1. Context
Liver failure is a life-threatening disease characterized by the presentation of jaundice, hepatic encephalopathy (HE), ascites, and disturbed blood clotting mechanism, i.e., prothrombin time activity (PTA) below 40% (1). In Europe and the United States, drug and alcohol are the main causes of liver failure; however, the primary cause of liver failure is the hepatitis B virus (HBV) in China (2). HBV-related liver failure has been a severe clinical syndrome, causing high morbidity and mortality rates in China (3-5). Indeed, conventional approaches, as well as liver transplantation and artificial liver support devices with supportive medicine, cannot produce satisfactory outcomes (6). Although in certain cases, the interferon and nucleoside analogues prevent the progression of the disease to hepatic failure (7). Therefore, we need to explore the mechanism of HBV-related hepatic failure and find potentially more effective therapies to solve the problems.
Evidence shows that HBV mainly causes liver injury by the induction of cytotoxic T-lymphocyte-mediated cytolytic pathways in HBV infected hepatocytes (8, 9). The special effect of corticosteroids to inhibit immune responses and prevent cytolysis in infected hepatocytes is a reasonable strategy, supporting glucocorticoid plus conventional therapy (10, 11). Several studies suggested that corticosteroid combination therapy could reduce the mortality rate (12-18). However, some published reports have questioned the promising results of corticosteroids (19). The adverse effects of corticosteroids (infection, hyperglycemia, psychosis, peptic ulceration, and poor bone healing) and risk factors associated with HBV reactivation is well-documented (20-22).
The Chinese guidelines for the treatment of liver failure recommend that liver failure can be treated with glucocorticoids in autoimmune liver diseases induced liver failure, or at an early stage of liver failure caused by non-viral infectious etiologies when the disease develops rapidly without serious complications (1). On the other hand, the guidelines of the Asian-Pacific Association (2), the American Association (23) or the European Association (24) for the study of the liver have not recommended glucocorticoids plus conventional therapy. Accordingly, it seems reasonable to assume that the management of liver failure with glucocorticoids plus conventional therapy varies with geographic locations.
2. Objectives
We conducted this meta-analysis to evaluate the efficacy and safety of corticosteroids plus conventional therapy in Chinese patients with HBV-related liver failure and to outline the evidence for clinical decision-making.
3. Data Sources
3.1. Search Strategy
We searched several national and international databases, including PubMed, Embase, the Cochrane library, China National Knowledge Infrastructure, Wanfang database, and Google Scholar until April 2017. The search strategy was restricted to Chinese/English language papers. The electronic search strategy was generated using the following terms, “liver failure”, “Hepatitis B”, “glucocorticoid”, “hydrocortisone”, “dexamethasone”, “prednisone”, “prednisolone”, “methylprednisolone” (Appendix 1). Alternatively, references of the retrieved articles were searched manually.
4. Study Selection
The inclusion criteria in the selection of relevant studies were: (1) systematic reviews restricted to randomized controlled trials; (2) previously diagnosed patients (1, 25) with hepatitis B virus-related liver failure (ALF, SALF, ACLF, and CLF); (3) trails provided records of conventional treatment (supportive treatment, nucleoside analogue treatment, anti-infection treatment, proton pump inhibitors for the prevention of gastrointestinal bleeding, with/without artificial liver support); (4) trials involved in using glucocorticoids without contraindications; (5) reported data of efficacy and/or complications of primary therapy. The exclusion criteria were: (1) trials published as case reports, reviews, pharmacology, pharmacokinetics, and other non-clinical research or in abstract form without raw data; (2) patients with drug-induced hepatitis, autoimmune hepatitis, alcoholic liver disease or other causes of liver failure; (3) patients co-infected with other hepatitis viruses (hepatitis E, A, D, or C) and/or human immunodeficiency virus (HIV). Two investigators (Ran, Luo) independently evaluated the inclusion and exclusion criteria, and any discrepancies between them were resolved by consensus. The study protocol of this meta-analysis was registered (registration no-CRD42019122976) in the “International Prospective Register of Systematic Reviews”.
