the readiness to return to sport after injury (19, 24). However, to the best of our knowledge, the presence of side-to-side differences in healthy runners compared to runners with a history of lower limb injuries or runners with a current lower limb injury is yet to be confirmed. Moreover, more studies exploring measures such as; peak vertical GRF, midfoot pressure, foot rotation, and gait variability are needed to better understand their association with the presence, or not, of lower limb injuries in runners. The current study aims to provide a better understanding of the biomechanical presentation associated with the presence of a current or previous injury, with a view to help clinicians develop focused assessments, progressive expectations from rehabilitation programs, and help decision making when considering a return to running practice.
2. Objectives
The primary purpose of the current study was to study side-to-side differences using clinical and running performance assessments of dominant and non-dominant sides in healthy runners (HR), runners with a history of lower limb injuries (RHI), and runners with lower limb injuries (RLI). The secondary purpose was to compare the side-to-side differences between HR, RHI, and RLI groups. The hypotheses were that side-to-side differences would be seen within the RLI and/or the RHI groups, and greater side-to-side differences would be seen between the RHI and RLI groups compared with the HR group.
3. Methods
This was a retrospective study. Data from the running clinic at the Faculty of Physical Therapy at Mahidol University were reviewed.
3.1. Participants
All runners were verbally informed about the study, and those that agreed to their data being used signed a written informed consent form, and the study was approved by the Mahidol University Central Institutional Review Board for Human Research (COA.No. 2019/076.2404).
Forty-nine runners joined an annual running assessment, of which 43 runners met the inclusion criteria and consented to have their data included. The data of 43 runners from those that consented were allocated into 3 groups; 14 healthy runners (HR), 13 runners with a history of lower limb injury (RHI), and 16 runners with a current lower limb injury (RLI) (Figure 1). Participants in the RHI group were defined as previously having a lower limb injury at least 3 months prior to testing with no current pain or symptoms during running. Participants in the RLI group were defined as currently reporting having a lower limb injury, but were excluded if they reported having inflammatory signs, resting pain, or severe pain during the running test. Participants who reported a history or a current injury not in the lower limb, such as low back pain were also excluded.

Participant allocation
3.2. Testing Procedures
Demographic data including general information; sex, age, type of running, running experience, running distance, leg dominance, and history of injury were recorded. The preferred leg for kicking a ball was identified as the dominant leg (25). In addition, the navicular drop height (NDH) test was performed to observe navicular drop from a non-weight bearing or sitting posture to a weight-bearing or standing posture (26). Navicular tuberosity heights were measured from the floor while the runner was firstly sitting on a chair with 90° hip and knee positions and then during standing, and the difference of navicular tuberosity heights between sitting and standing postures was recorded. Previous studies have reported intra-rater ICC(3,1) 0.61 - 0.79 (27) and inter-rater ICC(2,1) 0.48 - 0.97 (28) for the NDH test, and it has been suggested to be a valid indicator of midfoot and rear-foot pronation under static and dynamic conditions (29).
The participants were then asked to perform a running trial on a Zebris FDM-T Treadmill, which has integrated force sensors at a sampling rate of 120 Hz (Zebris Medical GmbH, Germany). The FDM-T has been shown to be a reliable and valid instrument (30, 31) and has been used to study the force distribution during running gait analysis. The FDM-T is fitted with an array of 10,240 miniature force sensors, each approximately 0.85 cm × 0.85 cm, covering an area of 150 × 50 cm. Participants wore their normal sports clothing and footwear. The protocol of a running trial started with a 2-minute walking warm-up at a self-selected speed. Participants were then asked to run for 5 minutes at a speed that was comfortable and matched what they normally used during routine training. Data were recorded from the last 30 seconds of the running test to minimize any effects due to habituation.
3.3. Data Acquisition
All parameters were obtained from Zebris Software analysis. The biomechanical parameters explored included; peak vertical GRF (Newton), midfoot pressure (Newton/cm2), and foot rotation angle (degree). Foot rotation angle was defined as the angle between the longitudinal axis of the foot and the running direction, with negative and positive values of foot rotation defined as internal and external rotations, respectively. These parameters were averaged over the gait cycles recorded during the 30 second data collection period and were recorded for each limb. Percentages of side-to-side differences were then calculated and reported.
Gait variability can be estimated as the standard deviation of the intersection point from a continuous trace of the center of pressure trajectory, which may be useful when exploring differences between runners with and without RRI. The variability of the anteroposterior and medial lateral directions was derived from the butterfly center of pressure diagrams and calculated from the standard deviation at the point of intersection (Figure 2). To gain a greater understanding of symmetry during running, the symmetry using butterfly plots has been suggested as these are simple and easy to interpret (22). The butterfly diagram shows the center of pressure trajectory during gait, which represents running gait variability, stride width, single/double support, and weight shifting symmetry between the lower extremities.
