



1. Background
The HBV prevalence in Europe ranges from 1 to 7% (1). Infection with this virus may lead to liver cirrhosis and hepatocellular carcinoma (HCC). In HBV-infected patients, there is an integration of changed viral DNA with human deoxycholic acid of the host that may stimulate both the development of primary neoplastic cells and the inhibition of apoptotic processes that favor this process.
As known, 90% of HCC cases are diagnosed in patients with HBV, HCV, liver cirrhosis, and fatty liver. The development of this tumor is associated with genetic and epigenetic predispositions, activation of cell oncogenes, and inactivation of tumor suppressor genes. Chronic HBV infection decreases the quality of life and constitutes a real life-threat.
The viral pre-S1 protein contains hepatocyte binding sites and plays a key role in the synthesis of HBsAg and subsequent virion assembly. HBsAg is synthesized in the endoplasmic reticulum and the Golgi apparatus. In the cytoplasm, it connects with the HBV genome and creates a complete viral particle. A decreased HBsAg synthesis leads to the intracellular inhibition of virus production.
2. Objectives
The study aimed to assess the frequency of HBsAg elimination among patients suffering from chronic HBV infection undergoing antiviral treatment with nucleoside or nucleotide analogs (NUCs). Possible predictive factors of this elimination were analyzed, such as the duration of HBV infection, sex, age, HBeAg status, initial viremia, and the type of antiviral therapy after which the HBsAg elimination occurred.
3. Methods
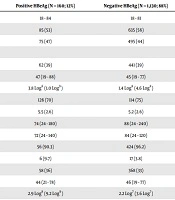
The study included 1,290 patients (720 women and 570 men) with a mean age of 60 (18 - 84 y/o) that were undergoing antiviral treatment due to chronic hepatitis B (Table 1). The patients were observed from 2014 to 2019.
| Profile | Positive HBeAg (N = 160; 12%) | Negative HBeAg (N = 1,130; 88%) |
|---|---|---|
| Age in years, average (range) | 18 - 84 | 18 - 81 |
| Women, % | 85 (53) | 635 (56) |
| Men, % | 75 (47) | 495 (44) |
| Last drug used | ||
| Entecavir, No. (%) | 62 (39) | 441 (39) |
| Age in years, average (range) | 47 (19 - 88) | 45 (19 - 77) |
| Viral load IU/mL, x (SD) | 3.8 Log8 (1.0 Log9) | 1.4 Log8 (4.6 Log8) |
| ALT IU/mL, x (SD) | 126 (70) | 114 (75) |
| AFP ng/mL, x (SD) | 5.5 (2.6) | 5.2 (2.6) |
| Average duration of infection, months (range) | 74 (24 - 180) | 88 (24 - 240) |
| Average duration of treatment, months (range) | 72 (24 - 140) | 84 (24 - 120) |
| Liver fibrosis from 1 - 3, No. (%)a | 56 (90.3) | 424 (96.2) |
| Cirrhosis, No. (%)a | 6 (9.7) | 17 (3.8) |
| Tenofovir, No. (%) | 58 (36) | 368 (33) |
| Age in years, average (range) | 44 (21 - 78) | 46 (19 - 77) |
| Viral load IU/mL, x (SD) | 2.9 Log8 (9.2 Log9) | 2.2 Log7 (3.6 Log7) |
| ALT IU/mL, x (SD) | 52 (38) | 58 (37) |
| AFP ng/mL, x (SD) | 6.6 (3.8) | 6.3 (7.3) |
| Average duration of infection, months (range) | 74 (24 - 140) | 69 (24 - 105) |
| Average duration of treatment, months (range) | 95 (44 - 130) | 85 (38 - 140) |
| Liver fibrosis from 1 - 3, No. (%)a | 49 (84.5) | 347 (94.3) |
| Cirrhosis, No. (%)a | 9 (15.5) | 21 (5.7) |
| Lamivudine, No. (%) | 28 (17) | 115 (10) |
| Age in years, average (range) | 46 (19 - 77) | 45 (18 - 77) |
| Viral load IU/mL, x (SD) | 2.9 Log8 (9.0 Log8) | 8.3 Log5 (5.7 Log4) |
| ALT IU/mL, x (SD) | 126 (71) | 115 (76) |
| AFP ng/mL, x (SD) | 5.6 (2.8) | 5.8 (5.6) |
| Average duration of infection, months (range) | 71 (24 - 180) | 85 (24 - 210) |
| Average duration of treatment, months (range) | 117 (42 - 227) | 127 (44 - 216) |
