1. Background
Organ transplantation is routinely performed to replace disabled organs, improving patients’ survival and longevity. However, this operation is accompanied by complications, such as a weakened immune system due to consumption of immunosuppressive agents (1). Under such conditions, microorganisms that are naturally colonized in healthy individuals, without harming the host, can become invasive and cause a wide range of problems, from local to fatal systemic diseases (2). Fungal infections, particularly candidiasis, are the major cause of mortality in transplant recipients (3).
The oral cavity in 20% of healthy adults contains various strains of colonized and non-pathogenic Candida spp. (4). This level reaches 31% in kidney transplant recipients and 44% in liver transplant patients (LTPs) (5). In a study on kidney transplant patients, hemodialysis patients, and healthy volunteers, Ahmadieh et al. found that the amount of Candida within the oral cavity of the first two groups was significantly higher than in the third (6). Such patients are likely to develop an invasive fungal infection (IFI), the prevalence of which among LTPs is 4% - 42%, with a mortality rate of 25% - 69%, according to studies by Patel et al. and Mora et al. (7, 8). Badiee et al. reported the prevalence at 19%, with a 100% mortality rate (9). Based on a study carried out by Lumbreras et al. these rates were as high as 50% and 100%, respectively (10).
Controlling and preventing fungal colonizations in different parts of the body, including the oral cavity, in LTPs can decrease the risk of developing post-transplant IFI (5). It also has positive economic effects by reducing the duration of hospitalization (11). Prevention can be achieved with the use of antifungal mouthwashes. Traboulsi et al. compared the antifungal effects of gentian violet, tea tree oil, and chlorhexidine on oral candidiasis, and observed that gentian violet was the most effective (12). Ramage et al. revealed that compared to azoles, the mouthwashes available on the market have a greater impact on Candida biofilms (13) Similarly, other studies have evaluated the effects of different mouthwashes on Candida strains in vulnerable patients by determining the minimum inhibitory concentration or minimum lethal concentration (14, 15). The recipients of solid organ transplants experience immune system weakening because of the transplant drugs; hence, they must be checked for prevalent Candida strains in the oral cavity, and given effective mouthwashes.
2. Objectives
This study aimed to determine the prevalence of fungal strains of Candida within the oral cavity of LTPs at a hospital in Shiraz, the center for liver transplantation in Iran, and to evaluate the effects of chlorhexidine, Nanosil D1, Vi-One, Oral-B, and Nystatin mouthwashes at different exposure times on these colonizations.
3. Patients and Methods
This experimental study was carried out on 101 LTPs who were referred to Namazi hospital for their first monthly examination during the final six months of 2014. The study was approved by the ethics committee of Shiraz University of Medical Sciences, and a written informed consent form was signed by each patient. All patients had the same medication regimen for at least one month; none had received systemic or local antifungal drugs for one week prior to sampling. A sterile swab was rubbed across the palate, tongue, gums, and teeth, and was then transferred into Sabouraud dextrose agar (Merck, Germany). The culture medium contained chloramphenicol to inhibit the growth of normal oral microflora. The patient’s name and the date of sampling were recorded on each plate. Demographic data, including age, sex, type of transplant, and medication doses, were retrieved from the patients’ files, as well as through interviews, and recorded on special forms.
3.1. Culture and Identification of Isolated Strains
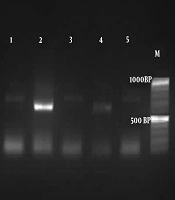
The plates were transferred to the laboratory to be stored at 24°C for one week, and then checked for fungal growth. The samples with fungal growth on culture were subcultured onto potato dextrose agar (Oxoid Ltd; Basingstoke, Hampshire, England). Once purity was ensured, suspensions of the isolated fungi and distilled water (105) were prepared in sterile tubes. Using a sonicator, the fungal walls were broken and DNA was released. The suspension was centrifuged at 3,000 RPM for 3 minutes, and the supernatant suspension containing DNA was used for the restriction fragment length polymorphism (RFLP) test. In this analysis, the yeast strains were identified by using ITS1 (5′-TCCGTA GGT GAA CCT GCG G-3′) and ITS4 (5′-TCC TCC GCT TAT TGA TAT GC-3′) primers and MspI enzyme (16).
3.2. Determining Mouthwash Susceptibility
The studied mouthwashes were 0.2% chlorhexidine (Donyaye Behesht pharmaceutical center, Iran), Vi-One (Rojin Ltd., Iran), Oral-B (Procter and Gamble technical center Ltd., UK), and Nanosil D1 (Kimia Fam pharmaceutical center, Iran), with Nystatin 100,000 IU/mL (Jaberebne Hayan pharmaceutical center, Iran) as the control. To determine the susceptibility of all isolated strains of Candida to the various mouthwashes, based on the CLSI M27-A2 standard method (17), a dilution equal to 0.5 McFarland was prepared of each single yeast with a spectrophotometer, at a 530 nm wavelength in normal saline. This dilution of fungi contained 106 yeasts/mL.