4.1. Primary and Secondary Outcomes
The primary outcome was the rate of improvement and mortality. The rate of improvement was evaluated via changes in clinical manifestations, biochemical parameters of liver function, hepatitis B virus deoxyribonucleic acid (HBV-DNA) levels, and prothrombin activity (PTA). Moreover, the mortality rate in the corresponding studies was measured during the treatment. The secondary outcomes were the incidence of complications, including gastrointestinal bleeding, lung infection, bacterial peritonitis, hepatic encephalopathy, hepatorenal syndrome, electrolyte imbalance, and ascites.
5. Data Extraction
Two authors (Luo and Zhang) independently extracted data from the included studies and reviewed the full text. Afterward, they discussed and checked the disagreements with the third member of the reviewing team (Da-Zhi Zhang). Data were extracted considering: (I) study: title, author, year, and location, diagnosis of patients, design, and sample size; (II) interventions: corticosteroids types and dosage, administration time, and follow-up time; (III) conventional treatment: types of antiviral drug; (IV) study outcomes: the rate of improvement, mortality rate, and the incidence of complications.
5.1. Quality Score
We used the modified Jadad scale to assess the quality of the selected studies, based on the description generation of allocation sequence, allocation concealment, double blinding, deviations, and withdrawals.
5.2. Statistical Analysis
The meta-analysis was carried out using Stata 12.0 software (Stata Company, College Station, Texas, USA). Odds ratios (ORs) with 95% confidence intervals (95% CIs) were calculated to compare the outcome in glucocorticoids plus conventional group and conventional group. Cochran’s Q test and I-squared index was assessed to evaluate heterogeneity between the groups. When P > 0.05 in Cochran’s Q test and I2 < 50%, the heterogeneity was absent. Mantel-Haenszel method was applied for a fixed-effects model, and P < 0.05 was considered statistically significant. Publication bias was examined using the Begg’s and Egger’s test. When P < 0.05, the bias was considered significant.
6. Results
6.1. Characteristics of the Included Studies
In this meta-analysis, 1259 articles were initially identified in the initial search as described above (Figure 1), then after removing duplicates items, 1187 articles were assessed and screened with regard to the title and abstract. Of these articles, 72 full-text studies were further evaluated regarding the inclusion and exclusion criteria. Finally, 10 studies met the inclusion criteria and were included in the meta-analysis.

Figure 1.
Study selection process. Of the 1259 studies initially identified from our electronic searches, 10 met the inclusion criteria. RCT: randomized controlled trial.
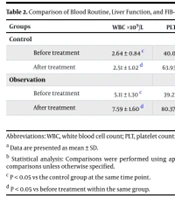
The main characteristics of the included studies are listed in Table 1. Of the 891 patients, 446 patients received combination therapy and 445 patients received conventional therapy. All studies were from China and published between 2011 and 2016. The detailed information regarding the liver biochemical markers is shown in Supplementary File Appendix 1. Among the 10 studies, improvement rate (827 patients) was reported in nine studies (12-19, 26), the mortality rate (439 patients) was reported in seven studies (14-19, 27); however, none of the studies reported liver transplantation rate. Furthermore, gastrointestinal bleeding (599 patients) was reported in six studies (13, 14, 16-19). Lung infection (405 patients) was reported in three studies (13, 17, 27). Bacterial peritonitis (465 patients) was reported in four studies (13, 14, 17, 27). Hepatic encephalopathy (663 patients) was reported in seven studies (13, 14, 16-19, 27). Hepatorenal syndrome (510 patients) was reported in four studies (13, 14, 18, 19). Electrolyte imbalance (159 patients) was reported in two studies (17, 18). Ascites (389 patients) was reported in three studies (13, 16, 17). The type and dose of glucocorticoid received by the patients in the combination group were different. Patients in four studies were randomized to receive dexamethasone (2.5 - 10 mg/day). Patients in two studies used methylprednisolone (1 mg/kg/day). Patients in two studies were treated with prednisone (20 mg/day to 50 - 60 mg/day). Patients in one study initiated methylprednisolone 1 mg/kg/day and changed to prednisolone 0.5 mg/kg/day. Patients in another study used hydrocortisone 25 mg/day. The characteristic of glucocorticoid treatment included in this meta-analysis is shown in Table 2. Based on the Jadad scale, we evaluated the methodological quality data of the included trails listed in Supplementary File Appendix 2.
