

INTRODUCTION
Kinematic magnetic resonance imaging (KMRI) is a well-known diagnostic method with great potential. It consists of a series of static magnetic resonance (MR) images taken with the target joint flexed at various discrete angles. Investigators can observe structural displacements and distortions of the anatomies of joints or the spinal column including bones, intervertebral discs, neural elements, ligaments, facets, menisci, and tendons by varying their positions. Many studies of KMRI have been performed using permanent or superconducting magnets in horizontally or vertically opened MR systems with relatively low (0.2-0.6 T) magnetic field strengths. Detailed explanations and examples of clinical applications for KMRI were first described in a book edited by Shellock and Powers [1]. Although KMRI has been applied to the lumbar spine [2–8], cervical spine [6–12], knee [13–21], ankle [22–24], shoulder [25–29], and wrist [30–33] and it offers information that often serves to characterize the underlying abnormality or to complement the information acquired with standard static magnetic resonance imaging (MRI), the deterioration of image quality due to the low magnetic field cannot be avoided. Recently, the superconducting, horizontally opened, 1.2 T MR system (OASIS, HITACHI, Tokyo, Japan) has become available commercially, and our facility, JFA (Japan Football Association) Medical Center Hospital, installed the system under a grant from the FIFA (Fédération Internationale de Football Association) goal program in August 2009. This system utilizes the combination of a vertical magnetic field and a solenoid receiver coil, offering higher sensitivity and greater uniformity than the combination of a horizontal magnetic field and a multiarray receiver coil adopted in the standard tunnel-type MR system. This new system enables us to acquire high–quality images (high spatial resolution, tissue contrast, and signal–to–noise ratio) in acquisition times that are nearly the same as those of standard tunnel-type 1.5 T systems, even though the strength of the magnetic field is lower. Therefore, the purpose of this study was to introduce and evaluate the potential of KMRI utilizing a horizontally opened space by means of this high-field open-magnet MR system.
METHODS AND SUBJECTS
Participants
We focused on KMRI of three parts of the body – lumbar spine, knee, and ankle – where sports injuries commonly occur in soccer players. Three healthy female volunteers who are futsal players were recruited and each of them was assigned one of the parts to be examined for this pilot trial. We performed the study according to the Declaration of Helsinki requirements and obtained informed consent from all subjects.
