1. Background
Abdominopelvic fluid collection and abscess management and the outcomes have improved in the recent years due to innovation of the image-guided drainage technique and improvement of surgical procedures (1). Percutaneous drainage (PCD) of abdominopelvic abscess or fluid collection has become an alternative for surgery in the treatment of abdominal abscess. Itallows effective drainage with minimal trauma to the tissues and lower morbidity and mortality rates (1-5). PCD also acts as a temporary route in situations like appendicular abscess for drainage before necessary following surgery (6).
The procedure is guided by ultrasonography or CT scan. US provides real-time imaging and it is the method of choice in the relatively superficial and unilocular abscesses, where there is little risk of transgressing a vascular structure, bowel, or pleural cavity. CT is the method of choice when US guidance does not seem safe enough (2, 3). CT fluoroscopy can facilitate percutaneous drainage and can reduce the time of the procedure (7). This technique is safe, rapid and accurate (8). CT-guided drainage may be used for abscess and collections with various causes such as Crohn’s disease (9, 10), perforated appendicitis, trauma, post-operative, hematoma, infected pancreatic pseudocyst, lymphocele and urinoma(4, 6, 11).
Undrained abdominopelvic abscess has a high mortality rate between 45 and100% (2, 12) that can be reduced by PCD (3). Relief of patient symptoms and signs including abdominal pain, distension, and fever, improvement in laboratory tests and follow-up imaging findings are indicators of successful drainage (3).
2. Objectives
In order to assess the efficacy and complications of this nonoperative percutaneous drainage technique, the authors have reported their experience in the management of abdominal abscess by PCD procedure.
3. Patients and Methods
The medical records of all patients with abdominopelvic abscess or fluid collection,who were referred to our hospital and had undergone PCD between November 2006 and April 2008, were studied. The details of 47 patients,who had routine preoperative evaluations including cell blood count, urine analysis and culture, renal function and coagulation tests, were available. The patients without a completed six-month follow-up were excluded. Forty one cases were included in the study for data analysis.
To assess the size, location and properties of the abscess, and also the anatomy of adjacent organs,the patients were assessed by abdominopelvic CT scan with IV and oral contrast before performing the procedures. The size of the abscess was defined as the largest diameter reported on CT exam. Information such as demographic data including the patient’s age and gender as well as the size and location of the abscesswere recorded. The ethics committee of Shahid Beheshti University of Medical Sciences approved the study protocol, and informed consents were obtained from all cases. Treatment with broad-spectrum intravenous antibiotics was started immediately. Intravenous sedation with local anesthesia was performed for patients to drain the abscess.
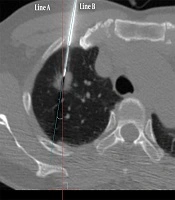
All the procedures were performed by a single experienced radiologist under CT guidance. First, a gauge-18 access needle was passed into the abscess to obtain a specimen for culture and Gram stain. After achieving the puncture, a 0.035-inch J tipped guide wire was introduced and coiled into the targeted abscess cavity. After tract dilatation, the 8-to 12-French pigtail drainage catheter (Gallini; Italy) was positioned under CT guidance. The cavity content was aspirated and rinsed with sterile normal saline and the catheter was fixed to the skin. All specimens taken from the abscess cavity were sent for biochemical analysis and culture for aerobic and anaerobic organisms. The pigtail was withdrawn when drainage was discontinued for two days.
Improvement was assessed based on absence of sepsis due to collection, loss of fever, loss of collection size or shrinkage of the abscess wall by follow-up ultrasonography or CT scan. Success rate (rate of treatment), hospital stay and the complications were collected. Data analysis was performed by SPSS software for Windows Ver 15 (SPSS Inc, Chicago, IL, USA). The data are presented as mean ± SD (minimum and maximum) for quantitative variables, and the number of observations, frequencies and percentage for qualitative variables.
4. Results
Forty-one patients were included in the study with at least a follow-up of 6 months and their data were analyzed. The average patient age was 54.4 years (12-79) including 21 (51%) men and 20 (49%) women. The common signs and symptoms were pain (83%), followed by fever (80.5%), chills and perspiration (56%). Liver was the most frequent site of abscess location with 17 (41.5%) cases. Previous surgery was the most prevalent etiology for abdominal abscess in 31 cases (75.6%). The diameter of the abscessranged between 5 and 12 (mean, 7.8) cm. Demographic and clinical characteristics of the patients are shown in Table 1.
As shown in Table 2, the most common pathogens obtained from culture media were E. coli (22%) followed by Pseudomonas (14.6%). However, no pathogen grew in nearly half of the specimens.