| Liver fibrosis from 1 - 3, No. (%)a | 26 (93) | 108 (94) |
| Cirrhosis, No. (%)a | 2 (7) | 7 (6) |
| Other, No. (%)b | 12 (8) | 206 (18) |
| Age in years, average (range) | 45 (20 - 80) | 45 (21 - 77) |
| Viral load IU/mL, x (SD) | 3.2 Log8 (8.9 Log8) | 3.9 Log7 (1.1 Log8) |
| ALT IU/mL, x (SD) | 97 (46) | 109 (45) |
| AFP ng/mL, x (SD) | 6.1 (2.3) | 5.6 (2.7) |
| Average duration of infection, months (range) | 78 (44 - 118) | 67 (42 - 115) |
| Average duration of treatment, months (range) | 108 (56 - 182) | 116 (24 - 180) |
| Liver fibrosis from 1 - 3, No. (%)a | 10 (83.3) | 194 (94.2) |
| Cirrhosis, No. (%)b | 2 (16.7) | 12 (5.8) |
aLiver biopsy or FibroScan (rating scale: Scheuer or METAVIR).
bInterrupted therapy, treatment with pegylated interferon alfa, LMV, ETV/TDV, and ADV.
Patients qualified for treatment were those chronically infected with HBV who had a minimum infection duration of six months (usually much longer). Patients eligible for treatment had HBeAg (+) minimum viral load of 20,000 IU/mL and anti-HBe (+) minimum viral load of 2,000 IU/mL. Liver biopsy or FibroScan was performed on treated patients to assess liver fibrosis. Based on the results, 90% of the patients showed slight fibrosis from 1 to 3 on a METAVIR or Scheuer scale. None of the patients had significantly elevated ALT levels (Table 1).
Before treatment, the patients were assessed for HBV viremia, HBsAg presence, HBeAg, ALT activity, AFP concentration, and the level of liver fibrosis. In all patients, the following was assessed every six months: HBV-DNA concentration, AFP, and the presence of HBsAg and HBeAg among patients with this antigen. In the case of HBeAg or HBsAg loss, the detectionof anti-HBe or anti-HBs was determined every three months.
Statistical analysis was performed using the chi-square test (χ2) and the Mann-Whitney U-test. The statistical significance level was set at P < 0.05.
All patients gave their constant to participate in the study and receive therapy. All patients (from all Research Centers) were qualified for the treatment and treated according to the recommendations of the National Health Fund (therapeutic program B18.1). All patients signed informed constant forms to use their laboratory results in scientific research.
4. Results
All patients, regardless of HBeAg presence in serum, had HBV viremia ≥ 4 log10 IU/mL. The permanent HBsAg loss within a 24-week observation period was confirmed in 39 (3%) individuals. The HBsAg loss occurred more often in men than in women (4.4% vs. 1.9%; P = 0.009). The HBsAg loss was found in eight (5.0%) patients that were HBeAg (+) and 31 (2.8%) patients that were HBeAg (-). However, the difference was not statistically significant (Table 1).
The mean age of the patients who had eliminated HBsAg was 60 (28 - 82 y/o). Only were four patients younger than 45 y/o. The age of the patients who had eliminated HBsAg was greater than the age of other patients (60 vs. 51 y/o); however, no statistically significant difference was confirmed.
The elimination of HBsAg was much more frequent among patients with cirrhosis of the liver than in all patients (13/39 (33.3%) vs. 77/1290 (5.9%), chi-square test (χ2) = 44.8, P < 0.0001).
Among all HBeAg (+) patients, an initial antiviral PEG-IFN therapy was commenced in 46 (29%) individuals, whereas it was the case of 396 (35%) patients in the group without HBeAg. In both groups, the treatment continued for 12 months. There was no influence of PEG-IFN on the HBsAg elimination right after the treatment and in the subsequent years.
