1. Background
Self-rated health (SRH), as a single-item self-assessment of health, is a commonly used subjective measure of health used in epidemiological researches (1, 2). These self-assessments have been used in many national surveys in the countries around the world. SRH has been shown to be associated with a number of important factors, including demographics (3, 4), geographical aspects (5), educational factors (6), economic factors (1), social correlates (2, 7), lifestyle behaviors (8), and some medical endpoints (9). Moreover, several studies have consistently demonstrated that SRH is a good predictor of mortality of various diseases (10, 11). Previous studies have also ascertained the validity and reliability of SRH (12, 13).
Women have poorer health compared to men in both developed and developing countries; 33.2% in Sweden (2), 24.3% in South Africa (14), 24.2% in South Korea (15), and 11.6% in Syria (16). Yet, these results may not be generalized to other populations due to different socioeconomic statuses and culture-specific perceptions of health. With regard to the socioeconomic status, a study concluded that to accurately estimate the “true” extent of inequalities in health, it is necessary that SRH measure health in a similar way across different socioeconomic levels (17). Moreover, individuals’ views regarding health are profoundly shaped by their cultural backgrounds (18, 19).
Up to now, few researches have been conducted on SRH among Iranian individuals (3, 6, 20-23). However, none of them has focused on the determinants of SRH in female population. One early study found a significant association between physical health, high-risk behaviors, and SRH among Iranian school students (21). Another study confirmed the association between SRH and economic status (3) and found the proportion of poor SRH to be 11.5% (3). In addition, among the individuals aged 15 years and over in Tehran, the capital of Iran, women reported poorer health compared to men (36% vs. 27%) (6). Two other studies also focused on the social factors related to SRH (24, 25).
The present study aimed to evaluate SRH and its related factors among women in the west of Iran.
2. Methods
This population-based, cross-sectional study was performed in the catchment area of 5 health centers in different districts of Sanandaj, western Iran, in 2012.
Based on the 11.5% proportion of poor SRH from an Iranian population (3) and considering significance level of 0.05 and error level of 0.012, a 977-subjects sample size was determined for the study. The samples were selected through cluster random sampling. Therefore, considering the design effect, the sample size was increased to 1200 subjects. To select a representative sample of women aged 18 years and over, stratified cluster random sampling method was employed considering districts (3 different districts) as strata and health centers as clusters (16 clusters). Then, all the women who came to the 5 selected health centers and consented to participate in the study were enrolled into the research. Before receiving the data from the participants, an informed verbal consent was obtained and anonymous questionnaires due to reassure the participants were distributed among them. The response rate was 87.5%.
Detailed description of the study variables have been published previously (26, 27) and only a brief summary has been reported here. The data were collected using an anonymous self-administered questionnaire by a single interviewer who was adequately trained. The questionnaire covered a wide range of socio-demographic characteristics, including age, education level, place of residence, marital, and pregnancy status, household’s income level, occupation status, quality of health services, use of health services, self-reported HIV testing, and SRH. The main outcome variable was SRH measured by a valid question (12, 13): “How do you rate your general health”. This question was responded through a Likert scale ranging from “very good” (coded as 1) to “very poor” (coded as 5). To analyze the data, the categories “very good”, “good”, and “fair” were combined (coded as 0) as were the categories “poor” and “very poor” (coded as 1) (28).
At first, each independent variable was entered separately into univariate logistic regression analysis. Then, the variables showing significance levels lower than 0.2 were entered into multiple logistic regression model. Bootstrapping with 1000 bootstrap samples was used to assess the relative robustness of the model. Lemeshow’s goodness-of-fit test was used to assess goodness of fit of the model. Simple coding was used to code the independent variables to compare each variable’s level to the reference level. Good SRH was used as the reference category. Furthermore, the results of evaluation of the associated factors with SRH were presented as odds ratios (OR) and 95% Confidence Intervals (95% CI) using STATA 11 statistical software (StataCorp, College Station, Texas).
3. Results
Overall, 37.68% (95% CI: 34.74, 40.61) of participants reported poor SRH and 62.32% (95% CI: 59.39, 65.26) reported good SRH. The proportion of descriptive characteristics among women is presented in Table 1.
