

1. Background
2. Objectives
3. Methods
3.1. Sample Size Calculation
3.2. Subjects
3.3. Ethics
3.4. Statistical Analysis
4. Results
| Variables | PCOS Group | Control Group | P-Value |
|---|---|---|---|
| Number of participants | 61 | 35 | |
| Age (y) | 27.92 ± 7.04 | 29.93 ± 5.94 | 0.11 b |
| Body weight (kg) | 68.61 ± 12.43 | 66.58 ± 10.03 | 0.43 b |
| Height (cm) | 158.87 ± 5.38 | 158.89 ± 6.21 | 0.71 b |
| BMI (kg/m2) | 27.24 ± 5.16 | 26.42 ± 4.02 | 0.44 b |
| WCF (cm) | 82.53 ± 11.00 | 82.92 ± 10.76 | 0.89 b |
| Physical activity | 0.20 c | ||
| < 3 times/wk (n) | 22 | 13 | |
| ≥ 3 times/wk (n) | 49 | 12 | |
| FBS (mg/dL) | 101.15 ± 9.32 | 104 ± 11.07 | 0.26 d |
| Insulin (µU/mL) | 12.48 ± 6.12 | 9.64 ± 4.22 | 0.024 d |
| HOMA-IR | 3.22 ± 1.76 | 2.55 ± 1.20 | 0.011 d |
| Osteocalcin (ng/mL) | 13.83 ± 7.94 | 10.95 ± 5.38 | 0.12 d |
| Vitamin D (ng/mL) | 24.135 ± 10.520 | 24.00 ± 9.46 | 0.70 b |
| PTH (pg/mL) | 35.53 ± 21.01 | 43.34 ± 21.20 | 0.10 b |
| Corrected calcium (mg/dL) | 8.72 ± 0.34 | 8.63 ± 0.34 | 0.23 b |
| Phosphorus (mg/dL) | 3.99 ± 0.53 | 3.73 ± 0.49 | 0.025 b |
| Testosterone (ng/mL) | 0.52 ± 0.18 | 0.35 ± 0.10 | 0.0001 d |
| Estradiol (pg/mL) | 135.04 ± 65.39 | 127.35 ± 59.03 | 0.59 b |
| DHEAS (µg/mL) | 2.01 ± 0.89 | 1.63 ± 0.67 | 0.013 d |
| LH (mIU/mL) | 7.90 ± 6.17 | 4.37 ± 2.82 | 0.003 d |
| FSH (mIU/mL) | 5.52 ± 2.80 | 5.45 ± 3.03 | 0.80 d |
| LS BMD (g/cm2) | 0.99 ± 0.11 | 1.00 ± 0.12 | 0.61 b |
| LS Z-score | -0.45 ± 1.02 | -0.28 ± 1.13 | 0.48 b |
| FN BMD (g/cm2) | 0.80 ± 0.10 | 0.78 ± 0.12 | 0.64 b |
| FN Z-score | -0.40 ± 0.98 | -0.37 ± 1.09 | 0.88 b |
| TH BMD (g/cm2) | 0.92 ± 0.12 | 0.90 ± 0.14 | 0.53 b |
| TH Z-score | -0.15 ± 0.98 | -0.20 ± 1.16 | 0.76 b |
| DR BMD (g/cm2) | 0.56 ± 0.04 | 0.55 ± 0.04 | 0.39 b |
| DR Z-score | -0.14 ± 0.75 | -0.26 ± 0.76 | 0.47 b |
Abbreviations: PCOS, polycystic ovary syndrome; BMI, body mass index; WCF, waist circumference; FBS, fasting blood sugar; HOMA-IR, homeostatic model assessment of estimated insulin resistance; PTH, parathyroid hormone; DHEAS, dehydroepiandrosterone sulfate; LH, luteinizing hormone; FSH, follicle-stimulating hormone; LS, lumbar spine; FN, femoral neck; TH, total hip; DR, distal radius; BMD, bone mineral density; SD, standard deviation.
a The data are expressed as mean ± SD.