Procedure
We utilized the superconducting, horizontally opened, 1.2 T MR system (OASIS) (Fig. 1a) for KMRI, which was equipped with a higher magnetic field than a conventional 0.2-0.6 T open-type MR system. The bore was widely opened horizontally (270°) and its height was 44 cm. One can easily recognize that the potential for KMRI is higher than that of the conventional tunnel-type bored MR system (Fig. 1b). We performed a qualitative comparison of the quality of KMRI images with those reported in previous studies.
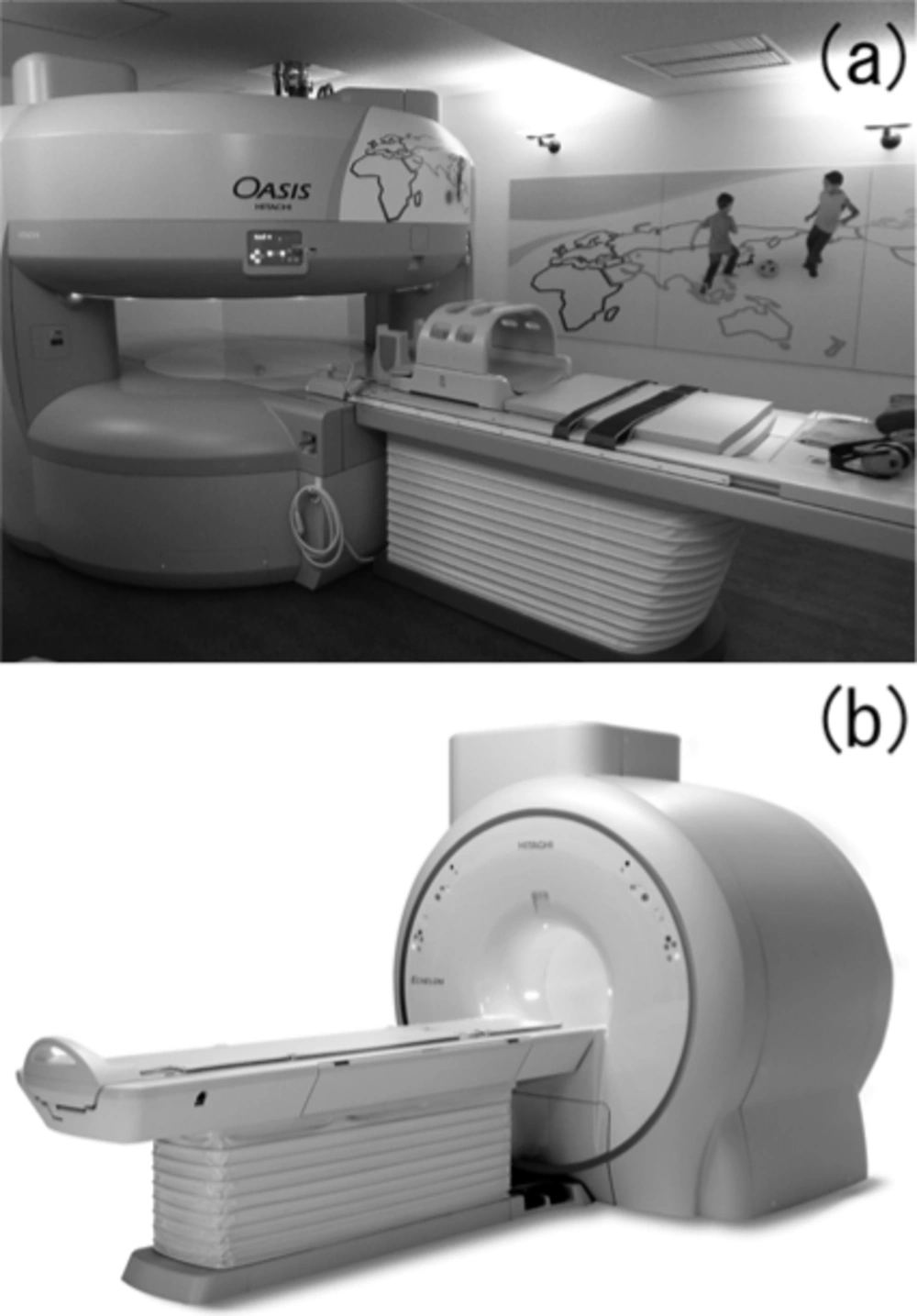
The configuration of two types of magnetic resonance systems: (a) the superconducting, horizontally opened, 1.2 T magnetic resonance system and (b) the conventional tunnel-type, bored 1.5 T magnetic resonance system.
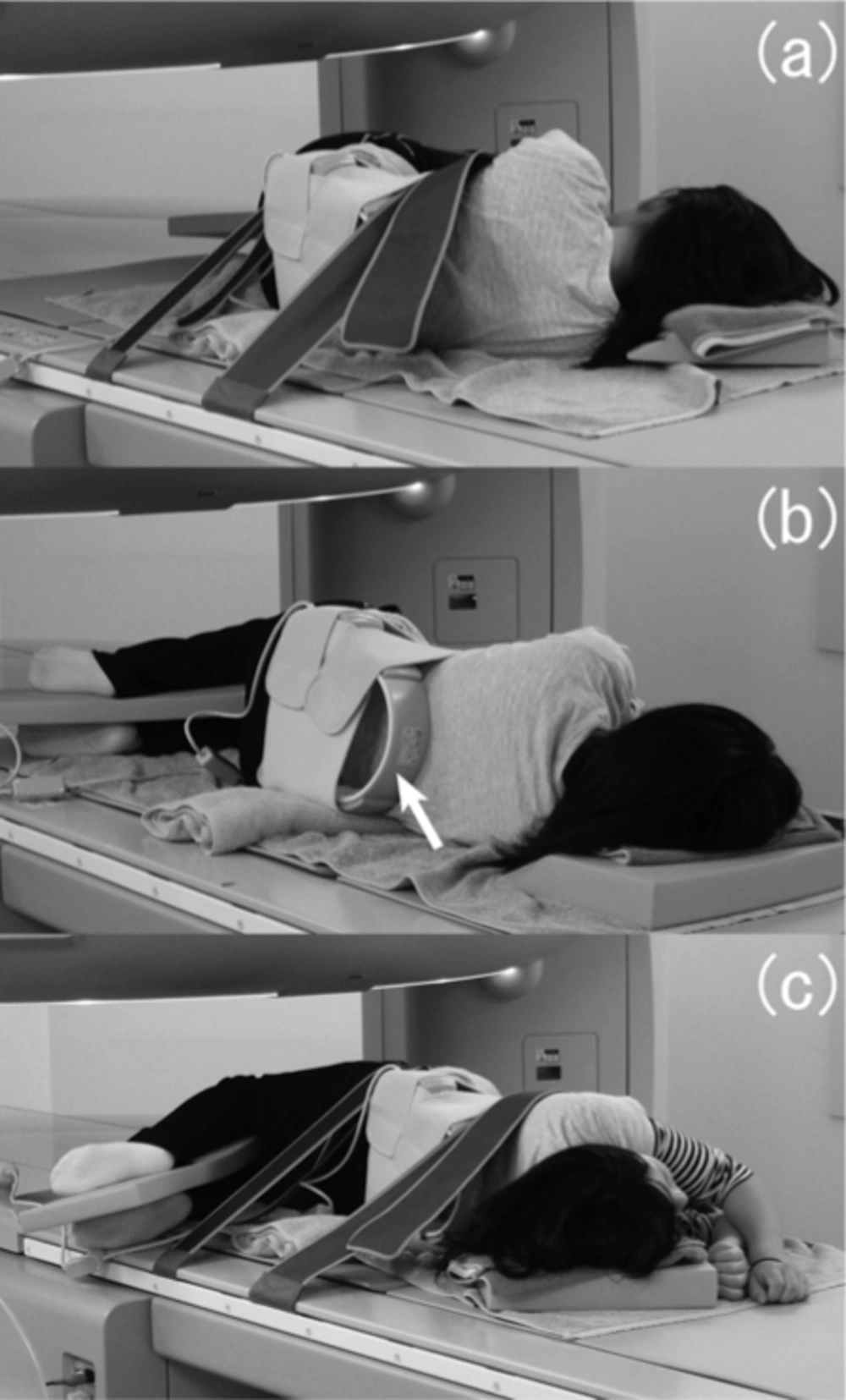
The designated volunteer was required to lie on her right side and maintain maximum anteflexed, neutral, and maximum retroflexed positions for the duration of the acquisition time (TA) for each posture with a solenoid receiving coil put on her back[34] (Fig. 2). The