
Fulltext
Introduction
Nowadays, most people are aware of the link between obesity and health risks. It is widely believed that cardiovascular disease is a major cause of morbidity and mortality among obese populations.v' It has been shown that overweight and obesity are associated with increased cardiovascular disease risk factors such as, hypertension':" and type 2 diabetes.' There also exists evidence suggesting that obesity and high blood pressure are disorders that are closely linked, particularly when obesity is characterized by a central fat distribution.3,6 The evaluation of central adiposity by way of the waist-to-hip circumference ratio (WHR) has been recognized as a substantial component in the assessment of cardiovascular disease risk factors due to a positive association between high WHR and hypertension." The relationship between overall fat distribution and central adiposity with hypertension, recognized in middle age, has received little attention in young adults. Surprisingly, there is substantially less published information about the prevalence of overweight, obesity and their associations to hypertension in Iran, particularly among university students. It is therefore, the purpose of this study to report on the prevalence of overweight and obesity and their relationship with high blood pressure for the prediction of cardiovascular disease risk factors in male university students in Kerman, a province in the southeast of Iran.
Nowadays, most people are aware of the link between obesity and health risks. It is widely believed that cardiovascular disease is a major cause of morbidity and mortality among obese populations.v' It has been shown that overweight and obesity are associated with increased cardiovascular disease risk factors such as, hypertension':" and type 2 diabetes.' There also exists evidence suggesting that obesity and high blood pressure are disorders that are closely linked, particularly when obesity is characterized by a central fat distribution.3,6 The evaluation of central adiposity by way of the waist-to-hip circumference ratio (WHR) has been recognized as a substantial component in the assessment of cardiovascular disease risk factors due to a positive association between high WHR and hypertension." The relationship between overall fat distribution and central adiposity with hypertension, recognized in middle age, has received little attention in young adults. Surprisingly, there is substantially less published information about the prevalence of overweight, obesity and their associations to hypertension in Iran, particularly among university students. It is therefore, the purpose of this study to report on the prevalence of overweight and obesity and their relationship with high blood pressure for the prediction of cardiovascular disease risk factors in male university students in Kerman, a province in the southeast of Iran.
Materials and Methods
Subjects
Five hundred and thirty seven male university students, aged, 18.3 to 29.7, years who enrolled for general physical education classes during the winter semester of 200 I at Shahid Bahonar University of Kerman in Kerman, Iran, were recruited to participate in the present study. In order to recruit the subjects, students from 30 classes were randomly selected. Written informed consent was obtained from all subjects prior to their participation in the study.
Subjects
Five hundred and thirty seven male university students, aged, 18.3 to 29.7, years who enrolled for general physical education classes during the winter semester of 200 I at Shahid Bahonar University of Kerman in Kerman, Iran, were recruited to participate in the present study. In order to recruit the subjects, students from 30 classes were randomly selected. Written informed consent was obtained from all subjects prior to their participation in the study.
Anthropometrical measurements
Anthropornetrical measurements were taken using standard apparatus with the subjects wearing light underwear and without shoes. A trained individual took all measurements. Weight was measured in the upright position with a weighting scale to the nearest 0.01 kilogram (kg). Each day the scale was calibrated with a standard weight. Height was measured to the nearest 0.1 ern. All measurements were taken using a non-stretching tape. Body mass index (BMI) was calculated as weight (kg) divided by height squared (rn") to estimate overall body fat distribution and was classified into four categories according
to Baray.' Thus, underweight was defined as BMI < 20.00, normal weight as BMI 20.00 - 24.99, overweight as BMI 25.00 - 29.99 and obesity as BMf ~ 30.00 Kg/m2. Waist was measured horizontally at the level just above the uppermost border of the iliac crest. The measurement was made at a normal minimal respiration' Hip was measured as the maximum circumference over the buttocks." Central obesity was also calculated and defined on the basis of WHR. The cut-off value of central obesity was considered ~ 0.92.10 .
Anthropornetrical measurements were taken using standard apparatus with the subjects wearing light underwear and without shoes. A trained individual took all measurements. Weight was measured in the upright position with a weighting scale to the nearest 0.01 kilogram (kg). Each day the scale was calibrated with a standard weight. Height was measured to the nearest 0.1 ern. All measurements were taken using a non-stretching tape. Body mass index (BMI) was calculated as weight (kg) divided by height squared (rn") to estimate overall body fat distribution and was classified into four categories according
to Baray.' Thus, underweight was defined as BMI < 20.00, normal weight as BMI 20.00 - 24.99, overweight as BMI 25.00 - 29.99 and obesity as BMf ~ 30.00 Kg/m2. Waist was measured horizontally at the level just above the uppermost border of the iliac crest. The measurement was made at a normal minimal respiration' Hip was measured as the maximum circumference over the buttocks." Central obesity was also calculated and defined on the basis of WHR. The cut-off value of central obesity was considered ~ 0.92.10 .