Table 1
. Descriptive Characteristics of the Participants, West of Iran
| Variable | Frequency | Percentage |
|---|---|---|
| Age groups, y | ||
| 18 - 28 | 515 | 49.0 |
| 29 - 39 | 441 | 42.0 |
| + 40 | 95 | 9.0 |
| Educational level | ||
| Non-academic | 628 | 59.7 |
| Academic | 423 | 40.3 |
| Occupation | ||
| Housewife | 422 | 40.1 |
| Working | 629 | 59.9 |
| Marital status | ||
| Married | 639 | 60.8 |
| Single | 412 | 39.2 |
| Pregnancy status | ||
| No | 460 | 43.8 |
| Yes | 178 | 16.9 |
| No answer | 413 | 39.3 |
| Quality of health services | ||
| Bad | 268 | 25.5 |
| Reasonable | 455 | 43.3 |
| Good | 328 | 31.2 |
| Household’s income level | ||
| Bad | 344 | 32.7 |
| Reasonable | 450 | 42.8 |
| Good | 257 | 24.5 |
| Place of residence | ||
| Rural | 173 | 16.5 |
| Urban | 878 | 83.5 |
| Public health services utilization | ||
| No | 412 | 39.2 |
| Yes | 639 | 60.8 |
| Private health services utilization | ||
| No | 485 | 46.2 |
| Yes | 566 | 53.8 |
| Self-reported HIV testing | ||
| No | 680 | 64.7 |
| Yes | 337 | 32.1 |
| No answer | 34 | 3.2 |
The results of univariate and multiple logistic regression analyses have been presented in Table 2. Accordingly, older women were more likely than younger ones to describe their health as poor (OR = 1.44, 95% CI: 1.12, 1.86). Married women also had worse health status compared to those who had never been married. Additionally, higher household economic status was associated with 52% lower odds of poor SRH (OR = 0.48, 95% CI: 0.34 - 0.68). Besides, use of public and private health services were associated with 27% and 25% lower odds of poor SRH, respectively. Moreover, the women with self-reported HIV testing had 28% (OR = 0.72, 95% CI: 0.55, 0.95) lower chances of reporting poor SRH. Among the socio-demographic variables, low education level (OR = 1.32, 95% CI: 1.02, 1.71) was associated with poor SRH. However, after controlling other variables, the adjusted OR of SRH was not significant for education level.
Table 2.
Determinants of Poor Self-Rated Health Among Women According to Univariate and Multiple Logistic Regression Analyses
| Variables | Unadjusted | Adjusteda | ||
|---|---|---|---|---|
| OR (95% CI) | P Value | OR (95% CI) | P Value | |
| Age group, y | ||||
| ≤ 30 | 1 | 1 | ||
| ≥ 31 | 1.44 (1.12, 1.86) | 0.004 | 3.92 (2.59, 5.94) | 0.0001 |
| Education level | ||||
| Academic | 1 | 1 | ||
| Non-academic | 1.32 (1.02, 1.71) | 0.034 | 1.21 (0.91, 1.61) | 0.195 |
| Occupation | ||||
| Homemaker | 1 | 1 | ||
| Employee | 1.20 (0.93, 1.55) | 0.153 | 0.97 (0.71, 1.31) | 0.846 |
| Marital status | ||||
| Single | 1 | 1 | ||
| Married | 1.44 (1.11, 1.87) | 0.006 | 1.38 (1.04, 1.83) | 0.024 |
| Pregnancy | ||||
| No | 1 | 1 | ||
| Yes | 1.03 (0.72, 1.46) | 0.871 | ND | ND |
| No answer | 0.69 ( 0.53, 0.92) | 0.010 | ND | ND |
| Quality of health services | ||||
| Bad | 1 | 1 | ||
| Reasonable | 0.80 (0.59, 1.08) | 0.152 | 0.86 (0.62, 1.19) | 0.382 |
| Good | 0.61 (0.43, 0.85) | 0.004 | 0.62 (0.43, 0.88) | 0.007 |
| Household’s income level | ||||
| Bad | 1 | 1 | ||
| Reasonable | 0.63 (0.48, 0.84) | 0.002 | 0.21 (0.13, 0.33) | 0.0001 |
| Good | 0.48 (0.34, 0.68) | 0.0001 | 0.22 (0.14, 0.35) | 0.0001 |
| Place of residence | ||||
| Rural | 1 | 1 | ||
| Urban | 1.10 (0.79, 1.54) | 0.585 | ND | ND |
| Public health services utilization | ||||
| No | 1 | 1 | ||
| Yes | 0.73 (0.58, 0.97) | 0.029 | 0.63 (0.39, 1.02) | 0.060 |
| Private health services utilization | ||||
| No | 1 | 1 | ||
| Yes | 0.75 (0.59, 0.97) | 0.028 | 1.30 (0.81, 2.10) | 0.276 |
| Self-reported HIV testing | ||||
| No | 1 | 1 | ||
| Yes | 0.72 (0.55, 0.95) | 0.020 | 0.89 (0.64, 1.22) | 0.462 |
Abbreviations: CI, Confidence Interval; ND, No Data; OR, Odds Ratio.