In the group of patients with HBsAg elimination, the mean HBV viremia of HBeAg (-) individuals amounted to 7 log10 IU/mL, while in the group of HBeAg (+) patients, it was 8 log10 IU/mL. All patients from the latter group had viremia exceeding 7 log10 IU/mL (Table 2).
| Treatment Regimen | All Patients | HBsAg Elimination, No. (%) | HBeAg (-) | HBeAg (+) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Initial Viral Load, x (SD) | Duration of Treatment Until HBsAg Elimination, mo | Number of Patients Being Treated | HBsAg Elimination | Initial viral load, x (SD) | Duration of Treatment Until HBsAg Elimination, mo | Number of Patients Being Treated | HBsAg Elimination | |||
| Total | 1,290 | 39 (3.0) | 3.8 Log7 IU/mL (9.1 Log7 IU/mL) | 41 | 1,130 | 31 (2.8) | 9.2 Log7 IU/mL (1.4 Log8 IU/mL) | 38 | 160 | 8 (5) |
| Only ETV | 94 | 7 (7.4) | 1.3 Log8 IU/mL (2.2 Log8 IU/mL) | 48 | 73 | 3 (4.1) | 1.8 Log8 IU/mL (1.9 Log8 IU/mL) | 50 | 21 | 4 (19.0) |
| Sequential therapy LMV followed by ETV | 409 | 6 (6.4) | 3.1 Log7 IU/mL (5.3 Log7 IU/mL) | 76 | 368 | 12 (3.2) a2 (17) | 3.9 Log7 IU/mL (4.9 Log7 IU/mL) | 54 | 41 | 3 (7.3) a3 (100) |
| Only ETV and LMV/ATV | 503 | 22 (4.4) | 6.8 Log7 IU/mL (1.1 Log8 IU/mL) | 62 | 441 | 15 (3.4)b | 8.5 Log7 IU/mL (1.5 Log8 IU/mL) | 52 | 62 | 7 (11.3)b |
| Only TDF | 115 | 5 (4.3) | 1.0 Log6 IU/mL (1.9 Log6 IU/mL) | 47 | 88 | 5 (5.7) a3 (60) | - | - | 27 | 0 |
| Sequential therapy LMV followed by TDF | 311 | 6 (1.9) | 1.3 Log7 IU/mL (1.9 Log7 IU/mL) | 40 | 280 | 5 (1.8) a4 (80) | 2.2 Log6 IU/mL | 24 | 31 | 1 |
| Only TDF and LMV/TDF | 426 | 11 (2.6) | 6.9 Log6 IU/mL (1.4 Log6 IU/mL) | 43 | 368 | 10 (2.7) | 2.2 Log6 IU/mL | 24 | 58 | 1 (1.7) |
| Only LMV | 143 | 4 (2.8) | 1.4 Log8 IU/mL (4.6 Log8 IU/mL) | 105 | 115 | 4 (3.5) a2 (50) | 3.8 Log8 IU/mL (1.1 Log8 IU/mL) | - | 28 | 0 |
| Other treatmentc | 218 | 2 (0.91) | 8.3 Log5 IU/mL (5.7 Log4 IU/mL) | 18 | 206 | 2 (0.97) | - | - | 12 | 0 |
aPatients with liver cirrhosis; No. (%).
bChi-square 8.09, P = 0.004.
cPEG-IFN, Lamivudini, Entecavir/Tenofovir, Adefovir. One patient (HBsAg (-)) treated with ADV; initial viral load 4.2 Log5 IU/mL: elimination of HBsAg after 12 months of therapy. One patient (HBsAg (-)) treated with ETV/TDF; initial viral load 1.2 Log6 IU/mL: HBsAg elimination after 24 months of therapy.
The average infection duration among HBeAg (+) patients was 8.3 years (from 1 to 30 years), while among HBeAg (-) patients, it was 13.7 years (from 2 to 31 years). No relationship was confirmed between the infection duration and HBsAg elimination.
Of 39 patients with HBsAg elimination, 16 were treated with only one antiviral drug, 22 were treated initially with LMV and then with ETV or TDF, and one patient was initially on PEG-IFN and then on TDF. In this patient group, the most popular drug was ETV or TDF. Although HBsAg elimination occurred more often after ETV treatment, the difference concerning patients treated with TDF was not statistically significant (Table 2).
