1. Context
Human papillomavirus (HPV) is a sexually transmissible virus renowned for its association with the development of cancer. Currently, there is no treatment available for HPV infection. In most cases, the infection is cleared by the body in around 1 - 2 years. However, sometimes HPV can persist and contribute to the development of pre-cancerous cervical intraepithelial neoplasia (CIN), which can progress into cervical cancer if left untreated.
Over 200 types of HPV exist, some of which are oncogenic or high-risk for cancer development. Approximately 70% of cervical cancers are caused by two HR-HPV types, HPV16 and HPV18 (1).
The cervix, one of the most susceptible mucosal sites to HPV, acts as an anatomical and immunological gatekeeper preventing the ascent of microorganisms from the vagina into the uterus. However, cervical viral infections during pregnancy increase the risk of ascending vaginal bacterial infections by compromising the protection offered by the cervical epithelium (2). Given the crucial protective roles of the cervix in the maintenance of pregnancy, it is likely that HPV infection increases the risk of intrauterine infections, which may lead to adverse pregnancy outcomes, including preterm labor (3).
Preterm labor, the etiology of which usually cannot be determined, remains one of the leading causes of perinatal mortality and lifelong morbidity worldwide (4). To date, a succession of studies has been published to divulge the association of viral and bacterial infections with adverse pregnancy outcomes. As the most common sexually-transmitted infection, the prevalence of HPV in pregnant women and its adverse consequences on pregnancy outcomes have gained increasing attention over the last years. However, the results of the available literature are inconsistent. In this context, the current mini-review aims to summarize the existing research evaluating the impact of HPV on preterm delivery.
2. Human Papillomavirus Infection
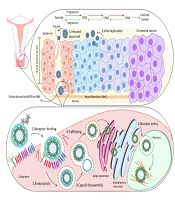
Human papillomavirus is a small, double-stranded, non-enveloped DNA virus with a genome of approximately 8000 base pairs in length. Its genome composes two late open reading frame (ORF) molecules called: L1 and L2. This virus has the ability to hijack the host’s replication and transcription machinery to produce virions that infect other cells (5).
The viral DNA may persist in the host cell without integration through aberrant episomal replication. The DNA transcripts of HPV are more likely to integrate near or within fragile sites of human DNA, where the strand is prone to breakage. There are five major HPV genera: alpha, beta, gamma, mu, and nu. Papillomaviruses present genotype-specific tropism for epithelial cells, causing skin (cutaneotropic) and mucous membrane (mucosotropic) infections. While the majority of cutaneous HPVs belong to the beta genus, the most important mucosal HPVs are a member of the alpha genus (6).
It is believed that cutaneous HPVs target hair follicle stem cells, where the virus can persist for long periods of time. They typically lead to the development of benign skin lesions, including cutaneous papillomas or warts. However, they may also be involved in the development of cutaneous squamous cell carcinoma (cSCC), especially in immunocompromised individuals (7).
Mucosal HPV infection occurs soon after the first sexual intercourse in early adulthood (8). Even though most women acquire a genital HPV infection shortly after becoming sexually active, most (> 90%) HPV infections will be cleared by the host’s immune system within 1 - 2 years. However, a minority of HPV infections persist beyond 12 months, increasing the risk of cervical and vaginal carcinogenic progression and the development of malignancies (9).
While there is no treatment for HPV, vaccines seem to be highly efficacious in preventing persistent infections and the formation of pre-cancerous lesions. However, these vaccines do not clear already established infections.
3. Human Papillomavirus as a Risk Factor for Preterm Birth
Generally, the risk and severity of certain infections are increased during pregnancy. A combination of physiological and immunological changes during pregnancy is suggested to play pivotal roles in increasing susceptibility to infections. Also, the relationship between infections and adverse pregnancy outcomes, as well as severe neonatal sequelae, has repeatedly been reported in studies (10).