imaging plane was set in the sagittal section and T2-weighted images (T2WI) were acquired using a fast spin-echo (FSE) sequence, which is routinely ordered in spine MRI. The parameters for the FSE T2WI were: repetition time (TR), 2400 ms; echo time (TE), 96.0 ms; echo train length (ETL), 16; number of phase encodes/frequency encodes (PE/FE), 320/352; slice thickness (T), 4.5 mm; slice gap (G), 0.5 mm; number of excitations (NEX), 4; field of view (FOV), 300 mm; reconstruction matrix (Mx), 512*512; TA, 3 min 14 s.
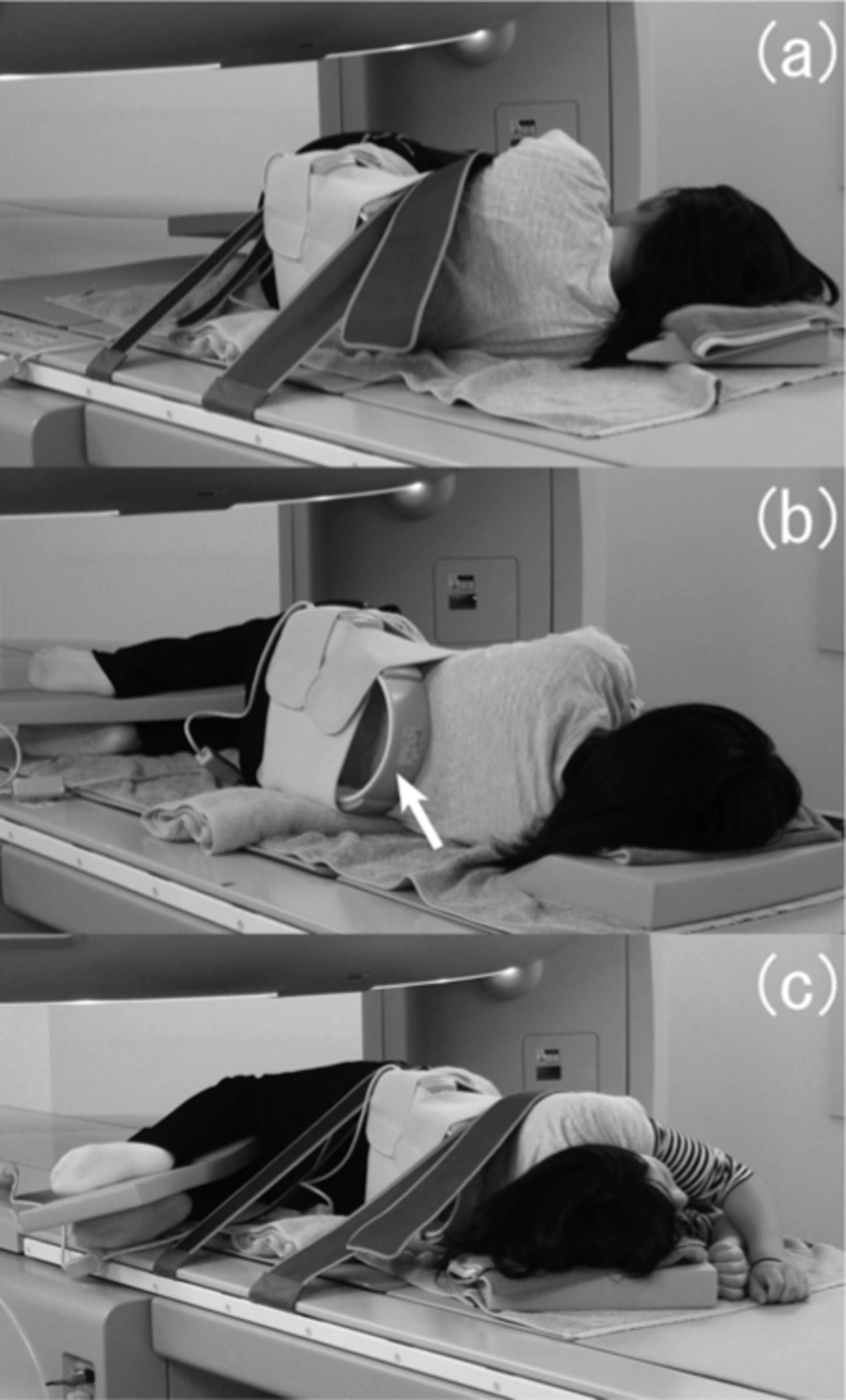
The postures in kinematic magnetic resonance imaging of the lumbar spine: (a) maximally anteflexed, (b) neutral, and (c) maximally retroflexed positions. A solenoid receiving coil was put on the subject's back (arrow).
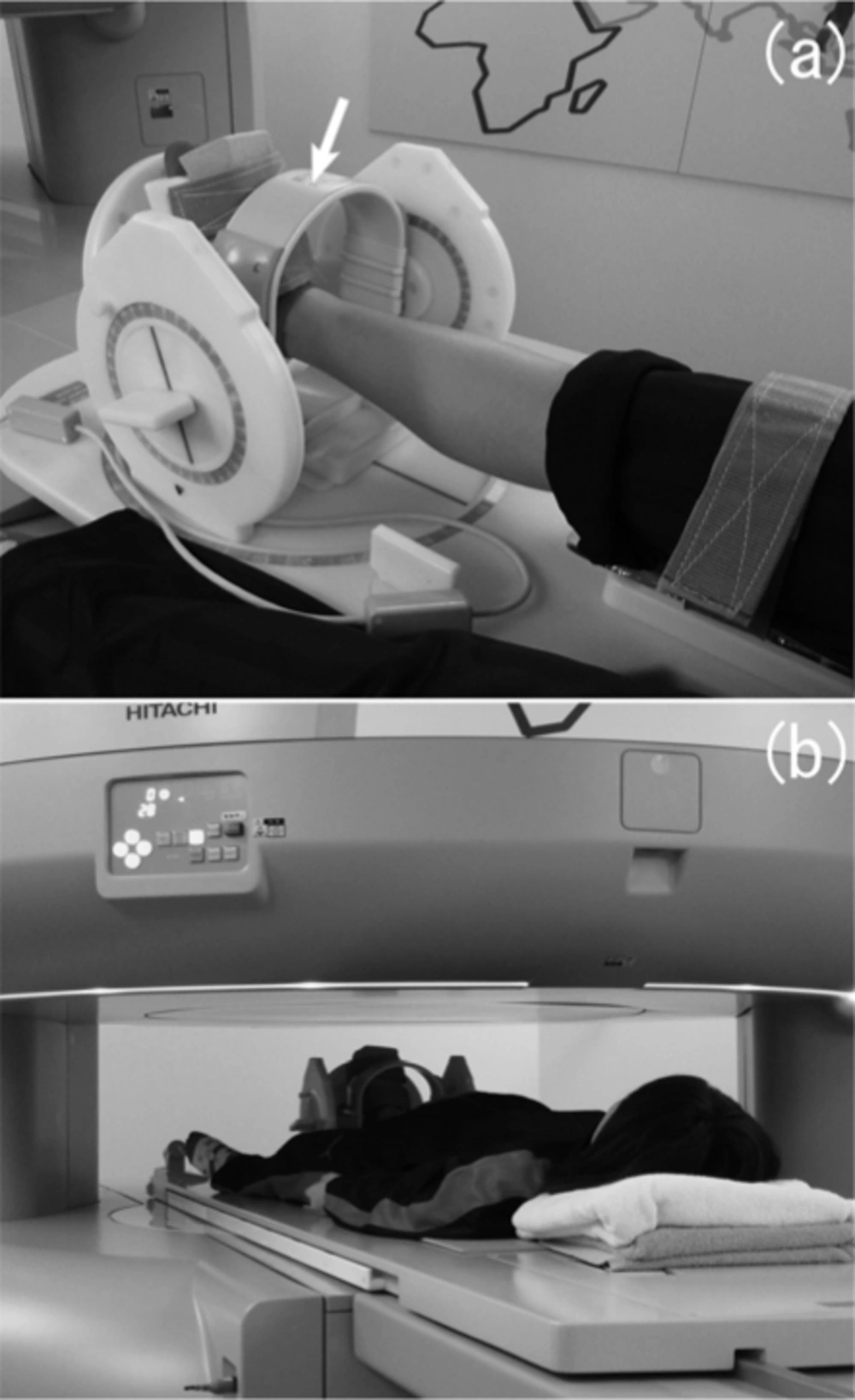
The designated volunteer was laid on her left side while maintaining her right knee in a 0°, 30°, 60°, 90°, or 120° flexion position fixed by a supporting tool (CHAMCO, Inc., Cocoa, Florida, USA) with her knee through the solenoid receiving coil (Fig. 3) during each TA. The imaging plane was set in the sagittal section and proton density weighted images (PDWI) were acquired using an FSE sequence, which is routinely ordered in joint MRI. The parameters for FSE PDWI were: TR, 1500 ms; TE, 12.0 ms; ETL, 3; PE/FE, 320/448; T, 3.0 mm; G, 0.3 mm; NEX, 1; FOV, 150 mm; Mx, 512*512; TA, 3 min 14 s.
The posture in kinematic magnetic resonance imaging of the knee. (a) The fixation of the knee by a supporting tool (CHAMCO, Inc., Cocoa, Florida, USA) and the arrangement of the solenoid receiving coil (arrow) are shown. The knee flexion can be adjusted from 0° to 120°. (b) The subject's position during the image acquisition is shown.
The designated volunteer was laid supine while maintaining her ankle in a maximally dorsiflexed, neutral, or maximally plantarflexed position fixed by a supporting tool (CHAMCO, Inc.) with her ankle through the solenoid receiving coil (Fig. 4) during each TA. The imaging plane was set in the sagittal section and PDWI using an FSE sequence were acquired. The parameters for FSE PDWI were: TR, 1700 ms; TE, 12.6 ms; ETL, 4; PE/FE, 320/384; T, 3.0 mm; G, 0.3 mm; NEX, 1; FOV, 180 mm; Mx, 512*512; TA, 3 min 40 s.
The posture in kinematic magnetic resonance imaging of the ankle. (a) The fixation of the ankle by a supporting tool (CHAMCO, Inc., Cocoa, Florida, USA) and the arrangement of the solenoid receiving coil (arrow) are shown. (b) The subject's position during the image acquisition is shown.