. B is an atypical example of pressure trajectory in a case of history of shin splint")
The butterfly diagram shows the center of pressure trajectory during running. Statistical outcome represents the gait variability in anteroposterior and lateral directions (A). B is an atypical example of pressure trajectory in a case of history of shin splint
3.4. Statistical Analysis
The distribution of the data was tested using the Shapiro-Wilk test, and all parameters were found to be suitable for parametric testing. Dependent t-tests were used to explore any differences between lower-limb sides within each group, and one-way ANOVA tests with post hoc pairwise comparisons were performed to investigate if any differences existed between the HR, RHI, and RLI groups. The statistical significance level was set at P < 0.05, and all testing was performed using SPSS Version 23.0 (IBM SPSS Statistics for Windows, Armonk, NY, USA).
4. Results
Six of the 49 runners were excluded from the study because three runners had incomplete data sets, and three runners had low back pain (Figure 1). The characteristics of the 43 runners included are shown in Table 1. The participants comprised 24 novice and 19 recreational runners. No differences were seen in the average running speed, level of experience, and frequency of running, although the running distance showed that runners with a current injury ran shorter distances than those who had a history of injury and those who had no history of injury.
| Parameter | HR (N = 14) | RHI (N = 13) | RLI (N = 16) | P-Value |
|---|---|---|---|---|
| Sex | ||||
| Male | 6 (43) | 9 (69) | 4 (25) | |
| Female | 8 (57) | 4 (31) | 12 (75) | |
| Age (y) | 32.5 ± 6.3 | 30.4 ± 5 | 30.8 ± 5.6 | |
| Type of runner | ||||
| Novice runner | 8 (57) | 6 (46) | 10 (63) | |
| Recreational runner | 6 (43) | 7 (54) | 6 (38) | |
| Speed (km/h) | 6.6 ± 1.5 | 7.2 ± 2 | 7.3 ± 1.6 | 0.50 |
| Running distance (km) | 8 ± 4.3 | 11.2 ± 6 | 6.1 ± 2.5 | 0.01 |
| Running experience (y) | 2.7 ± 1.3 | 3.7 ± 2.9 | 3.0 ± 3.6 | 0.68 |
| Frequency of running (time/w) | 2.7 ± 1.4 | 3.7 ± 1.3 | 2.9 ± 1.5 | 0.16 |
Characteristics of Healthy Runners (HR), Runners with a History of Lower Limb Injuries (RHI), and Runners with Lower Limb Injuries (RLI) Groups a
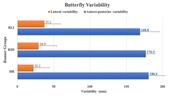
Table 2 shows the comparisons between sides in the three groups. The NDH was significantly different between sides in the HR (P = 0.02) and RHI (P = 0.009) groups. The peak vertical GRF was significantly higher (P < 0.01) on the dominant side when compared to the non-dominant side in the RLI group, however, no significant differences were seen in the percentage of side-to-side differences among the HR, RHI, and RLI groups, and no significant differences were seen between the three groups in all parameters, Table 3. The lateral variability of the butterfly center of pressure diagram in the RLI group was 37.1 mm, which was greater than in the RHI group (28.9 mm) and the HR group (22.2 mm). However, a greater anteroposterior variability was observed in the HR group (180.4 mm) when compared to the RHI group (176.5 mm) and the RLI group (168.8 mm) (Figure 3).