On this point, there is controversy regarding HPV prevalence in pregnant women compared to non-pregnant women. While various studies suggested a higher prevalence of HPV infection in pregnant women compared to age-matched non-pregnant women (11-15), some have claimed that there is no statistical difference between these groups (16, 17).
The results of a meta-analysis showed a significantly increased risk of HPV infection in pregnant women, especially for those aged < 25 years (13). It has also been suggested that during pregnancy, changes in the hormonal milieu and immune responses render the eradication of the virus more difficult due to the decreased number of maternal natural killer and helper T cells. Besides, increased levels of steroid hormones during pregnancy are thought to enhance HPV replication by interacting with hormone-response elements in the viral genome. This gives another possible mechanism for the higher incidence of HPV infection during pregnancy (18, 19).
Generally, inflammation and infection are linked with a number of pregnancy complications, including preterm birth (20). Microbial infections in the amniotic cavity and fetus may originate from the bacteria ascending through the vagina or cervix or may be caused by the retrograde spread through the fallopian tubes, hematogenous distribution via the placenta, or as a sequela of invasive medical procedures (21).
While the association between some bacterial infections and preterm birth has long been established, evidence is beginning to confirm the involvement of viral infections in preterm birth. Considering that HPV is the most prevalent sexually-transmitted infection, which can affect both female and male reproductive systems, it is of paramount importance to evaluate the clinical impact of HPV infection on pregnancy and obstetrical outcomes.
A growing number of studies have highlighted the association between HPV infection and various adverse pregnancy outcomes, including preterm labor (22), spontaneous abortion (23), the premature rupture of foetal membranes (24), gestational hypertension (25), intrauterine growth restriction (26), low birth weight (27), and perinatal mortality.
Preterm delivery, which is defined as childbirth prior to week 37th and after week 20th of pregnancy, is a major cause of perinatal and neonatal mortality and accounts for a major proportion of long-term adverse health consequences for the mother and the newborn.
Notwithstanding, despite advancements in obstetric and neonatal care, the incidence of preterm birth has continued to rise in the last two decades, most of which being moderate to late preterm (34th to 36th weeks of gestation) (28). Many factors have been implicated, including the improved survival rate of very premature babies, the use of assisted reproductive techniques (with the resultant increased risk of multiple pregnancies), advanced maternal age, and a rise in maternal obesity.
While the exact underlying mechanism(s) of preterm delivery is not yet completely elucidated, multiple factors have been suggested to contribute to its rising incidence. Intrauterine infection/inflammation, uteroplacental ischemia/hemorrhage, maternal immunological intolerance, abnormal placental implantation, incompetent cervix, maternal stress, hormonal disorders, gestational diabetes, fetal distress, and fetal anomalies are among the factors proposed to be the major contributors to preterm delivery (29, 30).
In recent years, different groups of investigators have suggested that HPV infection (especially those caused by HR-HPVs) is associated with an increased risk of preterm birth (22, 31-33). For instance, in a retrospective cohort study on 2153 women, Caballero et al. announced HPV infection as a risk factor for preterm delivery resulting from the premature rupture of membranes (PROM) (33). Moreover, the results of a recent cohort study on 899 pregnant women indicated that persistent HR-HPV infection was associated with a significant increase in the risk of preterm birth (32). Congruent results have also been obtained in a meta-analysis by Huang et al. showing that the risk of preterm delivery was twofold greater in HPV-positive pregnant women than in those who were HPV negative (34). Other studies have also reported similar associations (35, 36). For instance, in a recent retrospective population-based study by Wiik et al., the risk of preterm delivery was indicated to be significantly high among women with HPV infection and/or CIN, particularly in those receiving no previous treatment (37).
However, there are studies that challenge this association as well. For example, Ambühl et al. carried out a prospective case-control study on 271 placental tissues and found no association between placental HPV infection and the risk of spontaneous preterm birth (38). In line with this, in another retrospective cohort study on 2321 patients, Subramaniam et al. identified no link between maternal HPV infection and the risk of preterm delivery (39).