RESULTS
For each of the three volunteers, all KMRI examinations could be performed without any technical failure; there were no issues regarding coil settings, space for examinees to pose, parameter settings for the sequences, and limitations to slice planning.
Representative results of KMRI of the lumbar spine are shown in Figure 5, which includes the slices at the middle plane of the vertebral body and at the level of the intervertebral foramen in maximal anteflexion, neutral, and maximal retroflexion positions. The alignments of the vertebral bodies and spinous processes and the shapes of the intervertebral discs and the vertebral canal according to the differences of the three postures may be observed in the upper images in Figure 5. In the same way, the sizes and shapes of the intervertebral foramina and the kinematics of the facet joints may be observed in the lower images in Figure 5. The kinematic images of the knee at the slice level of the anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), and medial meniscus (MM) are shown with the flexion angle of the knee in Figure 6. The motion of the ACL, PCL, and MM could be depicted clearly with high spatial resolution and adequate signal-to-noise ratio. If one desires, the kinematics of the patellofemoral joint can also be evaluated using these KMRI images.
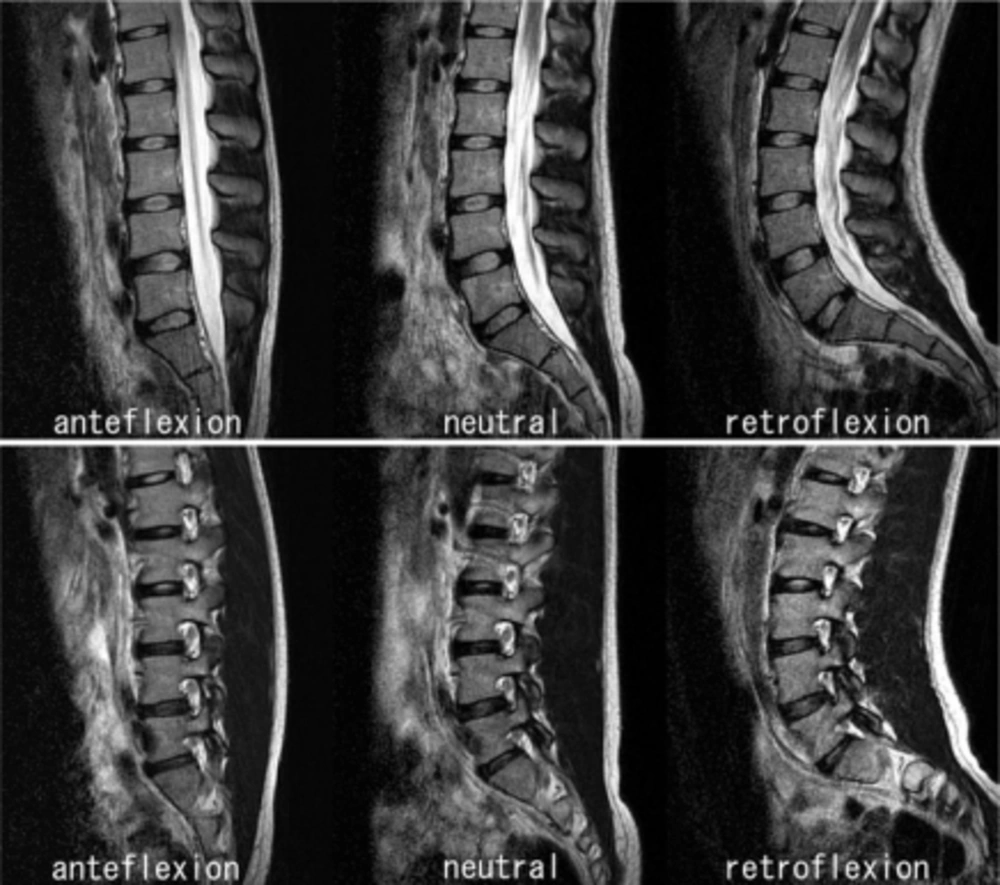
Example of kinematic magnetic resonance images of the lumbar spine. Upper row: slices at the middle plane of the vertebral body. Lower row: slices at the level of the intervertebral foramen. Each of them is arranged from left to right in order of maximal anteflexion, neutral, and maximal retroflexion positions.