Blood pressure measurement
Blood pressure was measured, using the standard mercury sphygmomanometer, on the right arm with a subject in the upright sitting position, following at least 5 min rest. Hypertension was defined as systolic blood pressure (SBP) > 140 mmHg, and diastolic blood pressure (DBP) >90mmHg. II
Blood pressure was measured, using the standard mercury sphygmomanometer, on the right arm with a subject in the upright sitting position, following at least 5 min rest. Hypertension was defined as systolic blood pressure (SBP) > 140 mmHg, and diastolic blood pressure (DBP) >90mmHg. II
Statistical analyses
Statistical analysis was carried out using the statistical program available in SPSS version 9.0. Descriptive statistics for anthropometric characteristics and SBP and DBP were calculated. Partial correlation coefficient was used to quantify the association between independent variables (BMI and WHR) and dependent variables (SBP and DBP). Linear regression analysis was used to assess the influence of BMl and WHR on the variance of SBP and DBP. All tests for statistical significance were two tailed and significance was selected at P-value <0.05.
Statistical analysis was carried out using the statistical program available in SPSS version 9.0. Descriptive statistics for anthropometric characteristics and SBP and DBP were calculated. Partial correlation coefficient was used to quantify the association between independent variables (BMI and WHR) and dependent variables (SBP and DBP). Linear regression analysis was used to assess the influence of BMl and WHR on the variance of SBP and DBP. All tests for statistical significance were two tailed and significance was selected at P-value <0.05.
Results
Anthropometric and blood pressure charac- teristics of the subjects are shown in Table I. Based on BMI according to definition used, descriptive analysis revealed that 38.4% of the study population was classified as underweight, 45.8% as normal weight, 13.6% as overweight, and 2.2% as obese (Fig. 1). The BMl cut-off points for overweight and obesity were ~ 84th and ~ 97th, respectively. The results revealed that at the WHR cut-off point recommended for central obesity in men (WHR ~ 0.92 ern), , abdominal adiposity was present in 11.4% of the subjects. Partial correlation controlled for age revealed strong positive correlation between BMI and WHR (r = 0.680, P < 0.0001) (Fig. 2).Inspection of the data obtained for the hypertension, indicated that 33 subjects of the study population
(4.8%) had systolic high blood pressure, and 21 (4%) had diastolic high blood pressure. Results of the partial correlation coefficient
controlled for age, indicated a significant positive correlation between SBP and DBP (r= 0.617, Plation revealed that, there were significant correlation between the independent and dependent variables. BMI was positively corre- lated with SBP (r = OAI0, P
Anthropometric and blood pressure charac- teristics of the subjects are shown in Table I. Based on BMI according to definition used, descriptive analysis revealed that 38.4% of the study population was classified as underweight, 45.8% as normal weight, 13.6% as overweight, and 2.2% as obese (Fig. 1). The BMl cut-off points for overweight and obesity were ~ 84th and ~ 97th, respectively. The results revealed that at the WHR cut-off point recommended for central obesity in men (WHR ~ 0.92 ern), , abdominal adiposity was present in 11.4% of the subjects. Partial correlation controlled for age revealed strong positive correlation between BMI and WHR (r = 0.680, P < 0.0001) (Fig. 2).Inspection of the data obtained for the hypertension, indicated that 33 subjects of the study population
(4.8%) had systolic high blood pressure, and 21 (4%) had diastolic high blood pressure. Results of the partial correlation coefficient
controlled for age, indicated a significant positive correlation between SBP and DBP (r= 0.617, Plation revealed that, there were significant correlation between the independent and dependent variables. BMI was positively corre- lated with SBP (r = OAI0, P
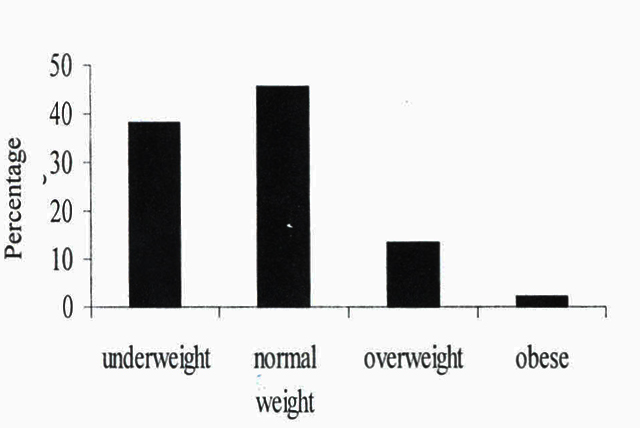
Fig. I. Prevalence of overall body fat distribution by four categories of body mass index, for male Kermanian university students (n = 537)
| Variables | Median | Mean | SD | Range |
| Age (y) | 21.3 | 21.7 | 2.4 | 18.3-29.7 |
| Height (cm) | 175.0 | 174.6 | 6.1 | 157.0-193.0 |
| Weight (kg) | 64.0 | 65.7 | 11.1 | 42.3-109.5 |
| Waist (cm) | 77.0 | 78.7 | 9.2 | 60.0-114.0 |
| Hip (cm) | 91.0 | 92.0 | 6.7 | 58.0-117.0 |
| WHR | 0.85 | 0.85 | 5.3 | 0.74-0.09 |
| BMI (kg/m2) | 21.1 | 21.6 | 3.4 | 14.5-34.2 |