Nonetheless, given that the establishment of a link between HPV infection and preterm delivery can have far-reaching implications in prenatal care, acquiring credible scientific evidence regarding this association is of utmost importance.
4. Suggested Mechanisms for the Association Between Human Papillomavirus Infection and Preterm Labor
4.1. Human Papillomavirus Targets Placental Trophoblast Cells
In pregnant women, the reported prevalence of HPV infection ranges from 6% to 65%. Several researchers have detected the DNA of HPV in the amniotic fluid, umbilical cord, placenta, and fetal membranes (38). Placental HPV infection has been linked to placental abnormalities, spontaneous abortion, and preterm delivery (35). The placenta is necessary for the maintenance of immune responses at the maternal-fetal interface and serves as a relatively effective barrier to the spread of infections to the fetus in utero. Nevertheless, multiple studies indicate that pathogenic viruses can invade the outer layer of the placenta, as well as trophoblast cells. Placental trophoblast cells play multiple roles during gestation, including in embryonic implantation.
Several lines of evidence have suggested that trophoblasts are the main target cells during placental HPV infection. Preliminary studies on trophoblast cell lines have indicated that HPV can directly infect trophoblasts and remain fully active in these cells (40, 41). Besides, HPV infection has been reported to alter the normal morphology and physiologic function of trophoblasts, increasing the rate of apoptosis and reducing placental invasion into the uterine wall. Unsuccessful trophoblast invasion of the uterine leads to the failure of placentation and subsequent adverse obstetric outcomes, including preterm delivery. This evidence supports the potential role of HPV in spontaneous preterm delivery (35).
4.2. Human Papillomavirus Infection Alters Vaginal Microbiome
The alteration of the homeostasis of vaginal microbiota during pregnancy has been reported to be associated with many pregnancy complications, including the increased risk of miscarriage, preterm birth, and endometritis (42, 43). Furthermore, HPV infection in pregnant women has been indicated to be associated with a more complex and diverse vaginal microbiome (44). During pregnancy, Lactobacillus is the dominant component of vaginal microbiota; however, HPV infection can increase the richness and heterogeneity of vaginal microbiota, characterized by a decline in the share of Lactobacillus (45). The alteration of the vagina’s acidic environment by HPV infection seems to promote the growth of bacteria (46). On the other hand, both HPV infection and disturbed vaginal microbiome seem to coincide with the increased production of inflammatory cytokines, mucosal injury, and chronic inflammation (47). Proinflammatory cytokines can contribute to the onset of labor; thus, the induction of the host’s inflammatory responses by HPV infection, along with changes in the vaginal microbiota, can be potential mechanisms intensifying the risk of preterm birth in the setting of HPV infection. Besides, inflammatory mediators such as metalloproteases (MMP) that degrade collagen and destroy fetal membranes can also contribute to PROM. In support of this theory, there is evidence of the association between HPV infection and PROM (24, 33).
5. Human Papillomavirus Vaccination and Preterm Delivery
While the benefits of HPV vaccination in preventing cancer progression are well-established, studies on the impacts of vaccination on the reduction of HPV-related adverse pregnancy outcomes are in their infancy. In a recent study in Australia, it was indicated that an increase in HPV vaccination coverage coincided with a slight reduction in the rate of preterm births (48). In another newly-published randomized clinical trial (NCT00534638), the rate of preterm labor was reported to be lower among HPV-vaccinated women compared to non-vaccinated counterparts (49). These findings support the hypothesis that HPV vaccination can reduce the incidence of preterm birth, which can offer noticeable public health benefits.
6. Conclusions
The unique hormonal and immunological changes happening during pregnancy may promote the persistence of HPV infection. While an increasing number of studies have shown that HPV infection is closely associated with premature delivery, this hypothesis is yet to be verified. Given that HPV infection changes the balance of the vaginal microbiome and alters the function of invasive trophoblasts, such an association is highly probable. This emphasizes the importance of HPV screening and vaccination programs prior to pregnancy.