For each mouthwash, two sterile test tubes were prepared, containing 100 µL of yeast suspension and 100 µL of mouthwash. Based on the exposure durations suggested by the mouthwash manufacturers, the first tube was neutralized after 30 seconds and the second was neutralized after 60 seconds, continuing for 5 minutes by using 200 µL of European neutralizing solution (1% v/v phosphate buffer, 0.5% w/v sodium thiosulfate, 0.1% w/v L-histidine, 0.3% w/v lecithin, and 10% v/v Tween-80 [refined soybean oil]). Next, the yeasts were rinsed with PBS buffer. Three different cultures were established for each suspension. The mean colony count on each plate for the related mouthwash was calculated after the specified duration. The patients’ file data and the laboratory data were analyzed using SPSS version 16 (Chicago, IL, USA). Wilcoxon’s signed-rank test, the Kruskal-Wallis H test, and the Mann-Whitney U test were used as appropriate.
4. Results
Of the 101 LTPs in this study, 39 were female (38.6%) and 62 were male (61.4%), with an age range from 2.5 months to 63 years (mean ± SD 29.8 ± 18.3 years). Fungal growths were observed in the culture media of 68 cases (67.4%), the most frequent of which were C. albicans (50.5%) and C. glabrata (7.9%) (Table 1).
Table 1.
Candida Species Isolated From Oral Specimens of Liver Transplant Patients
| Candida Species | Valuesa |
|---|---|
| C. albicans | 51 (50.5) |
| C. glabrata | 8 (7.9) |
| C. kefyr | 4 (4) |
| C. parapsilosis | 2 (2) |
| C. tropicalis | 2 (2) |
| C. intermedia | 1 (1) |
| Negative and missing | 33 (32.6) |
| Total | 101 (100) |
aValues are expressed as No. (%).
The susceptibility tests of the Candida species isolated from each patient to the four mouthwashes revealed a significantly higher antifungal effect at the exposure time of 60 seconds compared to 30 seconds. The highest and lowest effects within 30 seconds were respectively related to chlorhexidine and Vi-One, while Oral-B and Nanosil D1 showed no significant difference. At the exposure time of 60 seconds, chlorhexidine was the most effective, followed by Oral-B, Nanosil, and Vi-One, respectively. Meanwhile, Nystatin mouthwash had a full cytotoxic effect at both exposure times (Table 2).
Table 2.
| Mouthwash | Time 1 (30 s) | Time 2 (60 s) | P Valuec |
|---|---|---|---|
| Nanosil | 50 (53.9 ± 36.4)A | 10 (28.7 ± 31.4)A | < 0.001 |
| Chlorhexidine | 10 (28.9 ± 33.6)B | 5 (9.7 ± 17.7)B | < 0.001 |
| Vi-One | 80 (67.8 ± 32.5)C | 30 (39.2 ± 34.2)C | < 0.001 |
| Oral-B | 40 (43.9 ± 36)A | 10 (17.6 ± 26.3)D | < 0.001 |
| P valued | < 0.001 | < 0.001 |
aIn each time point, different capital letters (A - D) in superscript show significant difference between groups using Mann-Whitney U test.
bValues are expressed as median (mean ± SD).
cUsing Wilcoxon Signed-Rank test.
dUsing Kruskal-Wallis H test.
5. Discussion
Candida colonization in the oral cavity differs among different populations, and may become a source of candidiasis for immunocompromised patients, including LTPs. Candida colonization has been reported in 46.8% of patients with hematological disorders (18), and in 19% - 50% of LTPs (7-10, 19). The present study found a colonization rate of 67.4% in LTPs. Since the prescription of antifungal agents prophylactically can cause resistant strains, suitable mouthwashes can be used to prevent invasive Candida infections. According to authoritative sources and the background of infectious diseases in LTPs, invasive Candida infections usually develop during the first two months after transplantation (20), due to improper hygiene management in patients, operating rooms, and intensive care units. As stated in the study by Badiee et al. Candida infections occur in one out of five patients (19%), with a mortality rate of 100% (9). This fact highlights the importance of preventing the oral colonization of Candida species. Using an appropriate mouthwash before and after transplantation significantly improves the patient’s hygiene and decreases the risk of developing disease. It also decreases the need for medications and reduces subsequent costs.
In this study, the most frequent fungal strain found in the cultured intraoral samples from LTPs was C. albicans, which is the most prevalent species causing oral candidiasis (21, 22). The second most frequent was C. glabrata, which generally appears opportunistically in patients with weakened immune systems. This was in line with a study performed by Jin et al. that reported similar strains in samples from 70 transplant patients (2). The findings of a study by Haddadi et al. indicated that C. krusei was the second most prevalent strain found among 188 patients with weakened immune systems due to hematological disorders. Furthermore, C. glabrata was in fourth place in that study and C. kefyr was in sixth place, which was the third most frequent strain in the present study (18).
