1. Background
2. Methods
2.1. Patients
2.2. Definition of TACE-Refractory and TACE-Ineligible
2.3. Procedure
2.4. Efficacy and Safety
2.5. Statistical Analysis and Ethical Considerations
3. Results
| Variable | Values |
|---|---|
| Age, years | 73 (50 - 85) |
| Sex, male/female | 21/7 |
| PS (ECOG), 0/1/2 | 8/18/2 |
| Stage, III/Iva | 19/9 |
| MVI, present/absent | 9/19 |
| MVI, Vp 2/3/4, Vv 2/3 | 1/4/4, 0/5 |
| Tumor distribution, unilobar/bilobar | 5/23 |
| C-P score, 8/9/10 | 17/6/5 |
| Bil, mg/dL | 1.4 (0.5-2.4) |
| ALB, g/dL | 3.0 (2.0-3.7) |
| PT, % | 63 (49-79) |
| Ascites, -/+/++ | 1/25/2 |
| Encephalopathy, present/absent (history +) | 0/28 (4) |
| Etiology, HBV/HCV/NBNC | 1/21/6 |
| WBC, /μL | 3950 (2100-11350) |
| Hb, g/dL | 11.6 (9.9-14.4) |
| PLT, × 104/μL | 8.0 (4.4-41.2) |
| CRE, mg/dL | 0.78 (0.47-1.33) |
| AFP, ng/mL | 62.9 (5.3-135623) |
| PIVKA-II, mAU/mL | 1110 (7-295000) |
| STATE score, <18/ ≧ 18 | 13/15 |
| Prior therapy, present/absent | 18/10 |
| TACE history, present/absent | 17/11 |
| Categorization, TACE-refractory/-ineligible | 10/18 |
Abbreviations: AFP, Alpha-Fetoprotein; ALB, Albumin; Bil, Bilirubin; C-P, Child-Pugh; HBV, CRE, Creatinine; Hepatitis B Virus; HCV, Hepatitis C Virus; Hb, Hemoglobin; MVI, Macroscopic Vascular Invasion; NBNC, Non-HBV and Non-HCV; PIVKA-II, Protein Induced by Vitamin K Absence or Antagonist-II; PLT, Platelet; PS (ECOG),Performance; PT, Prothrombin; Status (European Cooperative Oncology Group); STATE, Selection for TrAnsarterial chemoembolization TrEatment; TACE, Transcatheter Arterial Chemoembolization; Vp, Portal Vein; Vv, Hepatic Vein; WBC, White Blood Cell.
aValue are expressed as number presente or median (range), as appropriate.
| Reason for dose reduction | N |
|---|---|
| tumor spread; unilobar | 5 |
| PLT decrease | 7 |
| WBC decrease | 2 |
| CRE increase | 3 |
| Child–Pugh score | 4 |
| PS decreased | 2 |
Abbreviations: CRE, Creatinine; PLT, Platelet; PS, Performance Status; WBC, White Blood Cell.
aThe numerical data represent the number of cases.
bThere is some overlapping of cases between categories.
| Variable | All Cases (n = 28) | MVI | Dose Intensity, % | |||
|---|---|---|---|---|---|---|
| + (n = 9) | - (n = 19) | 100 (n = 10) | 70-80 (n = 12) | 50 (n = 6) | ||
| CR | 0 | 0 | 0 | 0 | 0 | 0 |
| PR | 3 | 0 | 3 | 0 | 3 | 0 |
| SD | 7 | 1 | 6 | 4 | 1 | 2 |
| PD | 15 | 6 | 9 | 5 | 7 | 3 |
| NE | 3 | 2 | 1 | 1 | 1 | 1 |
| RR, % | 10.7 | 0 | 15.8 | 0 | 25 | 0 |
| DCR, % | 35.7 | 11.1 | 47.4 | 40 | 33.3 | 33.3 |
Abbreviations: CR, Complete Response; DCR, Disease Control Rate; MVI, Macroscopic Vascular Invasion; NE, Not Evaluated; PD, progressive disease; PR, partial response; RR, Response Rate; SD, Stable Disease.
aThe numerical data represent the number of cases.
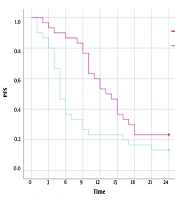
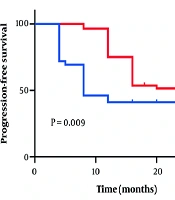
 and Progression-Free Survival (PFS)")
(A) OS of all cases, (B) PFS of all cases, (C) PFS and (D) OS for patients with/without macroscopic vascular invasion (MVI). (E, F) OS classified by treatment effect. (E) The partial response (PR) + stable disease (SD) group, showing significantly better survival than the progressive disease (PD) group. (F) SD vs. PD, showing significantly better survival of the SD group than the PD group.
| Variable | N |
|---|---|
| WBC decrease | 1 |
| Neutrophil count decreased | 1 |
| PLT count decreased | 4 |
| AST increase | 3 |
| ALT increase | 2 |
| ALP increase | 1 |
| Bil increase | 1 |
| Hepatic encephalopathy | 2 |
| Hemorrhagic gastric ulcer | 1 |
| BW increase ≥3 kg | 9 |
Abbreviations: AE, Adverse Event; ALP, Alkaline Phosphatase; ALT, Alanine Aminotransferase; AST, Aspartate Aminotransferase; Bil, Bilirubin; PLT, Platelet; WBC, White Blood Cell.
| Variable | Full Dose (n = 10) | Dose Down (n = 18) |
|---|---|---|
| Gr ≥ 3 AE+ | 6 | 5 |
| Gr ≥ 3 AE- | 4 | 13 |
| Full Dose (n = 10) | Dose Down (n = 18) | |
| BW increase < 3 kg | 5 | 15 |
| BW increase ≥ 3 kg | 5 | 3 |
Abbreviations:; BW, BodyWeight; Gr, Grade.
aThe numerical data represent the number of cases.