b Independent t-test
c Chi-square test
d Mann-Whitney U test
| BMI r(p), No. (%) | HOMA-IR r(p), No. (%) | Testosterone r(p), No. (%) | DHEAS r(p), No. (%) | Osteocalcin r(p), No. (%) | PTH r(p), No. (%) | |
|---|---|---|---|---|---|---|
| LS BMD | ||||||
| PCOS group | 0.24 b (0.06) | 0.11 c (0.42) | -0.14 c (0.27) | 0.02 c (0.87) | -0.18 c (018) | -0.17 b (0.20) |
| Control group | 0.30 b (0.10) | 0.04 b (0.81) | 0.01 b (0.97) | 0.23 c (0.22) | -0.40 b (0.03) | -0.10 b (0.61) |
| LS Z-score | ||||||
| PCOS group | 0.25 b (0.06) | 0.10 c (0.44) | -0.14 c (0.28) | 0.01 c (0.94) | -0.19 c (0.15) | -0.16 b (0.22) |
| Control group | 0.33 b (0.07) | 0.06 b (0.77) | 0.03 b (0.87) | 0.24 c (0.19) | -0.42 b (0.02) | -0.11 b (0.54) |
| FN BMD | ||||||
| PCOS group | 0.53 b (0.0001) | 0.42 c (0.001) | -0.02 c (0.88) | 0.27 c (0.03) | 0.03 c (0.83) | -0.09 b (0.51) |
| Control group | 0.53 b (0.001) | 0.25 b (0.18) | -0.41 b (0.02) | 0.19 c (0.32) | -0.16 b (0.39) | 0.33 b (0.08) |
| FN Z-score | ||||||
| PCOS group | 0.60 b (0.0001) | 0.42 c (0.001) | -0.04 c (0.76) | 0.22 c (0.08) | -0.05 c (0.72) | -0.06 b (0.66) |
| Control group | 0.63 b (0.0001) | 0.27 b (0.14) | -0.41 b (0.03) | 0.16 c (0.38) | -0.19 b (0.33) | 0.32 b (0.09) |
| TH BMD | ||||||
| PCOS group | 0.61 b (0.0001) | 0.36 c (0.006) | -0.02 c (0.88) | 0.27 c (0.03) | -0.14 c (0.28) | -0.23 b (0.07) |
| Control group | 0.67 c (0.0001) | 0.37 c (0.04) | -0.25 c (0.18) | 0.14 c (0.46) | -0.09 c (0.63) | -0.13 c (0.48) |
| TH Z-score | ||||||
| PCOS group | 0.70 b (0.0001) | 0.38 c (0.003) | -0.02 c (0.87) | 0.20 c (0.12) | -0.20 c (0.14) | -0.15 b (0.24) |
| Control group | 0.71 c (0.0001) | 0.40 c (0.03) | -0.25 c (0.19) | 0.13 c (0.48) | -0.11 c (0.55) | -0.13 c (0.50) |
| DR BMD | ||||||
| PCOS group | 0.23 b (0.83) | 0.13 c (0.31) | -0.26 c (0.05) | 0.07 c (0.57) | 0.05 c (0.71) | -0.06 b (0.63) |
| Control group | 0.54 b (0.002) | 0.32 b (0.08) | -0.25 b (0.18) | -0.14 c (0.45) | -0.33 b (0.07) | -0.11 b (0.55) |
| DR Z-score | ||||||
| PCOS group | 0.20 b (0.15) | 0.09 c (0.53) | -0.25 c (0.07) | 0.02 c (0.87) | 0.09 c (0.53) | -0.02 b (0.87) |
| Control group | 0.59 b (0.001) | 0.33 b (0.07) | -0.23 b (0.22) | -0.16 c (0.41) | -0.35 b (0.06) | -0.13 b (0.49) |
Abbreviations: PCOS, polycystic ovary syndrome; BMI, body mass index; HOMA-IR, homeostatic model assessment of estimated insulin resistance; DHEAS, dehydroepiandrosterone sulfate; PTH, parathyroid hormone; FN, femoral neck; LS, lumbar spine; TH, total hip; DR, distal radius; BMD, bone mineral density.