Table 1.
Baseline Characteristics of Studies Included in the Meta-Analysis: Demographic Parametersa
| First Author, Ref. | Year | Location | Age, y, (Mean ± SD) | Gender, Male/Female | Patients, No. | Study Design |
|---|---|---|---|---|---|---|
| Wu, (12) | 2011 | China | (31.9 ± 7.7)/(32.5 ± 8.2) | 32/36 | 43/44 | RCT |
| Shu-Sheng, (13) | 2014 | China | (47.25 ± 13.15)/(45.31 ± 12.22) | 127/135 | 150/150 | RCT |
| Lei, (14) | 2015 | China | NA | NA | 30/30 | RCT |
| Hui-Zhen, (15) | 2012 | China | NA | 30/30 | 40/36 | RCT |
| Lin-Fang, (16) | 2016 | China | (48.61 ± 12.41)/(47.26 ± 14.13) | NA | 26/22 | RCT |
| Xiu-Mei, (17) | 2012 | China | (39.765 ± 5.101)/(41.054 ± 5.998) | 13/12 | 21/20 | RCT |
| Bo, (18) | 2016 | China | NA | NA | 59/59 | RCT |
| Jin-Hui, (19) | 2014 | China | NA | NA | 12/20 | RCT |
| Wei-Mi, (26) | 2012 | China | NA | NA | 33/32 | RCT |
| Long Yun, (27) | 2016 | China | NA | NA | 32/32 | RCT |
Abbreviations: SD, standard deviation; NA, not available; RCT, randomized controlled trial.
aValues denote patients in the glucocorticoids plus conventional therapy group (before the slash) and those in the conventional therapy group (after the slash).
Table 2.
Characteristics of Glucocorticoids Treatment Included in This Meta-Analysis
| First Author, Ref. | Year | Type, Dose | Duration, days | Follow-Up, Time, days |
|---|---|---|---|---|
| Wu, (12) | 2011 | Dexamethasone, 10 mg/day | 7 | NA |
| Shu-Sheng, (13) | 2014 | Dexamethasone, 10 mg/day | 3 to 5 | 28 |
| Lei, (14) | 2015 | Methylprednisolone, 1 mg/kg/day, gradually reduced and changed to Prednisolone, 0.5 mg/kg/day, gradually reduced | 56 | 56 |
| Hui-Zhen, (15) | 2012 | Prednisolone, 50 - 60mg/day, gradually reduced | 56 | 84 |
| Lin-Fang, (16) | 2016 | Methylprednisolone,1 mg/kg/day, gradually reduced | 14 | 28 |
| Xiu-Mei, (17) | 2012 | Prednisolone, 20 mg/day, gradually reduced | 56 | 56 |
| Bo, 2016 (18) | Hydrocortisone, 25 mg/day | 28 | 28 | |
| Jin-Hui, (19) | 2014 | Dexamethasone, 2.5 mg/day | 14 | 56 |
| Wei-Ming, (26) | 2012 | Dexamethasone, 10 mg/day, gradually reduced | 21 | 28 |
| Yun, (27) | 2016 | Methylprednisolone, 1 mg/kg/day, gradually reduced | 30 | 30 |
Abbreviation: NA, not available.
