



1. Background
2. Objectives
3. Patients and Methods
3.1. General Data
3.2. X-ray Examination of Breast Tissue
3.3. MRI Examination of Breast Tissue
3.4. Imaging Analysis
3.5. Pathological Diagnosis
3.6. Statistical Analysis
4. Results
4.1. Clinical Data
| Benign and malignant breast lesions | Histopathological type | N |
|---|---|---|
| Benign lesions | Breast fibroadenoma | 58 |
| Adenosis | 28 | |
| Cystic hyperplasia of the breast | 12 | |
| Mammary tuberculosis | 2 | |
| Intraductal papilloma of the breast | 5 | |
| Malignant lesions | Invasive ductal carcinoma of the breast | 83 |
| Invasive lobular carcinoma of the breast | 7 | |
| Ductal carcinoma in situ of the breast | 8 | |
| Mucinous adenocarcinoma of the breast | 5 | |
| Premalignant breast lesions | 2 |
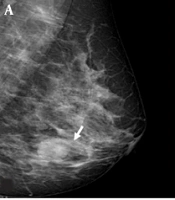
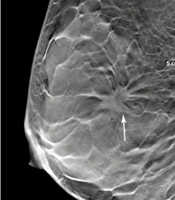
 diagnosed as stage II invasive ductal carcinoma. A, The DBT image of the largest layer indicates burrs on the edges of the mass (arrow). B, Fat-suppression T1-weighted MRI image (arrow). C, FFDM image showing overlaps between the mass edges and the mammary gland (arrow). ACR, American College of Radiology; DBT, digital breast tomosynthesis; FFDM, full-field digital mammography; MRI, magnetic resonance imaging.")
The imaging results of a 45-year-old female patient with a dense, uneven tumor (ACRc) diagnosed as stage II invasive ductal carcinoma. A, The DBT image of the largest layer indicates burrs on the edges of the mass (arrow). B, Fat-suppression T1-weighted MRI image (arrow). C, FFDM image showing overlaps between the mass edges and the mammary gland (arrow). ACR, American College of Radiology; DBT, digital breast tomosynthesis; FFDM, full-field digital mammography; MRI, magnetic resonance imaging.
4.2. Imaging and Pathological Results of Examination Methods
| Methods | Sensitivity | Specificity | Accuracy | Positive predictive value | Negative predictive value | Youden's index | AUC (95% CI) |
|---|---|---|---|---|---|---|---|
| FFDM | 82.86 (87/105) | 76.19 (80/105) | 78.57 (165/210) | 75.00 (87/116) | 82.98 (78/94) | 51.83 | 0.734 (0.723-0.845) |
| DBT | 90.48 (95/105) | 88.57 (93/105) | 89.05 (187/210) | 86.36 (95/110) | 91.00 (91/100) | 72.18 | 0.857 (0.794-0.873) |
| FFDM + DBT | 92.38 (97/105) | 90.48 (95/105) | 90.95 (191/210) | 88.18 (97/110) | 93.00 (93/100) | 76.45 | 0.865 (0.801-0.881) |
| MRI | 100.00 (105/105) | 80.95 (85/105) | 91.90 (193/210) | 82.68 (105/127) | 100.00 (83/83) | 77.94 | 0.883 (0.846-0.912) |
| FFDM + MRI | 100.00 (105/105) | 86.67 (91/105) | 95.24 (200/210) | 87.50 (105/120) | 100.00 (90/90) | 83.45 | 0.924 (0.876-0.986) |
Abbreviations: AUC, area under curve; CI, confidence interval; DBT, digital breast tomosynthesis; FFDM: full-field digital mammography; MRI, magnetic resonance imaging.
4.3. Diagnostic Efficiencies of Five Examination Methods for Breast Cancer
.")
The results of the ROC curve analysis for the diagnostic efficiency of five examination methods for breast cancer (ROC: receiver operating characteristic curve).