aAdjusted for all other variables in the Table.
In multiple logistic regression analysis, SRH was associated with age, marital status, household’s income level, and quality of health services. Furthermore, the results of both crude and adjusted analyses revealed no statistically significant relationship between SRH and occupation status, pregnancy status, and place of residence.
4. Discussion
The present study assessed the effect of some factors on SRH in an Iranian female population. The study findings suggested that poor SRH was associated with age, marital status, household’s income level, education level, quality of health services, utilization of both public and private health services, and self-reported HIV testing. The main goal of this study was estimating the proportion of SRH in the study population, and the results indicated that 32.68% of the participants rated their heath as poor.
According to the literature, the proportion of poor SRH is the result of the processes that involve several factors. Education level is an important modulator of this phenomenon (3, 29). In bivariate analysis, the results of the present study demonstrated that the individuals with low levels of education had worse health status, which is in agreement with other studies (6, 15, 30). However, no significance relationship was found between SRH and education level after adjusting other factors. This finding indicates that SRH is related to other variables. Although the underlying reason is unknown, the effect of education can be varying from one place to another. For example, the effect of SRH on subsequent mortality risk differs by level of education. Several studies have found a stronger association in subjects with higher levels of education (31, 32), other studies have found stronger associations in those with lower education levels (33), and some have revealed no variations by education level (17, 34). Moreover, an international study, which aimed to determine the educational health inequalities in 22 European countries, indicated that the magnitude of educational health inequalities varied among the countries (35). Consequently, educational attainment can play an important role in occupation, economic status, lifestyle, and utilization of healthcare services.
The findings of our study showed that a higher proportion of older women reported poor health compared to the younger ones. This is in line with the previous studies performed in other developing countries (15, 16) as well as 2 studies conducted in Iran (3, 30). Asfar et al., investigated the determinants of SRH in adults and found that age was a significant predictor of poor SHR in both men and women (16). After controlling other variables, there was a relatively strong association between age and poor SHR (adjusted OR = 3.92, 95% CI: 2.59, 5.94). The results also showed that older age remained as an important predictor of poor SRH. Chen et al., also used multinomial logistic regression analysis in their study and disclosed that age was a predictor of SRH (36). In a study to describe SRH in middle-aged and elderly individuals, the authors reported that global SRH declined with age in both cross-sectional and longitudinal analyses (37).
In the current study, the individuals’ perception of quality of health services was found as one of the most important predictors of SRH. This finding is consistent with those of the previous studies showing that a good experience about primary care, including satisfaction with care, might be associated with SRH status (38, 39). Even after adjustment for socioeconomic and other factors, quality of health services was positively associated with good SRH status. Similarly, recent studies have demonstrated that good primary care experience was significantly associated with better health outcomes, even after controlling for income inequality and other socio-demographic correlates of health (40). Good accessibility of health facilities and the role of employers may be the main causes of satisfaction with health care (41). Expansion of the coverage of healthcare plans may be one of the possible explanations for this relation (42). Some studies have also presupposed the predictive power of SRH on the subsequent healthcare utilization (43, 44). Our results were consistent with those of the previous researches indicating that utilization of health services was associated with SRH. Pu et al., (45) reported that an individual’s medical care utilization was reflected in different domains of general health. Moreover, Mavaddat et al., (46) conducted a meta-analysis in order to estimate the strength of the association between SRH and fatal and non-fatal cardiovascular disease. Although health service utilization was not reported in any of the retrieved studies, they concluded that individuals with current poor SRH might warrant additional input from health services to identify and address reasons for their low subjective health.