| Parameters | HR (N = 14) | RHI (N = 13) | RLI (N = 16) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Dominant | Non-Dominant | P-Value | Dominant | Non-Dominant | P-Value | Dominant | Non-Dominant | P-Value | |
| Navicular drop height (mm) | 5.6 ± 1.5 (5.0 - 6.5) | 7.1 ± 2.7 (5.5 - 8.8) | 0.020 | 6.2 ± 1.9 (5.1 - 7.4) | 7.5 ± 2.1 (6.2 - 8.7) | 0.009 | 7.3 ± 2.5 (6.3 - 8.6) | 7.2 ± 2.1 (6.3 - 9.3) | 0.900 |
| Peak vertical GRF (N) | 1207.7 ± 238.8 (1072.9 - 1367.5) | 1203.0 ± 241.8 (1061.3 - 1362.5) | 0.790 | 1297.8 ± 282.4 (1127.1 - 1468.4) | 1285.5 ± 272.4 (1120.9 - 1450.2) | 0.510 | 1312.3 ± 228.5 (1162.6 - 1460.7) | 1273.5 ± 232.2 (1117.0 - 1420.0) | < 0.01 |
| Midfoot pressure (N/cm2) | 16.4 ± 3.0 (14.3 - 18.1) | 16.0 ± 3.1 (14.6 - 18.4) | 0.260 | 19.3 ± 5.9 (15.7 - 22.9) | 18.4 ± 6.7 (14.3 - 22.5) | 0.210 | 18.1 ± 6.8 (13.4 - 19.8) | 18.4 ± 6.9 (14.1 - 19.7) | 0.630 |
| Foot rotation (degree) | 8.3 ± 3.9 (7.2 - 11.1) | 9.0 ± 3.2 (6.2 - 10.9) | 0.360 | 9.1 ± 4.1 (6.6 - 11.6) | 8.9 ± 3.6 (6.8 - 11.1) | 0.790 | 9.0 ± 3.4 (7.0 - 10.8) | 7.1 ± 3.4 (5.5 - 9.5) | 0.060 |
Statistical Comparisons of Navicular Drop Height, Peak Vertical GRF, Midfoot Pressure, and Foot Rotation Between Lower Limb Sides in Healthy Runners (HR), Runners with a History of Lower Limb Injuries (RHI), and Runners with Lower Limb Injuries (RLI) Groups (Mean ± SD (95% CI))
5. Discussion
The purpose of this study was to observe the symmetry of lower limbs or the side-to-side differences within clinical and running performance assessments in healthy runners (HR), runners with a history of lower limb injuries (RHI), and runners with a current lower limb injury (RLI). The RLI group had no resting pain but reported symptoms during the running test; however, they were still able to complete the tests even though they reported mild to moderate pain, knowing that they were free to withdraw. Despite running with mild to moderate pain, the RLI group had a slightly higher running speed than the RHI and HR groups, indicating the pain did not limit their running performance, although they did report a significantly lower usual average running distance.
The normal range of NDH is suggested to be less than 10 millimeters (26), and greater amounts of pronation may be associated with a greater navicular drop which has been reported to lead to medial tibial stress syndrome (15). Moreover, runners with low-arched feet seem to experience greater rearfoot eversion excursion, velocity, and a ratio of eversion to tibial internal rotation that could lead to overuse injuries on the medial side of the lower limb (16). In the present study, NDH showed a significant difference between lower limb sides in the HR and RHI groups but showed no significant difference in the RLI group. This was not the same as our first hypothesis, where the current study expected to see significant side-to-side differences on parameters in the RLI and/or the RHI groups, but not in the HR group. This may indicate that the NDH test does not offer any discriminatory insights between injured and noninjured runners. This is supported by Behling et al. (32), who investigated foot pronation during static and dynamic assessments in recreational runners and suggested that linking static assessments to dynamic tasks is not recommended. In addition, Nielsen et al. (33) studied novice runners over a year and found no clear links between high foot pronation and RRI when assessing using the foot posture index.
Previously the NDH has been significantly associated with medial plantar pressure during both static standing and walking in healthy individuals (34). In the present study, slightly less midfoot pressure on both feet was observed in the HR group when compared to the RHI group and the RLI group (Table 2), although this was not significant with similar pressures seen between lower limb sides within all the groups, again offering no discriminatory insights between injured and noninjured runners. It has been reported that the flexibility of the medial longitudinal arch influences the shock attenuation and plantar pressure distributions during running (16, 35). Future studies should consider the specific medial and lateral areas of the midfoot, which may help to offer a better explanation in the plantar loading of runners with RRI.
Peak vertical GRF on the dominant side was significantly higher than the non-dominant side in the RLI group only, although when comparing the HR, RHI, and RLI groups no significant side-to-side differences were seen. Girard et al. (36) investigated limb mechanical asymmetries in physically active males without injury and found that the asymmetry index of peak vertical force was on average 2.5 ± 1.3% between non-dominant and dominant limbs for maximum sprint tests. In the current study, an average of 3.8 ± 3.4% side-to-side difference was observed in the healthy runners. However, the running speed during this current study was less than that reported by Girard et al. The findings of this study support previous studies (18, 19) which also found no significant side-to-side differences in kinetics between noninjured and injured runners. In addition, our findings showed no differences in the peak vertical GRF between limbs in runners with a history of lower limb injuries. This is supported by Zifchock et al. (18, 19), who found no significant differences between sides in the peak vertical GRF in runners with a history of lower limb injuries such as hip bursitis, stress fractures, iliotibial band syndrome, and plantar fasciitis. In the current study, no significant differences between HR and RHI groups were observed, but also between these and the RLI group, which was surprising as the study hypothesized that differences would exist between those with a current injury.