| SBP (mmHg) | 120.0 | 120.8 | 13.4 | 90.0-160.0 |
| DBP (mmHg) | 75.0 | 73.6 | 9.35 | 45.0-100.0 |
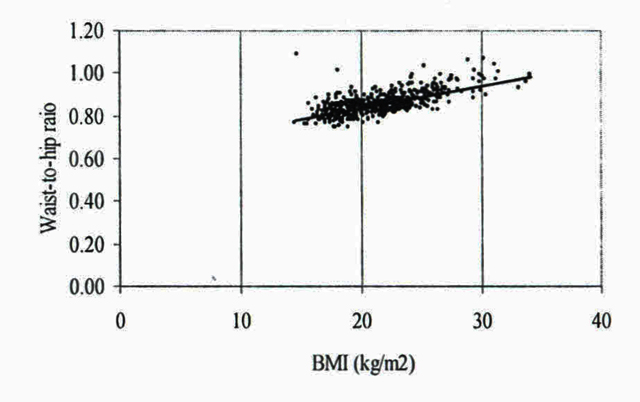
Fig. 2. Relationship between BM I and WHR in 537 Kermanian university, r=0.680, p
Discussion
The purpose of this study was to provide data on the prevalence of overweight and obesity and their associations with hypertension among male Kermanian university students. BMI and WHR were used in the present study for two reasons. First, due to simplicity and reproducibility of height, weight, hip and waist circumferences measurements and second, because both have been recognized as important indicators for estimating cardiovascular disease risk factors, in particular their positive association with hyperten. 124 Sl Oll. ' The results of the present study demon- strated that the overall prevalence of over- weight and obesity were 13.6% and 2,2%, respectively, In addition, according to the present results, 11.4% of the participants had waist-to-hip circumference ratio ~ 0.92,11 The principal finding in this study was that, the prevalence of obesity among the young adult population (18.3 - 29,7 y) was lower than those reported in literature, Ajlouni et al," reported that the prevalence of obesity (BMI 2 30 kg/m2) among Jordanian adult men (25 - 29 y) was 17.8%, In the study conducted by Bonora et al," to examine cardiovascular risk profile in 18 and 38 year old men, the prevalence of obesity (BMI ~ 30 kg/rn") in both groups was 8,5%. In addition, comparison between the mean BMI in the present study with those in the abovementioned studies is also notable, Using the same definition for obesity as the present study (BMI ~ 30 kg/rn"), in both the mean BMls were 24.9 kg/rn' and 25.6 kg/rn", respectively, which are much higher than 21,6 kg/rn' , that of the present study. However, although comparison with some university students in European countries may not be entirely justified, because their data were collected ~s answers provided to questiormaires.l'' the mean BMI in the present study is similar to those reported for England and France (21.8 kg/rn'' and 21.6 kg/m', respectively), but is less than those in Greece, Iceland and Spain (Table 2), The results of the present study showed that the prevalence of hypertension seem low. These are compared with 20,5% of overall hypertension with cut-off points of 140 or 90 mmHg or greater in young subjects aged 15- 24 y.15 Significant positive association between ei- ther BMI or WHR and SBP and DBP was found in the present study. The independent association between BMI and either SBP or DBP is in line with previous findings.f:" Similarly, the results of this study that described the independent relationship between WHR and either SBP or DBP are consistent with previous reports. 19•21 Surprisingly, however, contrasting results have been found in a number of studies, 14,22 Borona et al,14 reported that BMI was an independent predictor for diastolic blood pres sure and not for systolic blood pressure, However, they reported that WHR was not an independent predictor for either systolic or diastolic blood pressures, They argued that failure to find an independent association between WHR and blood pressure might have been due to the fact that most of the study populations were nonobese. This argument is based on the evidence that showed regional fat distribution has an impairment effect on metabolic and haemodynamic measures only when the overall body fat is larger than a cer. ,2324 tam quantity.An important result ofthe present study is a considerably high prevalence of underweight (38.4%) among young male university students. This has been observed to be more 'I 1516 J h bani d common among grr s.' ang or ant an Parvin 16 reported that the prevalence of underweight among high school girls aged 14- 21 years in Kerman, Iran was 54.6%. The authors suggested that "under-nutrition" which has been referred to as an outcome of recent post war socio-economic changes might be one of the causes, although not entirely, this may be true for Kermanian young men as well. An other possible explanation for the tendency toward being underweight among male uni those living far from their family are different, independent samples T-test was calculated. The results revealed a highly statistically significant (P
