1. Background
Although humans are smart, adaptable and have the ability to learn over time, they are prone to errors (1). Working in a healthcare environment is multitask, and depends on an efficient communication between those involved in the healthcare system, and on the manner in which the system is being managed (2). With respect to the complexity and dynamic job duties, nursing is unique and high workload is one of the major complaints of the nurses (3). This could impose major risks on patient safety (4); and as a result, mortality, prolonged hospital stay and medical costs would sharply increase (5). Patient safety is one of the most important issues in the healthcare system worldwide (6). An error is defined as a deficit created in the process of care, which results in patients’ major injury, or the one that has the potential to create such damages (7). Errors are of the most frequent causes of death and preventable complications in hospitals (8). Although nurses do not work apart from the whole system, and are the last part of the chain of care (9), more than 40% of their working time is directly involved in the implementation of health instructions (10). Therefore, committing errors when they are performing their tasks is typical (11). Applying the wrong dosage of medication and failure to comply with doctor’s prescription are examples of common errors among nurses in the healthcare environments (12). Evidence indicates that the level of medical errors in spite of all corrective actions has remained high (13). Between 44 to 98 thousand patients in the United States die due to preventable medical errors, and around one million injuries caused by medical errors is recorded annually (14). According to a study in the UK, changing the shift, lack of access to patient information, lack of experience, high workload, illegible handwriting, incomplete knowledge and skills, computational errors and faults in computer data entry were among the main causes of errors (15). A study in Australia showed that about 17% of all the cases admitted to the hospital led to an unwanted complication, half of which were preventable (16). Medical errors affected 85,000 people in the UK annually, leading patients to stay two more days in health facilities (17, 18). In France, 10,000 deaths are associated with medical errors annually (19).
According to Bandura’s theory, different factors can be attributed to medical errors (4), some of which are as follows: Fatigue (20), quality of working life (21), age (22), educational level (23), adherence to safety criteria (24), experience (25), leadership and organization (26), organizational structure (27), the demographics of patients (28) and shift working (29). In addition, medical errors have been ranked high in developing countries (5). Due to the poor reporting systems as well as complicated legal requirements to create a database, no exact figures are available in developing countries. However, according to court records, number of errors is high (30). In Iran, a study revealed that 16.7% of the nurses committed medical errors, and the most common were omission of some prescribed medications and inappropriate application of medications (31). In another study, 64.5% of Iranian nurses confessed that they had medical errors (32). In another research, 46.8% of the nurses in the emergency room of a teaching hospital in Tehran had errors within a year; of them, 69% were observed to have had at least one error during their nursing career (33).
Undoubtedly, one of the ways to improve patient safety is to distinguish medical errors and their causes. Among the methods available to identify and assess error, systematic human error prediction and reduction technique (SHERPA) is one of the most common ones to survey error. SHERPA method has more advantages compared to other methods of identifying human error (34) and is recommended for handling errors in healthcare processes and systems (35). Although the use of SHERPA is common in the industrial sector (36-39), in Iran published studies on human errors in healthcare centers were limited to areas such as surgery process (34), the duties of nurses in the emergency department (35, 40), ICU (41), and the duty of physicians in the emergency department (42).
2. Objectives
The aim of this study was to assess the types and causes of errors among the nurses and offer practical solutions to manage the tasks of the nurses and reduce the incidence of medical errors in the women’s infectious diseases ward in a teaching hospital in Qom, using the SHERPA method.
3. Methods
This cross-sectional study was conducted to identify and manage human errors of the nurses in the women’s infectious diseases ward in 2015. Sixteen female nurses were working in three shifts and were involved in the following activities: Administering drugs, injections, dressing, getting an EKG, checking the body temperature, measuring blood pressure, checking pulse rate, measuring blood sugar levels, and dealing with open and infectious wounds. Patients’ information was entered into a comprehensive system at admission, and after they were transferred to the wards, their conditions were checked and recorded. In this study, SHERPA was used to evaluate errors (37). The method’s reliability and validity have previously been approved (17, 43, 44). This method was also applied in healthcare sections in Iran and proved useful in recognizing errors (35, 40, 42). SHERPA could be adapted to various ward settings, and researchers could use it for a range of different healthcare procedures (17). In this study, SHERPA involved nine steps (Table 1).
Table 1.