6.2. Outcomes
6.2.1. Primary Outcome
6.2.1.1. The Rate of Improvement
Nine studies containing 827 patients reported improvement rates. Patients treated with glucocorticoid plus conventional therapy achieved a greater improvement rate compared to patients treated with conventional therapy (OR = 3.98; 95% CI [2.80, 5.66]; P = 0.000, Figure 2). No significant heterogeneity existed across the studies (P = 0.158; I2 = 32.5%); thus the fixed-effect model was applied.

Figure 2.
Pooled comparison of the rate of improvement in the glucocorticoid therapy group and control group
6.2.1.2. Mortality Rate
Seven trials containing 439 patients reported mortality rates in which three studies reported the information of 4-week mortality, 3 reported the information of 8-week mortality, and the one reported the information of 12-week mortality. By analyzing these seven studies together, our result demonstrated that glucocorticoid plus conventional therapy reduced the mortality rate of patients with HBV-related liver failure, and the difference was statistically significant (OR = 0.38, 95% CI [0.20, 0.74], P = 0.004, Figure 3). No statistical heterogeneity was detected among the studies and we chose the fixed effects model (P = 0.648, I2 = 0.0%).

Figure 3.
Forest plot showing on the occurrence of the mortality
6.2.2. Secondary Outcomes
6.2.2.1. Complications
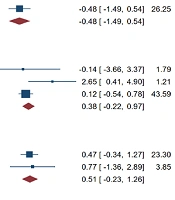
We conducted a complications analysis to compare the incidence of complications between the combination group and the control group (Table 3). Our data showed that the addition of glucocorticoid reduced the rate of hepatic encephalopathy (OR = 0.34, 95% CI [0.19, 0.60], P = 0.000), hepatorenal syndrome (OR = 0.22, 95% CI [0.10, 0.47], P = 0.000), electrolyte imbalance (OR = 0.27, 95% CI [0.12, 0.62], P = 0.002), and ascites (OR = 0.50, 95% CI [0.28, 0.90], P = 0.021). No statistically significant differences were found between the two groups regarding the incidence of complication for lung infection (OR = 0.76, 95% CI [0.27, 2.10], P = 0.595), gastrointestinal bleeding (OR = 0.48, 95% CI [0.23, 1.00], P = 0.050), and bacterial peritonitis (OR = 0.70, 95% CI [0.31, 1.58], P = 0.396). The results showed no statistical heterogeneity in the above complications analysis (P > 0.05, I2 < 50%) and the fixed-effect model was applied.
Table 3.
Results of Complication Analysis Evaluating the Differences Between the Combination Group and Control Groupa
| Complications | Studies, No. | Patients with Complications, No. | OR | 95% CI | P Value | I2 |
|---|---|---|---|---|---|---|
| Hepatic encephalopathy | 7 | 17/49 | 0.34 | 0.19 to 0.60 | 0.000 | 48.3% |
| Hepatorenal syndrome | 3 | 8/35 | 0.22 | 0.10 to 0.47 | 0.000 | 37.9% |
| Electrolyte imbalance | 2 | 10/27 | 0.27 | 0.12 to 0.62 | 0.002 | 0.0% |
| Ascites | 3 | 21/36 | 0.50 | 0.28 to 0.90 | 0.021 | 0.0% |
| Lung infection | 3 | 7/9 | 0.76 | 0.27 to 2.10 | 0.595 | 0.0% |
| Gastrointestinal bleeding | 6 | 13/24 | 0.48 | 0.23 to 1.00 | 0.050 | 8.8% |
| Bacterial peritonitis | 4 | 11/15 | 0.70 | 0.31 to 1.58 | 0.396 | 0.0% |
Abbreviations: CI, confidence interval; OR, odds ratio.
aValues denote patients in the glucocorticoids plus conventional therapy group (before the slash) and those in the conventional therapy group (after the slash).
