





.jpg)


1. Background
Intrauterine growth restriction (IUGR) occurs in 5 - 10% of all pregnancies (1). It is defined as a birth weight below the 10th percentile for gestational age and is mostly caused by placental insufficiency (2, 3). Multiple pathophysiological mechanisms occur during IUGR due to placental dysfunction (4). Following placental insufficiency, the transfer of oxygen and nutrients to the fetus is reduced, and the blood flow selectively redistributes to vital organs, including the brain, while the blood flow to other fetal organs is decreased (2). These hemodynamic changes cause recurrent hypoxemia episodes (4). Evidence shows the adverse effects of hypoxia on brain development, brain cell count, brain volume reduction, and consequently, whole brain weight loss (5). Doppler ultrasound is used in high-risk pregnancies for detecting the severity of hypoxia (6).
IUGR is a major factor in long-term perinatal morbidity and is associated with abnormal fetal brain development, cerebral palsy, mental retardation, neurological and motor skill disorders, and cognitive disorders (7). These neurodevelopmental problems are correlated with certain neurostructural changes in the brain (8), which are seen in both severe and mild IUGR (9). There is a major challenge in the perinatal diagnosis of brain injuries in IUGR pregnancies (10). The use of magnetic resonance imaging (MRI) has recently increased the possibility of determining structural and morphometric differences in the brain structure of IUGR and appropriate for gestational age (AGA) fetuses (1, 2). According to previous research, the patterns of brain abnormalities associated with IUGR remain unknown (11, 12).
Cortical development is a complex process, affected by many factors (9). The MRI of IUGR fetuses shows significant differences in the brain volume and cortical characteristics, such as the gyrification pattern and cortical thickness (8, 13, 14). Some studies have reported brain grey matter volume reduction, especially in the temporal and insular lobes (15).
2. Objectives
There are few studies measuring the brain cortical thickness and area in IUGR fetuses. This study aimed to evaluate the effect of growth restriction on the cortical thickness and brain area of fetuses compared to the controls by 3-tesla MRI.
3. Patients and Methods
3.1. Patient Population
In this study, we prospectively examined a sample of 42 women with IUGR pregnancies and 28 normal fetuses in the control group at a gestational age of 28 - 38 weeks. This study was performed in the imaging department of hospitals between March 2017 and January 2019. Written informed consent was obtained from all participants, and the study was approved by the institutional board members and the ethics committee. Gestational age was measured based on the first-trimester crown-rump length in all fetuses. Fetal weight was also assessed by ultrasound during the same week as fetal MRI. IUGR was defined as fetal weight less than the 10th percentile for gestational age, based on ultrasound and the reference data (16).
The control group was selected among fetuses with fetal and postnatal weights ≥ 10th percentile at a similar gestational age to the IUGR group; they were referred for MRI of the extra-central nervous system (CNS) pathologies. Maternal demographic and perinatal data, including gestational biometric parameters and weight at the time of MRI, birth weight, and pregnancy outcomes after birth, were recorded in the study groups. The MRI exclusion criteria were the presence of congenital infection, multiple pregnancies, chromosomal abnormalities, suspected genetic syndromes, chronic maternal diseases, general contraindications for MRI, and any structural or brain abnormalities detected on MRI.
Because of fetal calvarium shadowing, ultrasound is not a suitable tool for the evaluation of brain lobes. Also, ultrasound does not provide high-resolution images of soft tissues for differentiating the cortex from the white matter. Therefore, in this study, we aimed to assess the brain characteristics of fetuses via fetal MRI. According to the American College of Rheumatology (ACR) guidelines, exposure to 3T magnetic fields, used in routine clinical MRI, does not have any reproducible adverse effects on the developing fetus. Also, in this study, we tried to decrease fetal exposure by using rapid acquisition sequences and decreasing the acquisition time (17).
3.2. Doppler Ultrasound
An ultrasound examination was carried out using a transabdominal 2 - 6 MHz curved-array transducer (Philips Affiniti 50 General Imaging configuration, USA) in the same week as the MRI session. The fetal umbilical artery (UA) and middle cerebral artery (MCA) pulsatility index (PI) were assessed, and values above the 95th percentile and below the 5th percentile were considered abnormal, respectively, according to the reference chart (18). An abnormal cerebroplacental ratio (CPR) was defined as a CPR below the 5th percentile. The mean PI of bilateral uterine artery (UtA) was measured by transabdominal sonography; values were considered abnormal if they were above the 95th percentile (19). The IUGR cases, depending on the IUGR severity, were subcategorized into two study groups: (1) group A, with severity signs, such as fetal weight less than the 3rd percentile, and/or abnormal UA or UtA PI, and/or abnormal CPR; and (2) group B, without the abovementioned criteria.
3.3. MRI Protocol
Fetal brain MRI was carried out using a 3T MRI system (discovery 750 GEM, GE healthcare, USA), using a 16-channel phased-array coil. Brain MRI was performed during the same week as IUGR diagnosis by ultrasound. Imaging was performed after four hours of fasting without sedation, while the patient was positioned in the left lateral decubitus. The duration of brain MRI was almost 20 - 30 minutes for each case. The examination protocol applied to study the patients included the single shot fast spin echo (SSFSE) T2-weighted sequences with a slice thickness of 4 mm with no gap, a field of view (FOV) of 25 - 27 cm, repetition time of 1500 ms, echo time of 98 ms, matrix size of 288 × 192 mm, flip angle of 180°, and acquisition time of 25 sec. Brain MRI was taken at three different orthogonal planes. If any motion artifact degradation was detected, the sequence was repeated until a satisfactory image was obtained.
3.4. MRI Analysis
An offline analysis of all morphological and biometric brain measurements was performed on the Infinite Picture Archiving and Communication System (PACS) by an experienced specialist. The radiologist was informed about the preliminary diagnosis of IUGR, but not the subgroups. Brain biometric parameters [biparietal diameter (BPD) and head circumference (HC)] were measured in the transthalamic axial plane and assessed based on the standard reference chart (16). The brain cortical thickness was determined based on the following approach (Figure 1):
- Insular cortex thickness: In the axial plane, right below the cavum septum pellucidum plane.
- Frontal cortex and occipital cortex thickness: In the axial plane, at the level of the cavum septum pellucidum.
- