



1. Background
Novel coronavirus disease (COVID-19, named by WHO on February 11th, 2020) is a rapidly spreading disease that has first been discovered and reported in Wuhan, China, in 2019 (1). Early findings demonstrated fever and respiratory symptoms like pneumonia and ARDS to be the common manifestations of COVID-19 disease (1, 2). The number of cases has multiplied so rapidly that the outbreak was announced as a pandemic by WHO on March 11th, 2020, as confirmed cases surpassed 110000 cases globally with more than 4000 deaths (3, 4).
Previous studies have reported the person-to-person transmission of the disease through respiratory drops as one of the primary forms of disease transmission (5, 6). The high rate of virus transmission has caused great global concern (7). Many nations have taken severe actions, such as periods of lockdown (8-10), and put limitations on all sporting events to reduce the virus's propagation rate (11). As a result, football matches and training were all suspended until an applicatory method of decreasing infection risk was established (12-14). The Iranian ministry of health and the CORONA headquarters in sports halted all professional football competitions on February 29th, 2020. On May 20th, after league organizations were allowed to resume the matches, the teams began conducting PCR tests on all of their team members, including players, team officials.
To our knowledge, the majority of studies on the clinical characteristics of COVID-19 are focused on hospitalized cases. However, players and team staff face a different pattern of inter-personal contacts in team sports like football; they share the pitch with the opponents and the locker room with their team-mates. Therefore, we believed more data are needed to shed light on the signs and symptoms of COVID-19 infection in the described setting.
Although a recent study addressed the clinical characteristics of infected football players in Qatar (15), more investigations are necessary to better understand the clinical characteristics of COVID-19 in football players during professional football resumption to control the spread of this disease more effectively.
2. Objectives
This study aimed to report the clinical characteristics of COVID-19 in Iranian professional football players and team officials with a first-time positive PCR test after the resumption of the competition while evaluating its impact on team sports using symptom severity and days of training lost due to COVID-19.
3. Methods
3.1. Study Design and Ethics
This questionnaire-based study was conducted under the observation of the Iran Football Medical Assessment and Rehabilitation Center (IFMARC). The study was designed based on the declaration of Helsinki. Given the non-interventional and questionnaire-based nature of the study, no ethical approval was deemed necessary; thus, this study was approved by the Iran football Medical Assessment and Rehabilitation Center (IFMARC) Ethical Committee and Iran Football League Organization. Each participant confirmed his participation in this project by signing the informed consent before starting the questionnaire.
3.2. Study Population
All football players and team officials involved in the premier league and second division league with a positive COVID-19 PCR test were enrolled in this study. Real-time PCR tests were carried out on nasal swab samples starting on May 20th, before the official resumption of team training, and continued until the last official match. All participants were individually asked to fill out the questionnaire. The authors ensured the participants of their privacy and their rights of voluntary participation.
3.3. Data Collection and PCR Testing
According to the guidelines regulated by the CORONA headquarter in sports, team members were tested once every 10 days or if a suspicious symptomatic case was identified.
The results were sent to the league organization to be evaluated at IFMARC. Data collection was followed under the supervision of each team's medical staff. Samples were collected from various Iran regions, depending on the team participating in the study. In case of a positive result, individuals were allowed to return to team practice and football matches 48 hours after the disappearance of all symptoms and obtaining a negative PCR test.
3.4. Questionnaire
Participants were asked to fill in the questionnaire after their symptoms were completely resolved, which was assessed and affirmed by the team physicians. The questionnaire was locally designed to include the most common clinical COVID-19 symptoms reported by the ministry of health such as fever, coughs, dyspnea, etc. Symptoms' severity was assessed using the Likert scale.
3.5. Statistics
The data were statistically analyzed using IBM SPSS Statistics for Windows, version 24.0 (IBM Corp., Armonk, N.Y., USA). Means and standard deviations were used to demonstrate the continuous variables, whereas numbers and percentages were used to manifest categorical variables.
4. Results
4.1. Demographic Data
A total of 113 subjects tested positive for COVID-19 PCR, of which 86 (64.66%) were players and 47 (35.44%) were team officials. No participant was excluded from the study. The mean age was 30.81 ± 10.7 years for total participants (range of 18 - 64 years), with 24.42 ± 4.21 for players and 42.51 ± 8.92 for team officials. No participant reported hospital admission during this study.