Previously the amount of foot rotation during running tests has not been fully explored. Relative foot position and impact forces may influence the force distributions (37). However, no significant difference between lower limb sides was observed in any of the three groups, with similar amounts of external foot rotation. However, in the RLI group, a trend towards a statistical difference between non-dominant and dominant limbs was observed (P = 0.06). When considering the percentage of side-to-side differences, a greater asymmetry in foot rotation was exhibited in the RLI group (~ 34%) when compared to the RHI group (~ 30.5%) and HR group (~ 24%), (Table 3). This would suggest that more side-to-side differences should be expected from injured individuals, which may be associated with recovery or movement adaptation.
| Parameters | Percentage of Side-to-Side Difference | ||||
|---|---|---|---|---|---|
| HR (N = 14) | RHI (N = 13) | RLI (N = 16) | ANOVA Test | ||
| F | P-Value | ||||
| Navicular drop height | 33.3 ± 30.9 (14.6 - 51.9) | 23.4 ± 24.1 (9.8 - 38.9) | 26 ± 9.6 (20.2 - 31.8) | F (2, 42) = 0.515 | 0.602 |
| Peak vertical GRF | 3.8 ± 3.4 (1.8 - 5.9) | 3.6 ± 3.3 (1.6 - 5.6) | 3.8 ± 2.7 (2.2 - 5.4) | F (2, 42) = 0.093 | 0.911 |
| Midfoot pressure | 6.5 ± 4.7 (3.6 - 9.3) | 11.7 ± 8.9 (6.3 - 17.1) | 10 ± 6.4 (6.1 - 13.8) | F (2, 42) = 2.110 | 0.134 |
| Foot rotation | 24 ± 17.2 (13.6 - 34.4) | 30.5 ± 30.9 (11.9 - 49.2) | 34 ± 19. 1 (22.5 - 45.5) | F (2, 42) = 1.290 | 0.284 |
Statistical Comparisons of Percentage of Side-to-Side Differences on Navicular Drop Height, Peak Vertical GRF, Midfoot Pressure, and Foot Rotation Sides Healthy Runners (HR), Runners with a History of Lower Limb Injuries (RHI), and Runners with Lower Limb Injuries (RLI) Groups (Mean ± SD (95% CI))
The RLI group ran with more side-by-side variation whilst the HR group ran with more anteroposterior variation, which could be one factor that may help identify runners at a greater risk of lower limb injury (Figure 3). In the HR group, the 95% CI of anteroposterior and lateral variabilities were 166.7 - 194.1 mm and 9.1 - 35.4 mm, respectively. These may be useful clinically to monitor progress through rehabilitation. However, in the current study, no significant differences in variability were seen between groups, so further work is needed to confirm the hypothesis that variability is a useful predictive factor to monitor recovery in individuals with RRI.
, runners with history of lower limb injuries (RHI), and runners with lower limb injuries (RLI) groups")
Comparisons of anteroposterior and lateral variability of butterfly diagram among healthy runners (HR), runners with history of lower limb injuries (RHI), and runners with lower limb injuries (RLI) groups
The current study explored gait variability and symmetry during running at the preferred speed for routine training in 3 groups of runners. The results contribute to our understanding of the biomechanical presentation associated with the presence of a current or previous injury. One of the limitations to our current understanding is the variety of types of injuries within our RLI group and RRIs in general, which highlights the need for studies with a sufficient sample size to be able to explore different injury presentations using a variety of clinical assessments. However, this study did not focus on movement changes or compensations which may be associated with different types of lower extremity injury. However, the findings from the exploration of symmetry in this study are still useful to help guide the rehabilitation of RRI, but future studies should include more participants to explore the effects of gender and to increase statistical power.
6. Conclusions
Side-to-side differences should be considered when monitoring injured runners through their recovery and return-to-performance. The assessment of center of pressure variability during running may be one factor to help identify runners at a greater risk of lower limb injury. Runners with lower extremity injuries appear to show more side-to-side variation, whilst healthy runners show more anteroposterior variation. Side-to-side differences should be expected to progressively decrease from the injured stage through the recovery and return to sport phases. Target goals of less than 34% side-to-side difference for foot rotation and 37.1 mm for lateral variability of Butterfly center of pressure diagram may be used to help the decision-making process when considering a return to running practice and to help guide the rehabilitation of RRI.