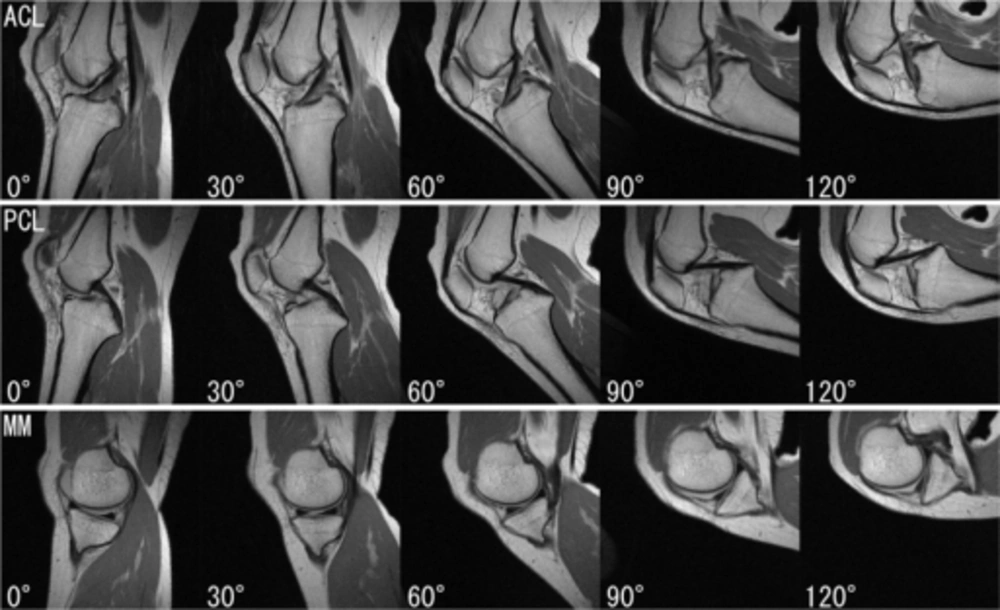
Example of kinematic magnetic resonance images of the knee. Upper row: slices at the level of the anterior cruciate ligament (ACL). Middle row: slices at the level of the posterior cruciate ligament (PCL). Lower row: slices at the level of the medial meniscus (MM). The angle indicated at the lower left of each image is the flexion angle of the knee.
Kinematic images of the ankle in the maximal dorsiflexion, neutral, and maximal plantarflexion positions at the slice level of the central trochlea of the talus (TT) and peroneal tendon (PT) are shown in Figure 7. The movement of the tibiotalar articulation and the location of PT may be observed.
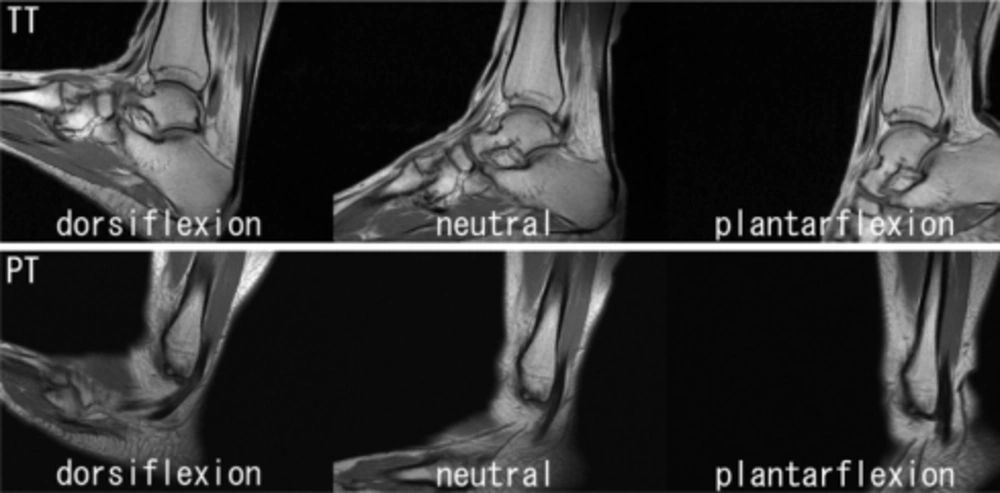
Example of kinematic magnetic resonance images of the ankle. Upper row: slices at the central trochlea of the talus (TT). Lower row: slices at the level of the peroneal tendon (PT). Each of them is arranged in order from left to right of maximal dorsiflexion, neutral, and maximal plantarflexion positions.