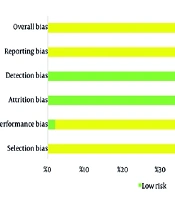
6.3. Publication Bias Analysis
Begg’s and Egger’s regression test was used for evaluating the publication bias of the literature, and there was no evidence of publication bias in this meta-analysis (Supplementary File Appendix 3).
7. Conclusions
Several associations for the study of liver diseases (the Asian-Pacific Association, the American Association or the European Association) have not recommended glucocorticoids plus conventional therapy in combination form for liver failure, except for Chinese guidelines. Our study investigated published data on glucocorticoids plus conventional therapy and found that combination therapy reduces the mortality rate without increasing the incidence of complications in Chinese patients.
Although liver failure is recognized as a clinical entity in chronic viral hepatitis, its impact continues to be associated with greater morbidity and mortality (28, 29). The clinical treatment of liver failure includes standard medical treatment, artificial liver treatment, stem cell transplantation, and liver transplantation. Liver transplantation is the definite and most effective therapy for patients with liver failure without malignancies who progressed to serious liver deterioration (30). Artificial liver, especially the bioartificial liver, also plays an important role in the treatment of liver failure. However, the shortage of liver donors in China and the inaccessibility of artificial liver in economically backward areas have emphasized medical treatment rather than liver transplantation. Therefore, the evaluation of standard medical treatment for hepatitis B patients with severe exacerbation is necessary.
Glucocorticoids as immunomodulatory agents have been applied to treat allergic and chronic inflammatory diseases, such as asthma, dermatitis and rheumatoid arthritis since the 1950s (31, 32). Several recent RCTs showed that a combination of glucocorticoids and conventional treatment was superior to conventional monotherapy (33-36); however, other reports claimed that mono-therapies and combination therapy had similar results (37).
Our data implied that combination therapy (glucocorticoid plus conventional) showed better improvement rate and mortality rate than conventional monotherapy. Anti-inflammatory actions of glucocorticoids could be beneficial to stop progressive liver deterioration (10). In addition, their capability of preventing from cytolysis of infected hepatocytes (11), and regulating the plasma levels of TNF, IL-6, CXCL8 (IL-8), and CCL2 (MCP-1) may also play a vital role (38). Importantly, this positive trend could impute the clinical use of blood products, antibiotics, proton pump inhibitors, and nucleoside (acid) analogues in the treatment of liver failure.
Liver failure can lead to the infection, bleeding, and hepatorenal syndrome (39), suggesting whether therapy with glucocorticoids could induce or aggravate the above complications. Our results demonstrated that the addition of glucocorticoid to conventional therapy did not result in an increased incidence of hepatic encephalopathy, hepatorenal syndrome, electrolyte imbalance or ascites in patients with HBV-related hepatic failure. One reason to explain the effectiveness of combination therapy in the current study compared to others could be the administration of corticosteroids for longer duration and the presence of infection or HBV replication.
There are some limitations to this meta-analysis. First, there are differences in the type, dose and duration of glucocorticoid among the studies included. Second, the long-term durability, safety, and side effects of corticosteroids had not been established. Third, the pathophysiology and the condition of patients varied in different types of liver failure, including ALF, SALF, ACLF, and CLF. These patients would have variable manifestations and outcomes. However, there was not enough data to perform subgroup analysis. Additionally, since all of the data in our meta-analysis are from China, future RCT studies on the use of combination therapy from all over the world will provide a better understanding. Finally, the ideal timing for beginning this treatment in the clinical course of the disease is unknown. Thus we still need to accumulate more data in this field to determine the optimal beginning time, type, dose, and duration of corticosteroids.
In summary, corticosteroids improve efficacy in patients with HBV-related hepatic failure without increasing the risk of mortality or complications. Our study provides comprehensive evidence in initiating glucocorticoid plus conventional therapy as a reasonable strategy in treating patients with HBV-related liver failure.