In 38% (3/8) of HBeAg (+) patients and 42% (13/31) of HBeAg (-) patients, there occurred conversion into anti-HBs within three months after HBsAg elimination at the earliest. No statistically significant difference was confirmed in the frequency of these antibodies depending on the HBeAg status (Table 2).
In patients treated with ETV, HBsAg was significantly more often eliminated in HBeAg (+) patients (Table 2). In five out of 39 (13%) patients in whom HBsAg was eliminated during the observation period, a liver transplant was performed due to liver failure secondary to liver cirrhosis (Table 2).
5. Discussion
The efficacy of various antiviral therapies varies among CHB patients, indicating that both viral and host factors can affect the results. Stelma et al. (2) treated 98 patients with CHB for 48 weeks with PEG-IFN and ADV. Five years after the treatment came to an end, the HBsAg elimination was confirmed in 19% of the patients with HBeAg and 16% of the patients without this antigen (2). Already in this study, similar to the authors’ study, a more frequent HBsAg elimination was observed in HBeAg (+) patients.
Aziz et al. (3) assessed 110 patients with CHB that were treated with TDF for 48 months and did not confirm the HBsAg elimination in a single one of them. On the other hand, Alawad et al. (4) observed HBsAg clearance within a five-year treatment period or five years after the treatment stopped in 34% of patients treated with PEG-IFN and 37% of patients treated with NAs. The observation indicated high NA efficacy. Usually, the therapy efficacy is worse with the use of these drugs than with PEG-IFN.
Inoue et al. (5) analyzed the frequency of HBsAg elimination among CHB-patients depending on the HBV genotype. During a 10-year long antiviral therapy, the HBsAg elimination was confirmed in 3.6% of patients with B genotype and 0.7% of patients infected with C genotype. It was not confirmed that any of the antiviral drugs (LMV, ETV, TDF, and ADV) led to higher efficacy of HBsAg elimination (5). In Poland, the most common HBV genotypes are A (67%) and D (20%) (6). In the authors’ study, the HBsAg elimination was confirmed more often among HBeAg (+) patients (5%) than in HBeAg (-) patients (2.8%), but it was not significantly different. Having analyzed all patients, in some of them, the PEG-IFN treatment preceded NAs therapy; however, it did not result in a more common HBsAg elimination. Only one patient among those who lost HBsAg was administered PEG-IFN before NAs.
Yan et al. (7) achieved a considerable decrease in or loss of HBsAg in patients with chronic HBV infections without HBeAg who were administered PEG-IFN for 48 weeks. However, a vast majority of patients treated with PGE-IFN had initial viremia ≤ 1000 IU/mL (7). Both PEG-IFN and NAs therapies rarely cause HBsAg elimination among patients suffering from chronic HBV infections (8). Numerous adverse reactions of PGE-IFN are the reasons behind the ever-increasing omission of this drug in the treatment of patients with chronic HBV infections.
A question about predictive factors for HBsAg elimination is more and more often raised, especially in the case of NAs treatment. In the authors’ study, patients with viremia ≤ 2,000 IU/mL were not qualified for treatment due to the criteria specified in domestic guidelines and drug program (9). In the authors’ study, patients treated with PEG-IFN usually had high viremia, which could explain the lack of efficacy of PEG-IFN therapy.
The mechanism of NAs antiviral effect is associated with their suppressive activity towards the synthesis of the virus’s DNA. However, in vitro studies have shown that ETV inhibits the priming of DNA-HBV polymerase, which presents an additional mechanism for the antiviral effects of this drug (10). Perhaps it is significant concerning a slightly more frequent HBsAg elimination during the ETV therapy observed in the authors’ study. A significantly more frequent HBsAg elimination in HBeAg (+) patients than in HBeAg (-) patients treated with ETV is interesting.
5.1. Conclusions
The HBsAg elimination in patients undergoing antiviral treatment is more common in men, patients with detectable HBeAg antigen, and individuals above 60 y/o. The liver cirrhosis was often diagnosed in patients who had HBsAg elimination. It appears that ETV is the best choice for patients with detectable HBeAg.