DISCUSSION
Many studies on KMRI have been performed in the past 20 years. Most of these have been performed using vertically [3–8,12,14,19,20,28,29] or horizontally [2,16–18,21,24,26,27,34] opened MR systems, or a specified system of KMRI [15], excluding the studies under the small ranges of the joint posture within the bore size of conventional tunnel-type MR systems [13,25], because there are sometimes serious limitations on the poses of subjects in conventional tunnel-type MR systems. Conversely, KMRI of the cervical spine, ankle, or wrist, whose range of motions are relatively tiny, has been performed using a tunnel-type MR system [9–11,22,23,30–33]. Generally, the higher the magnetic field of an MR system is, the higher the resulting image qualities such as spatial resolution, tissue contrast, and signal-to-noise ratio are and the shorter the acquisition time. However, MR systems with higher magnetic fields were available only as tunnel-type systems until recently. Thus, it has been impossible to perform KMRI of the lumbar spine, knee, or shoulder, which requires wide space beyond the size of a tunnel-type MR system's bore, with high-quality images due to the high magnetic field. Therefore, an open MR system with a high magnetic field has been desired for a long time. Finally, such a system has become available commercially, which gives clinicians a way to perform KMRI of those parts of the body, resulting in high-quality images in shorter acquisition times. Short acquisition time is invaluable, particularly in KMRI with postures attended with pain. In this study, acquisition times were over 3 min due to the sequence parameters for high spatial resolution and signal-to-noise ratio. If we set the sequence parameters to acquire the images whose qualities are equal to those acquired by a low field type of MR system, we can shorten the acquisition times.
We performed KMRI of the lumbar spine, knee, and ankle, which are closely associated with soccer players’ injuries, because our facility was established mainly for the treatment of soccer players. In the present study, KMRI of the lumbar spine and knee with high-quality images was performed for the first time in the world (Figs. 5 and 6), although KMRI of the ankle (Fig. 7) has been available using a tunnel-type, high magnetic field MR system. These high-quality KMRI images can not only demonstrate the lesions not visible on conventional MRI but also provide further detailed depiction of abnormalities derived from varying joints or spinal column postures. Those abnormalities include spinal canal and/or intervertebral foramen narrowing caused by deformation of an intervertebral disk and ligamentum flavum, dysfunction of a facet joint apparent in KMRI of the lumbar spine, ligament dysfunction and meniscus deformation apparent in KMRI of the knee, and tendon dysfunction, impingement syndromes, osteochondral defects, and loose bodies apparent in KMRI of the ankle. Although we excluded KMRI of the shoulder from this study, the shoulder can be one of the best candidates for KMRI using a high-field, horizontally opened MR system utilizing the large space of the gantry, which can provide high-quality images of tendons and the glenoid labrum for the diagnoses of rotator cuff tear and shoulder dislocation. Furthermore, we can acquire KMRI images with much higher spatial resolution utilizing a microscopic coil [35] under the high magnetic field, which will enable us to observe minute lesions. However, this high-field, horizontally opened MR system is not complete and there is a critical imperfection in a certain type of KMRI. We cannot perform weight-bearing KMRI with a horizontally opened MR system, although it is feasible with a vertically opened MR system [3–8,12,14,19,20]. The ideal solution for a full KMRI study may be the development of a high-magnetic-field, vertically opened MR system. Nevertheless, the fact that a high-magnetic-field, horizontally opened MR system has become commercially available will lead to progressive improvements in KMRI studies.
CONCLUSION
We performed KMRI of the lumbar spine, knee, and ankle using a high-field, open-magnet MR system. We introduced high-quality KMRI images and evaluated their potential for clinical use. Those KMRI images make possible a detailed depiction of abnormalities derived from varying joints or spinal column postures, including spinal canal and/or intervertebral foramen narrowing and dysfunction of a facet joint apparent in lumbar spine KMRI, ligament dysfunction and meniscus deformation apparent in knee KMRI, and impingement syndromes, osteochondral defects, and loose bodies apparent in ankle KMRI. The results of our pilot trial indicated that a superconducting horizontally opened, 1.2 T MR system offers high-quality KMRI images and can be utilized for the kinematic diagnosis and evaluation of sports injuries.