Steps of SHERPA Technique
| Step | Title | Description |
|---|---|---|
| One | Hierarchical task analysis | Task/sub-tasks analysis by interviews and observation |
| Two | Task classification | Dividing tasks based on the behavior taxonomya |
| Three | Human error identification | Using error code |
| Four | Consequence analysis | Examining the consequences of each error |
| Five | Recovery analysis | Which action is necessary to error prevention |
| Six | Ordinal probability analysis | The probability of the error is determined |
| Seven | Criticality analysis | The severity of damage caused by error is determined |
| Eight | Remedy analysis | Practical ways to control and prevent error |
| Nine | Tabulation | SHERPA’s worksheets |
aTypes of errors included action, checking, retrieval, communication and selection errors.
In this study, the research team referred to the ward at different times within a day to observe the nurses’ performances as well as the conditions of the patients. After conducting interviews and providing the necessary explanations about aims of the study, the research team members collected the data on the activities of the nurses. Then SHERPA’s worksheets were completed. Tasks were classified and other items of the including including the codes of the errors, error descriptions, consequences of the errors, recovery, level of risk and corrective actions were completed for specified tasks based on the worksheets. The risk level of the errors contained probability (frequent, probable, occasional, remote and improbable) and severity (catastrophic, critical, marginal and insignificant) (Table 2). The results were examined with the cooperation of a number of nurses of the ward. The analysis was performed after the final verification of the worksheets.
Table 2.
Risk Level Matrix for Application in the SHERPA Techniquea
| Risk | Catastrophic | Critical | Marginal | Insignificant |
|---|---|---|---|---|
| Frequent (A) | 1A | 2A | 3A | 4A |
| Probable (B) | 1B | 2B | 3B | 4B |
| Occasional (C) | 1C | 2C | 3C | 4C |
| Remote (D) | 1D | 2D | 3D | 4D |
| Improbable (E) | 1E | 2E | 3E | 4E |
aShading indicates the highest risk level.
4. Results
One hundred fifty-nine errors related to the studied tasks (89 cases) were identified in the infectious diseases ward. According to Table 3, the highest number of recorded errors was reported as action type, and the lowest number of errors, which occurred in the infectious diseases ward, was the selection type. The frequency of nursing errors in terms of risk level is demonstrated in Table 4.
Table 3.
Description of Tasks and Identified Errors Based on the Hierarchical Task Analysis (HTA)a
| Categories | ||||||
|---|---|---|---|---|---|---|
| Action | Checking | Retrieval | Communication | Selection | Total | |
| Errors | 118 (74.21) | 8 (5.03) | 7 (4.40) | 25 (15.72) | 1 (0.63) | 159 (100) |
| Tasks | 65 (73.04) | 4 (4.49) | 4 (4.49) | 15 (16.86) | 1 (1.12) | 89 (100) |
aValues are expressed as No. (%).
Table 4.
Description (N (%)) of Identified Errors based on the Risk Level
| Risk Criteria | |||||
|---|---|---|---|---|---|
| Risk Type | Low | Medium | High | ||
| Acceptablea | Acceptableb | Undesirablec | Unacceptabled | Total | |
| Action | 32 (27.12) | 41 (34.74) | 38 (32.2) | 7 (5.93) | 118 (100) |
| Checking | 3 (37.5) | 5 (62.5) | 0 | 0 | 8 (100) |
| Retrieval | 0 | 3 (42.86) | 4 (57.14) | 0 | 7 (100) |
| Communication | 2 (8) | 2 (8) | 19 (76) | 2 (8) | 25 (100) |
| Selection | 1 (100) | 0 | 0 | 0 | 1 (100) |
| Total | 38 (23.90) | 51 (32.08) | 61 (38.36) | 9 (5.66) | 159 (100) |
aError: Occurred, No Harm to the Patient.
bIncreased need for monitoring, no change in vital signs or transient change in vital signs, No harm to the patient.
cIncreased monitoring, change in vital signs – treatment needed, change in length of stay or effect on an investigational drug protocol.
dIncreased monitoring and treatment, change in patient morbidity or death.
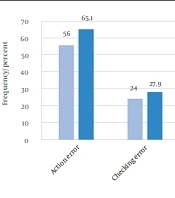
Based on the results (Table 4), 5.66% of the medical errors (9 errors) had an unacceptable risk level (high), 38.36% (61 errors) had undesirable risk level, 32.07% (50 errors) had an acceptable risk level, with a need for corrective acts (Medium), and 23.9% (38 errors) had acceptable risk level with no needs for corrective acts (Low). The highest number of errors was reported in those with undesirable risk level, and the lowest number was in those with unacceptable risk level. Among the unacceptable errors, action errors (77.78%) had the highest frequency, followed by communication errors with the rate of 22.22%. In addition, among the errors with undesirable risk level, action errors (62.29%) and communication errors (31.14%) were the most frequent. Moreover, errors with the greatest probability were identified based on SHERPA technique.