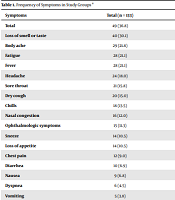
4.2. Frequency, Duration, and Severity of the Symptoms
Among 133 confirmed cases of COVID-19 in this study, 49 (36.8%) experienced symptoms, including 31 players (36%) and 18 team officials (38.3%). The most frequently reported symptom was the loss of smell or taste, with 30.1% in the total study population. Skin lesions, low energy, inability to move, restlessness, and anxiety were among the least frequently reported symptoms, with only 1 participant (0.75%) reporting each. The frequencies of reported symptoms can be found in detail in Table 1.
| Symptoms | Total (n = 133) | Players (n = 86) | Team Officials (n = 47) |
|---|---|---|---|
| Total | 49 (36.8) | 31 (36.0) | 18 (38.3) |
| Loss of smell or taste | 40 (30.1) | 30 (34.9) | 10 (21.3) |
| Body ache | 29 (21.8) | 18 (20.9) | 11 (23.4) |
| Fatigue | 28 (21.1) | 17 (19.8) | 11 (23.4) |
| Fever | 28 (21.1) | 17 (19.8) | 11 (23.4) |
| Headache | 24 (18.0) | 14 (16.2) | 10 (21.3) |
| Sore throat | 21 (15.8) | 12 (14.0) | 9 (19.2) |
| Dry cough | 20 (15.0) | 14 (16.3) | 6 (12.8) |
| Chills | 18 (13.5) | 11 (12.8) | 7 (14.9) |
| Nasal congestion | 16 (12.0) | 13 (15.1) | 3 (6.4) |
| Ophthalmologic symptoms | 15 (11.3) | 8 (9.3) | 7 (14.9) |
| Sneeze | 14 (10.5) | 9 (10.5) | 5 (10.6) |
| Loss of appetite | 14 (10.5) | 7 (8.1) | 7 (14.9) |
| Chest pain | 12 (9.0) | 6 (7.0) | 6 (12.8) |
| Diarrhea | 10 (6.9) | 5 (5.8) | 5 (10.6) |
| Nausea | 9 (6.8) | 6 (7.0) | 3 (6.4) |
| Dyspnea | 6 (4.5) | 4 (4.7) | 2 (4.3) |
| Vomiting | 5 (3.8) | 3 (3.5) | 2 (4.3) |
| Abdominal pain | 4 (3.0) | 2 (2.3) | 2 (4.3) |
| Skin lesions | 1 (0.8) | 1 (1.2) | 0 (0.0) |
| Other: Low energy, inability to move | 1 (0.8) | 1 (1.2) | 0 (0.0) |
| Other: Restlessness, anxiety | 1 (0.8) | 0 (0.0) | 1 (2.1) |
Frequency of Symptoms in Study Groups a
Tables 2 and 3 illustrate the duration of symptoms in days along with symptoms' severity assessed using the Likert scale and reported out of a maximum score of 5 among symptomatic participants, respectively. Symptom duration is demonstrated as mean and standard deviation for each study group. As demonstrated, the most persistent reported symptom was the loss of smell or taste in both groups, with a total mean of 9.15 days. The shortest lasting symptom was reported to be sneezing, with a mean of 1.93 days. As demonstrated in Table 3, a sore throat was reported to be the most severe symptom in players with a mean score of 3.10, as loss of smell was reported to be the most severe symptom in the staff with a mean score of 2.90.
