
Fulltext
A dramatic increase in the prevalence of overweight and obesity has occurred during the last few decades worldwide[1,2] and is prevalent across gender and ethnic groups[3,4]. Recent statistics also shows that prevalence of overweight continues to increase during the school age and pre-adolescent/adolescent stages[3]. In this stage children attain a rapid growth spurt, characterized by rapid linear growth and deposition of fat mass[3]. Many studies reported that girls had higher average of body fat mass than their boy counterparts[1,4]. Abdominal obesity among girls is shown to be an emerging issue. Boys tend to deposit more fat free mass than fat mass while girls tend to deposit more fat mass than fat free mass[3]. Similar trend has also been demonstrated in Indian school-aged children[5].
Epidemiological literature shows that about one-third of obese pre-school children and about one-half of obese school age children become obese adults[2]. Lifestyle transition and socio-economic improvement have contributed enormously to the escalating problem of overweight and obesity among children in developing countries[5]. A child with obesity is at risk to develop a wide spectrum of adiposity-related diseases and comorbid conditions[1,3]. Hence close monitoring of overweight prevalence in children and adolescents and taking timely preventive measures will be an effective approach in dealing with the problem of obesity.
Seven secondary schools in Kharagpur municipality of Paschim Medinipur district, West Bengal, india were randomly selected and all 1481 girls (Bengalee Hindu and Muslims ethnicity) from the age group of 10-14 studying in these schools were screened for overweight and obesity.
The height and weight measurements were made and recorded following the standard techniques[6]. Height and weight were measured using anthropometric rod and weighing scale to the nearest of 0.1cm and 0.5kg, respectively. Technical errors of measurements (TEM) were computed and they were found to be within acceptable limits. The body mass index (BMI=weight/height2) has been recommended to be used routinely to evaluate obesity in children and adolescents[7].
Two methods for the classification of obesity and overweight were utilized in this study. The first was according to the proposed cut-off points for BMI adopted by the International Obesity Task Force (IOTF)[8], based on international data and linked to the widely accepted adult cut-off points for overweight and obesity (BMI of 25 and 30 kg/m2, respectively). The second was based on CDC growth charts, and more specifically the 85th percentile was taken as a cut-off point for overweight whereas the 95th was taken for obesity[9].
The overall mean values (±SD) of weight, height and BMI of participants were 32.47(±8.37), 139.39(±10.16) and 16.50(±2.85), respectively. According to the BMI cut-off points of IOTF, 6.75% of girls in the study were classified as overweight, whereas obese were 1.01%. Corresponding values using CDC growth charts were 6.89% of girls for overweight and 1.89% of girls for obese. The prevalence of overweight obesity was highest at 14 years of age and lowest at 12 years of age.
Present study also illustrated ethnic specific comparisons of BMI in Fig. 1. When we examined
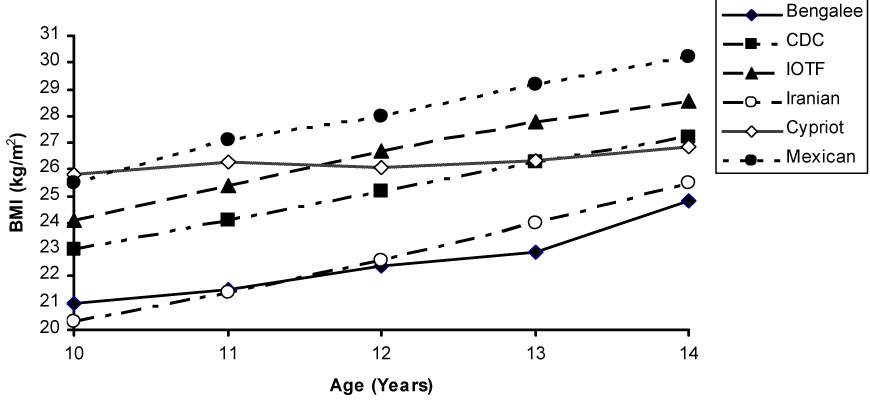
Fig. 1: Comparison of the 95th percentile of BMI values in early adolescent girls from various parts of the world [CDC, IOTF, Sanghai, Cypriot, Mexican].
the early adolescent girls’ 95th BMI percentile curves, Mexican adolescent girls’ [11] percentiles stayed highest on the figure and above the IOTF standards values. Cypriot adolescent girls’ [11] percentiles curve dropped at the age of 12 years. Both curves were above the CDC standard curve. The smoothed curve of Iranian girls was the below the curves of CDC. Interestingly, 95th BMI curve of the Bengalee early adolescent girls lied at the bottom on early ages and increased more sharply with age.
Childhood obesity is a growing national concern. This study and other recent studies[2,5] confirm that it has become a major public health challenge in urban areas of India. The increasing prevalence of obesity in a population is an early indicator of an emerging health burden due to the increasing mortality and morbidity from NCDs in developing societies[2].
School based data in India showed the extent of overweight is most pronounced in the pre-adolescents group[3,5]. A study in urban areas of India (as per IOTF) showed that overweight and obesity among early adolescent school girls was 15.2% and 5.3%, respectively[2]. This probably accounted for the better nutrition of the affluent girl. Prevalence of overweight in the present study was similar to those reported extent of overweight among Bengalee early adolescent girls was 7.20% (IOTF criterion used)[5].
Modern lifestyles (nutritional habits, inactivity and socio-economic improvement) in an obesogenic environment cause an increased prevalence of obesity among children[1,3]. The increasing incidence of overweight during early adolescence in girls is a critical health issue[5].
The present study highlights that childhood overweight/obesity is an emerging health problem that requires effective preventive strategies to halt the epidemic. Targeting interventions at early stages may be effective way of dealing with overweight and obesity.