The most important errors were as follows: Forgetting to assess the patient’s breathing conditions at admission, with the risk level of 3A (unacceptable); errors in assessing the patient’s pulse, with the risk level of 3B (undesirable); improper closing of the cuffs in dresses, with the risk level of 4A (acceptable with a need to redesign); lack of ECG lubricant gel, with the risk level of 3B (undesirable); no masking, with the risk level of 2B (unacceptable), and no hand washing or disinfection, with the risk level of 3B (undesirable). Moreover, errors with greater severity were recorded, including no replacement of the catheter in standard intervals,with the risk level of 2D (undesirable); failure to register the patient’s condition in terms of previous surgeries and diseases, with the risk level of 2E (acceptable but needing a redesign of actions); no measurement of blood sugar in patients, with the risk level of 2D (undesirable); failure to register the patient’s chest pain when taking ECG, with the risk level 2C (undesirable); and and lack of timely suction with the risk level of 2D (undesirable). The number of credible errors in SHERPA and an example of the filled worksheet of SHERPA in the studied wards are displayed in Tables 5 and 6, respectively.
Table 5.
Number of Credible Errors in SHERPA
| Error Type | Error Code | Explanation | Error Number | Total |
|---|---|---|---|---|
| Action | A1 | Action too long/short | 4 | 118 |
| A2 | Action mistimed | 10 | ||
| A3 | Action in wrong direction | 2 | ||
| A4 | Action too little/too much | 8 | ||
| A5 | Misaligned | 22 | ||
| A6 | Right action on wrong object | 5 | ||
| A7 | Wrong action on right object | 7 | ||
| A8 | Action omitted | 43 | ||
| A9 | Action incomplete | 17 | ||
| A10 | Wrong action on wrong object | 0 | ||
| Checking | C1 | Checking omitted | 7 | 8 |
| C2 | Check incomplete | 1 | ||
| C3 | Right check on wrong object | 0 | ||
| C4 | Wrong check on right object | 0 | ||
| C5 | Check mistimed | 0 | ||
| C6 | Wrong check on wrong object | 0 | ||
| Retrieval | R1 | Information not obtained | 0 | 7 |
| R2 | Wrong information obtained | 7 | ||
| R3 | Information retrieval incomplete | 0 | ||
| Communication | I1 | Message not transmitted | 19 | 25 |
| I2 | Wrong message transmitted | 0 | ||
| I3 | Message transmission incomplete | 6 | ||
| Selection | S1 | Selection omitted | 0 | 1 |
| S2 | Wrong selection made | 1 |
Table 6.
An Example of SHERPA Technique’s Worksheet in the Studied Infectious Diseases Ward
| Task Step | Error Code | Description | Consequence | Recovery | Risk Level | Remedial Measure |
|---|---|---|---|---|---|---|
| 1.1.1 | A8 | Fail to start infusion | No drug given | 3B | Training | |
| 2.1.1 | C1 | Fail to check the volume of medication in syringe | Overdose | 2C | Training in administering injections | |
| 3.1.1 | R2 | Read drug name incorrectly | Selection of wrong drug for administration | 3.1.3 | 1B | Indicate the patient condition the drug is prescribed for |
| 3.1.2 | R2 | Read drug dose incorrectly | Administration of overdose or dose of no therapeutic value | 3.1.3 | 2B | Only use standard abbreviations or write words in full. Computerized order entry |
| 3.1.3 | C1,2 | Check omitted/ incomplete | Wrong drug and/ or wrong dose would be delivered | 2C |
5. Discussion
As demonstrated in Tables 3 and 5, action errors accounted for the highest frequency (74.21%), similar to findings of other researchers in the healthcare section (41, 42) and industries (36). Since most of the activities of the nurses in hospitals involve clinical procedures, lack of an appropriate implementation of guidelines and improper drug usage, or treatment communication with the registered patients may lead to the incidence of errors in the form of the action type (35). In this study, the lowest number of errors was identified in the selection type. Mohammadfam et al. also found similar results in a therapeutic process (34). The only reported error that represented the selection error type was the application of catheter with a wrong number. However, this selection error had acceptable risk level. Given that the nurses do not need to make as much decisions as the physicians, this condition was acceptable. Furthermore, Lane et al. designed a research, using the SHERPA technique to identify pharmaceutical management errors in a hospital (17). In their study, the most frequent errors were of the action type and the least frequent were of the selection type.
