

INTRODUCTION
Athletes training at high intensity may present with vague symptoms of cough and fever. As the immune response during high intensity training may be impaired, the usual symptoms of an underlying pneumonia may not be overtly apparent[1, 2]. The clinician must maintain a low index of suspicion of pneumonia in such cases.
CASE PRESENTATION
A 24-year old male elite triathlete presented at a sports medicine clinic five days after an Ironman triathlon race, complaining of lethargy, localised pleuritic chest pain, loss of appetite and race underperformance. On examination he was tachycardic and exhibited decreased lower left lung air entry accompanied by crackling. A chest x-ray was ordered and this revealed a left sided basal pneumonia associated with a para-pneumonic effusion (Fig. 1). His blood investigations were unremarkable with a white cell count of 7.7, neutrophils of 4.18, eosinophils of 0.82, lymphocytes of 2.09, erythrocyte sedimentation rate (ESR) of 21 and a C-reactive protein (CRP) of 9. Besides, his pneumonia severity index was <51[3] (lowest risk group). Hence, he was treated on an outpatient basis and was prescribed oral cefuroxime 500mg BD for one week, to which he responded well.

Fig. 1
Chest X-ray showing left basal pneumonia with para-pneumonic effusion (arrow)
Course of the Illness
This triathlete's medical episode started eight weeks prior to his Ironman race (3.8km of swimming, 180km of biking and 42.2km of running), when during intense training runs he started complaining of recurrent interscapular pain in deep inspiration. Two weeks later, after completing training sessions that lasted more than five hours, he developed a fever of up to 40°C. The fever subsided within an hour following administration of self-prescribed oral paracetamol 1g.
Two to three weeks prior to the event he developed a persistent dry cough and decreased appetite, associated with an unremitting fever of 39°C, unresponsive to paracetamol. The symptoms were accompanied by shortness of breath on exertion, lethargy and left sided pleuritic chest pain. There was no relevant previous medical history, including no previous respiratory conditions. His family physician prescribed oral co-amoxiclav 1g BD for one week. He responded well to this antibiotic.
On race day, the triathlete had an uneventful swim and the initial bike segment went smoothly, adhering to his pre-planned race schedule. However, after 120km on the bike segment he felt unusually lethargic and by the 13th km of the running segment he developed bouts of loose watery diarrhoea, causing him to stop at approximately every 3km.
He reported having chills and rigors, despite an ambient temperature of around 22°C and he resorted to walking the route in order to complete the race. His diarrhoea settled spontaneously on completion of the race, and no medications were ingested. Following the chest X-ray findings and the cefuroxime regime, blood investigations were repeated after two weeks, showing a white cell count of 6.0 (neutrophils 2.8, eosinophils 0.4), ESR 4, CRP <6.
After 8 weeks of recovery, the triathlete started training gradually at intensities that were initially less than 60% of his maximum heart rate. These training sessions were incrementally increased in duration and frequency following a set training programme agreed with the treating sports physician. A chest CT scan (Fig. 2) was taken 3 months after full resolution of the symptoms as the athlete developed a one week history of similar pleuritic chest pain on exertion. The scan showed residual thickening of the lower part of the left oblique fissure and focal thickening of the left diaphragmatic pleura. The pain was attributed to an increased stretching of scarred lung tissues and this resolved over time.
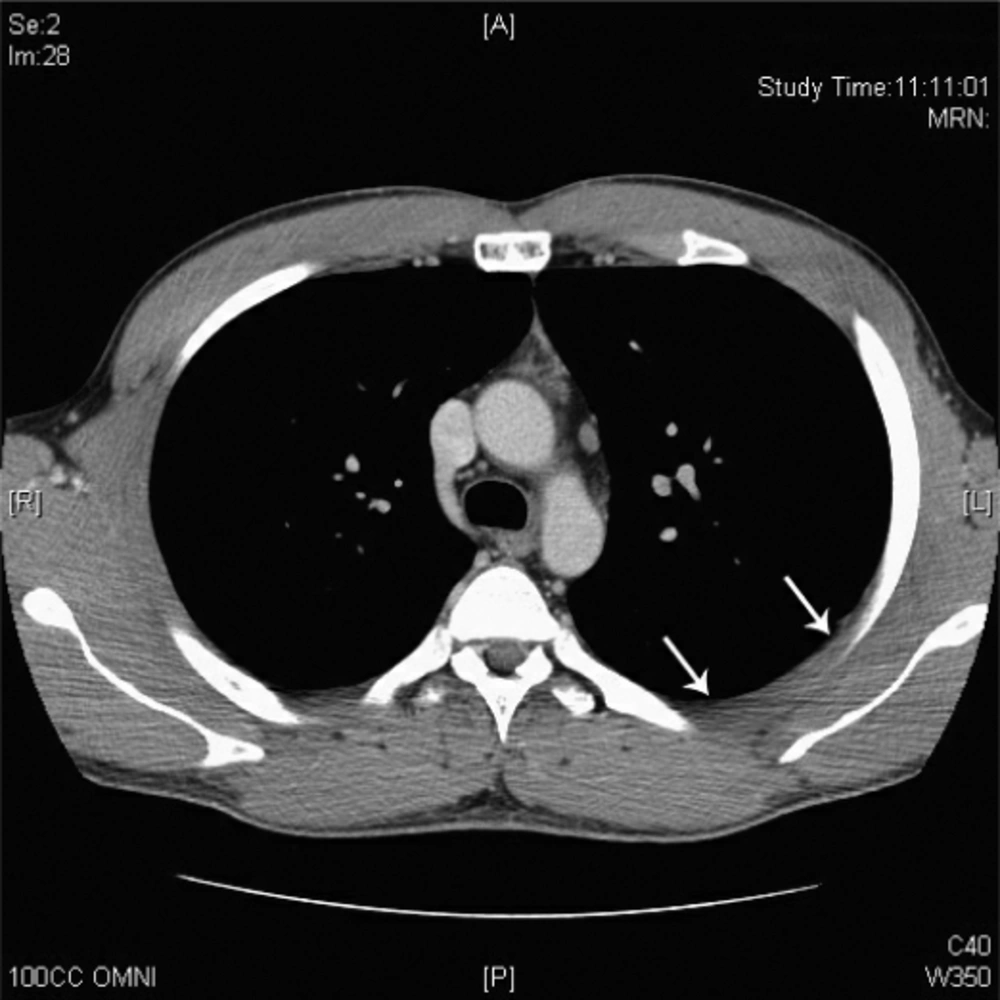
Fig. 2
CT scan of the thorax showing thickened pleura (arrows)
He has since this episode completed a further three ironman races with no similar episodes or adverse effects.
DISCUSSION