a Bivariate correlation
b Pearson correlation coefficient
c Spearman’s correlation coefficient
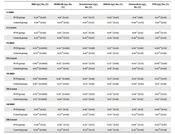
| Bone Parameters | PCOS Group | Control Group | ||
|---|---|---|---|---|
| BMI B b(95% CI) c | HOMA-IR B b(95% CI) c | BMI B b(95% CI) c | HOMA-IR B b(95% CI) c | |
| LS BMD (g/cm2) | 0.005 (0.00 - 0.01) | 0.01 (-0.01 - 0.02) | 0.01 (-0.00 - 0.02) | 0.01 (-0.03 - 0.04) |
| LS Z-score | 0.05 (-0.00 - 0.10) | 0.07 (-0.08 - 0.23) | 0.09 (-0.01 - 0.19) | 0.05 (-0.31 - 0.42) |
| FN BMD (g/cm2) | 0.01 (0.01 - 0.01) | 0.02 (0.09 - 0.04) | 0.02 (0.01 - 0.03) | 0.03 (-0.01 - 0.06) |
| FN Z-score | 0.11 (0.07 - 0.15) | 0.23 (0.09 - 0.37) | 0.17 (0.09 - 0.25) | 0.25 (-0.09 - 0.58) |
| TH BMD (g/cm2) | 0.01 (0.01 - 0.02) | 0.02 (0.01 - 0.04) | 0.02 (0.01 - 0.03) | 0.04 (0.00 - 0.08) |
| TH Z-score | 0.13 (0.09 - 0.17) | 0.22 (0.77 - 0.36) | 0.21 (0.14 - 0.28) | 0.36 (0.01 - 0.71) |
| DR BMD (g/cm2) | 0.002 (0.00 - 0.004) | 0.003 (-0.004 - 0.009) | 0.005 (0.002 - 0.008) | 0.01 (-0.00 - 0.02) |
| DR Z-score | 0.03 (-0.01 - 0.07) | 0.03 (-0.83 - 0.15) | 0.11 (0.05 - 0.17) | 0.21 (-0.02 - 0.44) |
Abbreviations: PCOS, polycystic ovary syndrome; BMI, body mass index; HOMA-IR homeostatic model assessment of estimated insulin resistance; LS, lumbar spine; FN, femoral neck; TH, total hip; DR, distal radius; BMD, bone mineral density.
a Univariate linear regression analysis
b B, unstandardized Beta
c CI, the confidence interval for Beta
| Bone Parameters | PCOS Group | Control Group | ||
|---|---|---|---|---|
| BMI B b (95% CI) c | HOMA-IR B b (95% CI) c | BMI B b (95% CI) c | HOMA-IR B b (95% CI) c | |
| LS BMD | -0.01 (-0.08 - 0.06) | 0.01 (-0.01 - 0.03) | 0.01 (0.00 - 0.03) | -0.02 (-0.06 - 0.02) |
| LS Z-score | -0.06 (-0.72 - 0.59) | 0.07 (-0.1 - 0.23) | 0.11 (-0.004 - 0.234) | -0.14 (-0.51 - 0.22) |
| FN BMD | 0.06 (0.01 - 0.12) | 0.02 (0.01 - 0.04) | 0.02 (0.01 - 0.03) | -0.01 (-0.03 - 0.02) |
| FN Z-score | 0.60 (0.08 - 1.13) | 0.21 (0.08 - 0.34) | 0.19 (0.11 - 0.26) | -0.06 (-0.29 - 0.17) |
| TH BMD | 0.08 (0.02 - 0.14) | 0.02 (0.01 - 0.04) | 0.03 (0.02 - 0.04) | 0.00 (-0.03 - 0.03) |
| TH Z-score | 0.65 (0.14 - 1.17) | 0.18 (0.05 - 0.31) | 0.23 (0.15 - 0.31) | -0.01 (-0.23 - 0.24) |
| DR BMD | -0.01 (-0.04 - 0.01) | 0.003 (-0.003 - 0.009) | 0.005 (0.001 - 0.009) | 0.003 (-0.01 - 0.02) |
| DR Z-score | -0.14 (-0.62 - 0.34) | 0.05 (-0.07 - 0.16) | 0.09 (0.01 - 0.17) | 0.06 (-0.18 - 0.30) |
Abbreviations: PCOS, polycystic ovary syndrome; BMI, body mass index; HOMA-IR, homeostatic model assessment of estimated insulin resistance; DHEAS, dehydroepiandrosterone sulfate; LS, lumbar spine; FN, femoral neck; TH, total hip; DR, distal radius; BMD, bone mineral density.
a Multivariate regression analysis
b B, unstandardized Beta
c CI, the confidence interval for Beta