Based on the obtained data, it was revealed that action errors were in the first line of errors, which is in line with findings of the previous studies (17), followed by communication errors as the most frequent errors (Table 5). Furthermore, a study conducted (using the SHERPA technique) among nurses in an Iranian hospital revealed that action errors were the most frequent, followed by retrieval errors (35, 42, 45).
In this study, undesirable errors dominated all other types, similar to some other studies (35, 42). On the other hand, Kermani et al. reported errors that were acceptable but needed corrections as the most frequent errors (40). These types of errors were consistent with the types of nurses’ tasks in the infectious diseases ward. Communication errors usually occurred between the nurses and patients and between the nurses and patients’ families during the admission process. The nurses’ errors could be due to work overload or the lack of sufficient time to obtain valid and reliable information. The personnel of the infectious diseases ward encountered more workloads in their quest to maintain and support the epidemic of diseases (e.g., influenza), especially in certain seasons. It is anticipated that an increase in patients’ admission process and the high workload of the personnel generally increase errors, particularly action errors. To prevent this, it is recommended that more personnel be recruited based on a predefined plan.
According to Table 4, although action errors accounted for the highest frequency of errors, communication errors were of comparatively smaller percentage, as some of them were in the undesirable and unacceptable risk levels (38.13% vs. 84%). Therefore, it seems that communication errors, in addition to action errors, were important in infectious diseases wards and should be considered as a priority. Although many studies have signified the importance of teamwork in reducing action errors (36, 46), it should be noted that ambiguity increases communication errors in a team. In a study conducted on Swedish nurses, it was revealed that about 69% of the errors were related to teamwork (2). Nowadays, nursing is considered as a complex and dynamic job, which needs creativity and decision-making in undoubtedly difficult situations (47). In addition, contributing factors in the incidence of errors are multifactorial and related to people, teams and their organizations. In such circumstances, implementation of a root cause analysis (RCA) is recommended. Moreover, designing an effective analysis may help develop a proper system of record keeping and reporting as well as follow-up of the errors and internal investigation. For this purpose, the conceptual framework for error classification was suggested by WHO and the European Union (48).
In our study, which is similar to others (49), errors such as failure of recording vital signs and medications of the high risk patients were identified as common errors. Hence, addressing and redesigning this type of error as a high priority plan is recommended. It seems that high workload (50), long shifts (29) and quality of work (51) are the main factors that contributed to many errors in our study. Based on an extensive study in 617 hospitals, of which 488 were located in the United States and 12 in European countries, respectively, it was revealed that work organization of correlated with the quality of work environment in nursing (52). Another study on nurses in Belgium found that making improvements in nurses’ attitude increased their decision-making power, and created an honest environment based on common values as well as active participation of the head nurses, leading to performing the nursing tasks more accurately with the least number of errors (51). However, checking the status of patients and medical procedures can help control and improve conditions (53).
Reporting clinical errors is a crucial element in creating safer healthcare systems (46). Thus, improving error-reporting system is an essential step to improve patient safety (54). Researchers found that only 10% of medical errors are reported (55) and only 3.5% of the nurses believe that they should report all medical errors (56). A study on Iranian nurses showed that the number of errors that occurred was much more than what was reported (49). Ehsani et al. showed that 72.7% of the nurses did not report medical errors to their superiors (33). Their failure to report was due to the fear of fines or negative reaction of the patients (57). It seems that voluntary reporting of errors should be one of the common strategies. Creating computer based error reporting systems (42), job responsibility, organizational honesty, and learning from errors increase the number of reported errors (58). Moreover, equipment and tools can increase the human error rates considerably (59).
We are hopeful to detect and prevent the occurrence of errors and their great consequences. According to previous studies, 70% of the medical errors are preventable (42). The concept of integrated human factors and ergonomics (HFE) has been introduced as one of the key factors to help reduce medical errors (60). Based on the literature, controlling human error in medical environments is associated with human factors and ergonomics in the design and implementation of technologies, processes, workflows, jobs, teams and sociotechnical systems (61). Taking into account human factors and ergonomics increases the quality of healthcare services and patient safety (62). Application of information technology, organizational and work design (63), electronic records and health care/treatment data entry (64), social interactions, standard teamwork, and medical technologies are impressive cases in this challenging field (65).
5.1. Conclusions
In general, about 1.78 errors were detected for every studied task given in the infectious diseases ward. Considering the high level of errors, together with the sensitivity and the difficulty of patients’ status in infectious conditions, it is mandatory to implement medical error management systems. Based on the findings of this study, it is highly recommended to redesign treatment protocols and medical procedures based on principles of human factors and ergonomics (HFE) to enhance the quality of services, improve patient safety and reduce medical errors.