It has been postulated that there exists a J-shaped correlation curve between exercise load and risk of an upper respiratory tract infection[4, 5] possibly related to a transient immunity deficit at high training loads[1]. Following periods of intense training there might be a postulated ‘open window’ to infection because of diminished immune function of athletes 3-12 hours after exertion[4, 5]. Both the innate (natural killer cells and neutrophil activity) and adaptive (T cell and B cell function) immune system exhibit suppressed function. Recently Malm[6] proposed that rather than J-shaped the relationship could be S–shaped, with elite athletes being less prone to infections. Gleeson also proposes that a combination of factors is often present among elite athletes. Indeed, physiologic and psychological stress and disrupted sleep patterns may compromise their resistance to infection [2].
This particular case clearly shows the importance of a heightened clinical awareness by physicians when treating endurance athletes. These individuals regularly push their bodies to extremes and often delay seeking medical advice with symptoms that could belie theseriousness of an underlying condition. In this instance, the athlete managed to successfully complete two thirds of the Ironman race before his performance succumbed to the clinical conditions.
The literature reports a number of fatal bacterial pneumonia cases that were closely associated with exercise[7]. What is salient is that the athletes’ symptoms ranged from being totally asymptomatic up to full blown sepsis. Hence, return to play is another hot issue since currently there are limited guidelines post pneumonia. Early return can lead to complications including spontaneous pneumothorax, bronchiectasis, haemoptsis, acute respiratory failure[8] and the potentially fatal myocarditis[9]. Although deconditioning takes 4-5 days[8], return to full training had to be even slower in this particular case due to the combined excessive strain the triathlete underwent by running an ironman with pneumonia. Primos[10] states that if the athlete's symptoms are localised above the neck, such as headache and sneezing, the athlete can be allowed to play. Conversely, if the symptoms are below the neck, rest is advised. During acute infection, strenuous exercise should be avoided due to a systemic acute phase response to the infection and fever. The body will mobilise nutrients in response to the increased needs of the immune system, which can result in impaired muscle and aerobic performance. This further strengthens the argument that athletes should not exercise when they are febrile[10].
A number of nutritional supplements, such as magnesium[11], cystine, theanine (precursor of glutamate)[12] or glutamine[13] have been studied to see whether they can restore the impaired immune function after training. However, further research is needed in this field.
In this particular case the clinician chose the side of caution and closely monitored the athlete's training to minimise the possibility of relapse or complications. After all the athlete had to recover not only from the tough physical exertion associated with racing an Ironman, but also from his pneumonia. However, an athlete's crammed competitive programme does not always permit this. In such situations the sports medicine specialist must consult with the athlete and coaches concerned to ensure a safe return to competitive sport.
CONCLUSION
An athlete developing upper respiratory tract symptoms that are not resolved merits a chest X-ray to exclude pneumonia. Inadequate rest and recovery from minor illnesses predisposes the athlete to severe infections due to an impaired immune function. This athlete had a relapsing pattern of pneumonia which may have been potentially prevented had the athlete decreased training intensity and/or rested completely at the initial stages of the illness. As the literature does not offer similar cases of relapsing pneumonia in endurance athletes, it is hard to provide recommendations about their management and return to sport.
