
Fulltext
Isolated congenital left ventricular diverticulum is a rare congenital heart malformation with an incidence ranging from 0.05% to 0.4%[1]. This lesion was defined by a protrusion of the three-layer left ventricular free walls, and was first described in 1838[1]. Multiple clinical phenotypes were presented in literature, such as chest pain, arrhythmia, systemic embolisation, valve regurgitation, ventricular wall rupture and sudden death. However, most patients would be asymptomatic and detection usually occurred by accident, often during echocardiography. Cases of left ventricular diverticulum accompanying myocarditis were rarely reported. A nine-year-old boy diagnosed with left ventricular diverticulum accompanying acute myocarditis underwent surgical management and was followed up for two years after surgery in our hospital. We proposed that conventional surgical treatments are not suitable for our patient during the period of acute myocarditis, except for heart transplant. A nine-year-old boy who had been suffering from palpitation and edema for half a month was referred to our hospital in 2010. In physical examination a mild systolic heart murmur was auscultated at the apex and the liver was palpated 4 cm below the subcostal margin. Echocardio¬graphy revealed four enlarged cardiac chambers and a diverticulum, 55 mm in diameter and 70 mm in length, without other congenital cardiac malformations. Mild mitral valve regurgitation was detected by color Doppler flow imaging. The left ventricular ejection fraction (EF) and fractional shortening (FS), which mirrored cardiac function, was 33% and 16%, respectively. Magnetic resonance imaging confirmed that the diverticulum with a narrow short neck was connected to the left ventricle. The electrocardiogram showed a few ventricular premature beats. No evidence showed that the patient had a recent viral infection, particularly influenza.
The surgical procedure was performed. The diverticulum was observed to be full of thrombi upon incision. After cleaning the thrombi, the opening (8 mm × 8 mm) to the left ventricle was sewn and closed by a Teflon patch with 4/0 prolene through the incision. A myocardial specimen was harvested and sent for pathological examination. The examination revealed an active lymphocytic myocarditis with cell necrosis and thrombi. Upon surgical manipulation, the echocardiograph indicated exclusion of the diverticulum with only mild mitral valve regurgitation.
The postoperative course was uneventful and vasoactive drugs, like dopamine (6 μg/kg•min-1) and adrenaline (0.05 to 0.1μg/kg•min-1), were administrated for five days. The size of the four cardiac chambers did not change compared with their size before surgery during the two-year follow-up period; whereas more mitral and tricuspid valve regurgitations were observed. Cardiac function was significantly weaker (EF: 28%, FS: 13%) (Table 1 and Fig. 1). The patient suffered from chronic heart failure and had to