| Symptoms | Total (n = 49) | Players (n = 31) | Team Officials (n = 18) |
|---|---|---|---|
| Loss of smell or taste | 9.15 ± 6.40 | 8.73 ± 6.29 | 10.40 ± 6.93 |
| Fatigue | 6.30 ± 4.71 | 6.50 ± 5.83 | 6.00 ± 2.57 |
| Dry cough | 5.70 ± 4.68 | 4.71 ± 3.87 | 8.00 ± 5.93 |
| Body ache | 5.07 ± 3.83 | 5.22 ± 4.61 | 4.82 ± 2.18 |
| Loss of appetite | 4.57 ± 3.13 | 5.00 ± 3.70 | 4.14 ± 2.67 |
| Chest pain | 4.00 ± 3.33 | 2.83 ± 1.47 | 5.17 ± 4.36 |
| Fever | 3.96 ± 3.04 | 3.59 ± 3.48 | 4.55 ± 2.21 |
| Nasal congestion | 3.88 ± 2.85 | 3.38 ± 2.93 | 6.00 ± 1.00 |
| Ophthalmologic symptoms | 3.60 ± 2.61 | 3.00 ± 2.39 | 4.29 ± 2.87 |
| Chills | 3.50 ± 2.66 | 3.55 ± 3.04 | 3.43 ± 2.15 |
| Headache | 3.29 ± 3.26 | 3.14 ± 3.61 | 3.50 ± 2.88 |
| Nausea | 3.17 ± 2.32 | 3.75 ± 2.75 | 2.00 ± 0.00 |
| Sore throat | 3.10 ± 1.45 | 3.44 ± 1.81 | 2.83 ± 1.12 |
| Dyspnea | 3.00 ± 1.79 | 2.00 ± 0.82 | 5.00 ± 1.41 |
| Vomiting | 3.00 ± 1.22 | 3.33 ± 1.53 | 2.50 ± 0.71 |
| Abdominal pain | 2.75 ± 1.50 | 2.00 ± 0.00 | 3.50 ± 2.12 |
| Diarrhea | 2.00 ± 1.25 | 2.4 ± 1.67 | 1.60 ± 0.55 |
| Skin lesions | 2.00 | 2.00 | - |
| Sneeze | 1.93 ± 2.13 | 1.33 ± 0.50 | 3.00 ± 3.46 |
| Symptoms | Total (n = 49) | Players (n = 31) | Team Officials (n = 18) |
|---|---|---|---|
| Sore throat | 2.74 ± 1.48 | 3.10 ± 1.37 | 2.33 ± 1.58 |
| Ophthalmologic symptoms | 2.60 ± 1.12 | 2.38 ± 1.06 | 2.86 ± 1.22 |
| Fatigue | 2.46 ± 1.32 | 2.76 ± 1.25 | 2.00 ± 1.34 |
| Loss of smell or taste | 2.42 ± 1.37 | 2.27 ± 1.23 | 2.90 ± 1.73 |
| Dyspnea | 2.33 ± 0.82 | 2.50 ± 1.00 | 2.00 ± 0.00 |
| Body ache | 2.32 ± 1.28 | 2.47 ± 1.42 | 2.09 ± 1.04 |
| Chills | 2.17 ± 1.04 | 2.45 ± 1.13 | 1.71 ± 0.76 |
| Nasal congestion | 2.07 ± 0.80 | 2.15 ± 0.80 | 1.50 ± 0.71 |
| Chest pain | 1.92 ± 1.24 | 1.67 ± 0.82 | 2.17 ± 1.60 |
| Loss of appetite | 1.92 ± 0.79 | 1.67 ± 0.82 | 2.17 ± 0.75 |
| Fever | 1.86 ± 1.14 | 1.88 ± 1.11 | 1.82 ± 1.25 |
| Sneeze | 1.86 ± 0.36 | 1.89 ± 0.33 | 1.80 ± 0.45 |
| Dry cough | 1.85 ± 0.81 | 1.64 ± 0.84 | 2.33 ± 0.52 |
| Headache | 1.79 ± 1.06 | 1.79 ± 0.90 | 1.80 ± 1.32 |
| Diarrhea | 1.67 ± 0.87 | 1.80 ± 0.84 | 1.50 ± 1.00 |
| Nausea | 1.33 ± 0.71 | 1.50 ± 0.84 | 1.00 ± 0.00 |
| Vomiting | 1.33 ± 0.58 | 2.00 ± 0.00 | 1.00 ± 0.00 |
| Abdominal pain | 1.25 ± 0.50 | 1.50 ± 0.71 | 1.00 ± 0.00 |
| Skin lesions | 1.00 | 1.00 | - |
4.3. Days Lost to COVID-19
Data were collected using the questionnaire with regards to the number of days of training missed due to suffering from COVID-19. We classified the lost days into 3 categories; the symptomatic period, the quarantined period, and the return to team training period. Table 4 demonstrates the mean duration of symptoms, quarantine days, and days of missing the team training due to COVID-19 in study groups with details of the minimum and maximum reported values. It shows that our population on average has lost 12.89 days to fully return to team practices.