Ramage et al. found that compared with azoles, the mouthwashes available on the market have a stronger effect on Candida biofilms (13). Similarly, in an in vitro study, Shrestha et al. demonstrated the antifungal effects of mouthwashes containing chlorhexidine and thymol, by determining the minimum inhibitory concentration and time-kill assays in Candida strains (15). Carvalhinho et al. investigated the antifungal effects of essential oils on Candida strains by using the disk diffusion method (14).
In a different study, Al-Mohaya et al. observed that using miswak sticks considerably reduced oral Candida colonizations in kidney transplant patients (23). The mouthwashes used the present study were chlorhexidine (0.2% chlorhexidine gluconate), Vi-One (0.05% sodium fluoride and 0.05% cetylpyridinium chloride), Oral-B (sodium fluoride, cetylpyridinium chloride, polysorbate 20, and some preservative agents), and Nanosil D1 (H2O2 and Ag+ nanoparticles), with 100,000 mL/IU of Nystatin as the control. All of these underwent time-kill assays to determine their antifungal susceptibility.
The present study demonstrated that the antifungal effects of all four of the mouthwashes were significantly higher at the exposure time of 60 seconds than at 30 seconds. Chlorhexidine and Vi-One, respectively, had the highest and lowest effects at 30 seconds; however, Oral-B and Nanosil showed no significant differences and were in the middle. At 60 seconds of exposure, chlorhexidine was the most effective, followed by Oral-B, Nanosil D1, and Vi-One, respectively. Nystatin, a renowned antifungal agent from the polyene family, demonstrated full cytotoxicity at both exposure times as the control mouthwash.
Mouthwashes carry out their effects through chemical and mechanical processes: the pressure of the circulating liquid in the mouth mechanically inhibits the colonization of fungi, while the active ingredients deactivate fungal organisms through chemical reactions. The chemical mode of action is the coagulation of proteins and nucleoproteins, destruction of the cell walls, and prevention of the germination and growth of fungi, in addition to detergent effects and increased solubility of organic materials (15). Thus, a longer exposure time increases the mechanical and chemical efficiency, and more fungi are consequently killed. In this study, chlorhexidine was the most effective at the exposure time of 60 seconds. Further research is suggested in order to evaluate longer exposure times, tolerance to using mouthwashes based on patients’ ages, and mouthwashes with other active ingredients, preferably herbal types. Also, mouthwash is recommended to be circulated on plates in order to simulate the rinsing motion.
Clearly, Candida colonization is a risk factor for IFI and candidemia, particularly in hospitalized patients. It is also known that the mortality rate of candidemia is almost 11% in children (24), which culminates in LTP (9). The oral cavity is the most common location for Candida colonization (25). Considering all of these factors, controlling and preventing fungal colonization in different parts of the body, including the oral cavity, in LTPs can decrease the likelihood of developing post-transplant IFIs (5). This will also help to decrease the costs of hospitalization (11).
This prevention can be done both through taking antifungal agents and by using mouthwashes that act against fungal colonization. However, special attention must be paid to the increasing drug-resistance of microorganisms; for example, Haddadi et al. (18) reported C. glabrata as the most resistant strain to azoles and amphotericin B, while it was second-place in the current study. Another concern to consider is the higher costs of drugs compared to mouthwashes. A simple calculation is enough to show that if a patient uses 0.2% chlorhexidine gluconate three times daily (5 mL each) to prevent fungal colonization during the first two critical months after transplantation, three 300-mL bottles will be required, for a total cost of 15.54 USD from the Amazon website (5.18 USD or 3.68 GBP per bottle) (26). On the other hand, daily pharmaceutical prophylaxis in the form of, at most, 400 mg/day of fluconazole or 2 mg/kg of liposomal amphotericin B for two weeks (27) will cost, respectively, 239 and 378 USD (28, 29); i.e., almost 20 times higher than the cost of preventing infection with mouthwash. In cases of IFI, hospital costs are estimated to be approximately 40,000 USD (27). All of this indicates that mouthwashes can considerably reduce therapeutic costs.
The results of the present study at Namazi hospital showed that the rate of fungal colonization in the oral cavities of LTPs was 67.4%, and C. albicans was the most frequent strain. Chlorhexidine, at an exposure time of ≥ 60 seconds, is suggested as an effective antifungal prophylaxis to be included in the medication regimen of such patients before and after transplantation, in order to prevent fungal colonization and subsequent systemic infection. In additional, fungal colonizations must be regularly checked for in these patients, so that appropriate decisions can be made in a timely manner in cases of resistant strains.