Table 1: Echocardiography results measured before and after surgery*
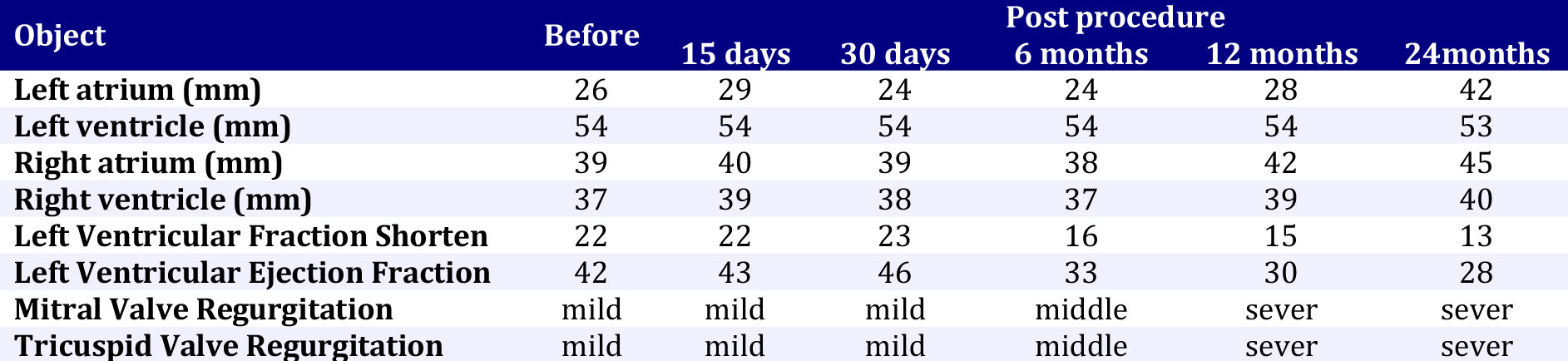
*All the data was measured at the end-diastole dimension in the text and the table
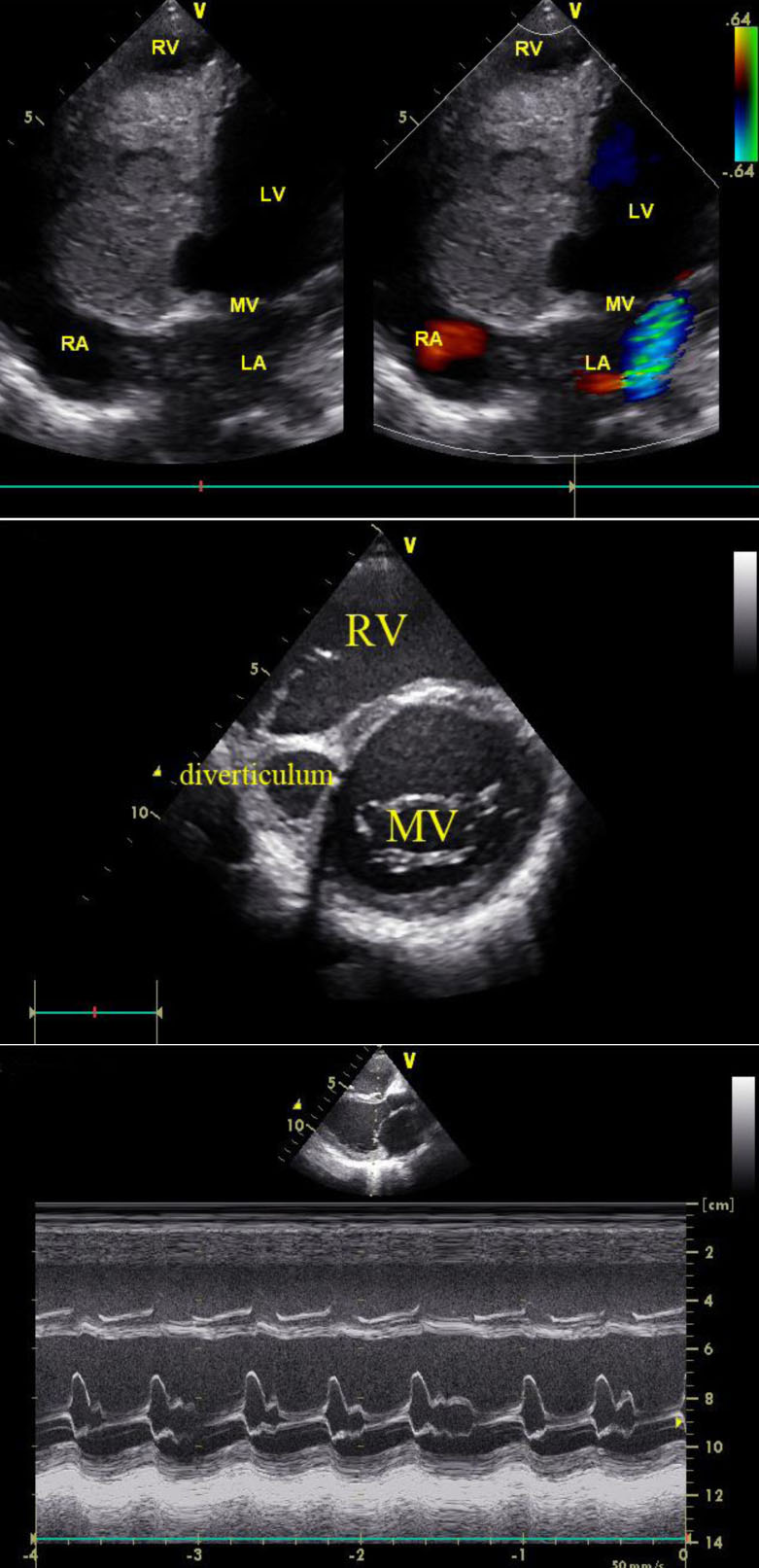
Fig. 1: (A) Color Doppler echo and B-echo showing the left ventricular diverticulum full of thrombi
(B) B-echo 2 and M-echo two years after the surgery showing the resident diverticulum and low heart function
receive digoxin interval treatment because of weaker cardiac function.
Congenital ventricular diverticulum is a rare malformation which is always accompanied by other cardiac malformations, as well as vascular or thoraco-abdominal abnormalities. This malfor-mation can be differentiated from aneurysm, which is a consequence of coronary heart disease, cardiac trauma or hypertrophic cardiomyopathy according to the connection of the neck to the left ventricle. However, certain cases of aneurysm caused by viral myocarditis are similar to congenital diverticulum and are characterised by a narrow connection. These aneurysm cases are called micro-diverticula for their small size[3]. Endocardial biopsy is the golden standard for diagnosing viral myocarditis. In addition, hepatitis C and influenza A viruses are more commonly found in patients with aneurysm and myocarditis[4]. Our patient was subjected to pathological examination, which revealed acute myocarditis symptoms without any virus detected. Therefore, our patient was diagnosed with congenital cardiac diverticulum accompanying acute myocarditis based on morphological and clinical features.
Considering that only a few cases of such incidence have been reported or published in literature, controversies on the treatment and prognosis of congenital cardiac diverticulum accompanying acute myocarditis are ongoing[1]. Frustaci et al (1992) proposed that these combined lesions should not be subjected to surgical manipulation according to the mid-time follow-up[6]. However, majority of patients died because the diverticulum ruptured; therefore, repair was necessary once lesions were diagnosed[7]. Makoto (2003) performed a successful surgical management on a patient with left ventricular aneurysm accompanying acute myocarditis[8]. Considering the size of the diverticulum and the risk of rupture, our patient underwent surgical management. Unfortunately, the exacerbated cardiac function during the two-year follow-up period after surgery implied that conventional surgical procedures might not be suitable for our patient during the period of acute myocarditis, except for heart transplant.