| Periods | Total (n = 133) | Players (n = 86) | Team Officials (n = 47) |
|---|---|---|---|
| Symptomatic | 10.10 ± 5.84 | 10.10 ± 6.16 | 10.11 ± 5.41 |
| Quarantined | 11.47 ± 4.89 | 10.79 ± 5.18 | 12.70 ± 4.10 |
| Return to team trainings | 12.89 ± 7.86 | 12.76 ± 7.28 | 13.13 ± 8.90 |
5. Discussion
This study reported the status of the clinical manifestations of COVID-19 disease in Iranian men’s professional football setting during the resumption of the competitions. Although data is still lacking on the details and impacts of COVID-19 in professional sports, we here discuss the major findings of our report and compare them with the available literature.
Frequency, duration, and severity of the symptoms
In general, we found that the most common symptoms were loss of smell or taste, body aches, fatigue, and fever. The least frequently reported symptoms were gastrointestinal symptoms and skin lesions. These findings are compatible with other studies, including a meta-analysis, in which the most frequent symptoms were reported to be fever, cough, fatigue, while gastrointestinal unrest was found to account for the least frequently reported symptoms (16-19). However, it might be worth mentioning that the proportion of dyspnea was reported higher in the studies conducted on the general population compared to our report (2, 19). The difference in findings may be caused by the general superior physical fitness and cardiorespiratory potential of individuals involved in professional football in comparison to the general population. It was also revealed that the frequency of symptoms was similar in both study groups.
The mean duration of symptoms was 10.1 days, the longest-lasting symptom was the loss of smell and taste in both groups, followed by fatigue in players and dry coughs in team officials. Loss of appetite and chest pain were also among the topmost persistent symptoms. The quickest symptom to resolve was sneezing in players (1.33 days) and diarrhea in team officials (1.6 days).
Sore throat, fatigue, loss of smell or taste, dyspnea, and dry coughs were among the most severe symptoms experienced by the study population. On the other hand, the least severe symptoms comprised gastrointestinal symptoms, headache, and fever.
Limited studies were found to address the duration and severity of symptoms in football players and team staff. However, Khraise et al. (17) reported 13.5 days of illness in a quarantine center. A shorter symptomatic phase among COVID-19 positive football players and staff may indicate the effect of better physical fitness on the COVID-19 course of the disease. Further studies are suggested to address the differences and similarities between the general population and athletes' symptoms more effectively.
5.1. Days Lost Due to COVID-19
Although there has been no previous report on the days lost due to COVID-19 in professional sports, the 12.76 days lost for each player was comparable with sport-specific injuries. Ekstrand et al. (20) reported mean absent days between 13 to 14 days for the following most common injuries in football: ankle medial ligament injury (13.4 days), groin other muscle-related or tendon related pain (13.4 days), groin pain (13.5 days), groin adductor pain (13.5 days) and hip flexor pain (13.8 days). Despite an obvious difference between the nature of COVID-19 disease and other injuries, absence from the competition is a considerable situation for the teams. It affects both the performance and the financial aspects of each team.
On the other hand, it was also revealed that team officials have missed an average of 13.13 days of training due to COVID-19. Given their importance and various roles, losing them could have an undeniable impact on the performance of the team.
5.2. Study Imitations
The authors would like to acknowledge the inevitable limitations in this study, given the study design, which aimed to report the clinical characteristics of COVID-19 in the setting of return to sport protocols, carried out and implemented by the ministry of health and CORONA Headquarters in sports direction during the COVID-19 pandemic, as it happened in Iran. Despite all the limitations, we believe that this report will help further understand the impacts of COVID-19 on individuals in team sports.
5.3. Conclusions
In conclusion, since most of the infected individuals in our population were asymptomatic, proper case identification using regular PCR testing could stop the transmission of the disease more effectively. Also, more attention is required to be paid to less severe symptoms such as the loss of smell and taste. Moreover, the days lost due to COVID-19 are almost comparable to the days lost by other injuries for the players, which highlights the importance of taking proper preventive measures.