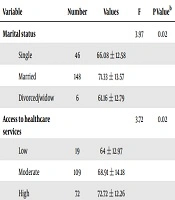
Our findings showed that being married was an important predictor of poor SRH. Married women were 44% more likely to report poor health compared to the single ones. Up to now, numerous epidemiological studies have investigated the correlation between marital status and SRH. However, inconsistent findings have been obtained. Some researchers believed that never married and divorced individuals had significantly higher ORs of poor SRH (2, 47). On the other hand, some other studies claimed that being married was the most important determinant of poor SRH (6, 16). Another study reported that married people tended to overestimate their health status (48). Accordingly, being married or not is an individual level indicator, however, its impact may depend upon cultural and socioeconomic statuses that vary at the social level. In addition, in a study conducted in Syria, the authors assumed that the difference between married and unmarried women might have its roots in gender roles and traditions of the Syrian society (16). Our finding is in line with another study, conducted in Iran, which showed that singleness was related to lower health-rated status (30).
In the present study, household’s income level was associated with SRH, such a way that the women who reported their income level as “good” had 52% lower odds of reporting poor SRH. Comparison of the significant variables in crude and adjusted analyses gave us points about SRH. The results of crude analysis revealed household’s income level as a probably associated variable. Interestingly, after adjusting the other variables, a strong significant relationship was found between SRH and household’s income level (crude OR = 0.48 vs. adjusted OR = 0.22). There may be several probabilities that help to account for the difference in reporting poor health. For instance, Molarius et al., (49) asserted that there was a disparity between women and men in terms of poor SRH. They reported that the OR of poor SRH related to good SRH was 1.29 (95% CI: 1.17, 1.42) for women compared to men. The authors also found no significant association between gender and SRH after controlling financial insecurity and condescending treatment. Another study using world health survey (WHS) data from Turkey with 10,287 respondents over 18 years old indicated that household’s income level was the greatest contributing factor to self-assessed health inequality (50). Similarly, Nedjat et al. (3) studied health inequality and its determinants among different socioeconomic groups in Tehran, the capital of Iran, and reported that several factors, including age, marital status, level of education, and household’s economic status were significantly associated with SRH in both crude and adjusted analyses. In that study, economic status was the main contributor to inequality in SRH (47.8%).
In our study, self-reported HIV testing, as a healthy behavior, was detected to be associated with SRH (OR = 0.72, 95% CI: 0.55, 0.95). We found only 1 similar study for comparison of the results. Tsai et al., (51) conducted a study in 2010 to investigate the association between the number of healthy behaviors and optimal SRH among U.S. adults. They found that healthy behaviors were associated with an increased likelihood of reporting optimal SRH among adults with cardiovascular diseases or diabetes.
The present study had several limitations. First of all, causality inference could not be determined due to the cross-sectional design of the study. Besides, the data were obtained through a self-report questionnaire and, therefore, recall bias was inevitable. The use of other self-report measures (household’s income level and self-reported HIV testing), as a benchmark for SRH, was also a major limitation of the study. Finally, in logistic regression analysis, SRH was categorized as “poor” (very poor/poor) and “good” (very good/good/fair). Thus, fair, very good, and good self-ratings of health were assumed to be the same, while in fact they are not.
4.1. Conclusion
The proportion of poor SRH varied depending on socioeconomic and socio-demographic determinants. Particularly as the main result, factors, such as advanced age, being married, household’s income level, and quality of health services were related to SRH. As SRH is an important predictor of death, individuals with the above-mentioned factors should be considered as the priority target populations.