The purpose of this study was to provide data on the prevalence of overweight and obesity and their associations with hypertension among male Kermanian university students. BMI and WHR were used in the present study for two reasons. First, due to simplicity and reproducibility of height, weight, hip and waist circumferences measurements and second, because both have been recognized as important indicators for estimating cardiovascular disease risk factors, in particular their positive association with hyperten. 124 Sl Oll. ' The results of the present study demon- strated that the overall prevalence of over- weight and obesity were 13.6% and 2,2%, respectively, In addition, according to the present results, 11.4% of the participants had waist-to-hip circumference ratio ~ 0.92,11 The principal finding in this study was that, the prevalence of obesity among the young adult population (18.3 - 29,7 y) was lower than those reported in literature, Ajlouni et al," reported that the prevalence of obesity (BMI 2 30 kg/m2) among Jordanian adult men (25 - 29 y) was 17.8%, In the study conducted by Bonora et al," to examine cardiovascular risk profile in 18 and 38 year old men, the prevalence of obesity (BMI ~ 30 kg/rn") in both groups was 8,5%. In addition, comparison between the mean BMI in the present study with those in the abovementioned studies is also notable, Using the same definition for obesity as the present study (BMI ~ 30 kg/rn"), in both the mean BMls were 24.9 kg/rn' and 25.6 kg/rn", respectively, which are much higher than 21,6 kg/rn' , that of the present study. However, although comparison with some university students in European countries may not be entirely justified, because their data were collected ~s answers provided to questiormaires.l'' the mean BMI in the present study is similar to those reported for England and France (21.8 kg/rn'' and 21.6 kg/m', respectively), but is less than those in Greece, Iceland and Spain (Table 2), The results of the present study showed that the prevalence of hypertension seem low. These are compared with 20,5% of overall hypertension with cut-off points of 140 or 90 mmHg or greater in young subjects aged 15- 24 y.15 Significant positive association between ei- ther BMI or WHR and SBP and DBP was found in the present study. The independent association between BMI and either SBP or DBP is in line with previous findings.f:" Similarly, the results of this study that described the independent relationship between WHR and either SBP or DBP are consistent with previous reports. 19•21 Surprisingly, however, contrasting results have been found in a number of studies, 14,22 Borona et al,14 reported that BMI was an independent predictor for diastolic blood pres sure and not for systolic blood pressure, However, they reported that WHR was not an independent predictor for either systolic or diastolic blood pressures, They argued that failure to find an independent association between WHR and blood pressure might have been due to the fact that most of the study populations were nonobese. This argument is based on the evidence that showed regional fat distribution has an impairment effect on metabolic and haemodynamic measures only when the overall body fat is larger than a cer. ,2324 tam quantity.An important result ofthe present study is a considerably high prevalence of underweight (38.4%) among young male university students. This has been observed to be more 'I 1516 J h bani d common among grr s.' ang or ant an Parvin 16 reported that the prevalence of underweight among high school girls aged 14- 21 years in Kerman, Iran was 54.6%. The authors suggested that "under-nutrition" which has been referred to as an outcome of recent post war socio-economic changes might be one of the causes, although not entirely, this may be true for Kermanian young men as well. An other possible explanation for the tendency toward being underweight among male uni those living far from their family are different, independent samples T-test was calculated. The results revealed a highly statistically significant (P
| Country | N | Age (y) | Weight (kg) . | Height (em) | BMI |
| England | 303 | 20.0±2.0 | 69.0±10A | 178.0±6. | 21.8±2.6 |
| France | 289 | 21.1±2.3 | 68.0±9.3 | 178±7.2 | 21.6±2.2 |
| Greece | 310 | 20.9± 1.9 | 75.0±9.5 | 179.05±5.9 | 23.5±2.4 |
| Iceland | 393 | 21.2±2.9 | 76.0± 10.0 | 182.0±5.9 | 23.0±2.7 |
| Spain | 369 | 21.2±2.6 | 72.0±10.0 | 176.0±6.6 | 23.1±2.7 |
| Current study | 537 | 21.7±2A* | 65.70±11.1 | 176.4±6.1 | 21.6±3.4 |
* Numbers represent Mean ± SD
Acknowledgement
This study was supported by grant from Shahid Bahonar University of Kerman. Theauthor is grateful to associate Professor IanMaddox for reading an earlier draft of thismanuscript. I would like to gratefully thankall the students who participated in this study.My thanks go to Mr Mohamad Reza Saifadinifor his assistance in collecting the data.