The average hospital stay was 8 (4-15) days. Thirty-five cases (86%) were successfully treated and six patients needed secondary drainage.
Complications developed in only one patient as peritonitis, who was conservatively managed with antibiotics and close monitoring.
Table 1.
Demographic and Clinical Characteristics of the Patients
| No. (%) | |
|---|---|
| Gender | |
| Male | 21 (51) |
| Female | 20(49) |
| Symptoms and Signs | |
| Abdominal pain | 34 (83) |
| Fever | 33 (80.5) |
| Chills and perspiration | 23 (56) |
| Nausea and vomiting | 20 (48.8) |
| Weight loss | 15 (36.5) |
| Loss of appetite | 12 (29.2) |
| Chest manifestations | 8 (19.5) |
| Jaundice | 6 (14.6) |
| Diarrhea | 5 (12.2) |
| Abscess Location | |
| Liver | 17 (41.5) |
| Spleen | 3 (7) |
| Pancreas | 2 (5) |
| Subdiaphragmatic/subhepatic | 4 (10) |
| Renal/perirenal | 4 (10) |
| Peri-transplant kidney | 3 (7) |
| Appendiceal region | 3 (7) |
| Psoas | 2 (5) |
| Abdominal wall | 1 (2.5) |
| Paravertebral | 1 (2.5) |
| Etiology | |
| Idiopathic | 4 (10) |
| Post operation | 31 (75.5) |
| Pancreatitis | 2 (5) |
| Crohn's disease | 1 (2.5) |
| Trauma | 2 (2.5) |
| Pott's disease(TB) | 0 (0) |
Table 2.
Culture Results, Complications and Success Rates
| Pathogens | No. (%) |
|---|---|
| E. coli | 9 (22) |
| Klebsiella | 3 (7) |
| Staphylococcus | 2 (5) |
| Streptococcus | 1 (2.5) |
| Proteus | 1 (2.5) |
| Pseudomonas | 6 (14.6) |
| Enterobacteria | 1 (2.5) |
| Acinetobacterbaumannii | 1 (2.5) |
| Anaerobics | 0 (0) |
| Multiple Organisms | 0 (0) |
| Amoeboid Abscess | 0 (0) |
| Negative culture | 17 (41.5) |
| Complications | |
| Total | 1 (2.5) |
| Wound infection | 0 (0) |
| Hematoma | 0 (0) |
| Peritonitis | 1 (2.5) |
| Fistula | 0 (0) |
| Empyema | 0 (0) |
| Success rate | 35 (86) |
5. Discussion
The development of improved imaging modalities together with broad-spectrum antibiotics and new drainage catheters has established PCD as the standard therapy for abdominal and pelvic abscess in the absence of indications for immediate surgery (1-5). PCD or aspiration could be performed potentially in every organ. The contraindications are relatively few. The main ones are uncorrectable coagulopathy, lack of safe percutaneous access, and inability of the patient to cooperate. In practice, the absence of a safe route is the only factor that inhibits percutaneous drainage. On the other hand, there is a spectrum of procedure complexity that influences outcomes in percutaneous procedures; for example, multiple or multiloculated abscesses, abscess due to Crohn’s disease, pancreatic abscesses, a drainage route that traverses the bowel or pleura, an infected clot, and infected tumor (2, 10, 13, 14). One should expect that percutaneous drainage in such cases will have a lower chance of success, be more technically difficult, require longer periods of time for drainage, and have a higher rate of complications. We performed a retrospective study on patients who underwent PCD for abscess or abdominal fluid collection and were followed up for 6 months. PCD was performed under CT guidance because of the local staff expertise and its better resolution and safety.
This study revealed that successful treatment was achieved in 86% of the cases. It is in concordance with most of the previous reports (15-18). Of all specimen cultures, 17 (41.5%) did not show growth that may have been false, in part due to technical problems. Inappropriate temperature of the drainage site or culture room, delay in transmission of the specimen, or delay in culture may be the underlying causes.
The complication rate was 2.5% (one patient with secondary peritonitis). In older reports, a complication rate of 4-29% has been reported for PCD(16, 17), which is reduced in recent studies. Laopaiboon et al. (18) reported no complication for PCD. This finding could be attributed to interventional technique improvement during the last two decades.
The limitation of this study is that data of the internal characteristic of the abscess such as internal septa or gas formation were not mentioned in the medical records in most of the cases and therefore, could not be utilized, since recent studies have suggested that gas formation within the abscess might be an important predictor for PCD failure (15).
In concordance with previous studies, we showed that PCD is a safe and effective procedure for the treatment of abdominal abscess and fluid collections.
Reference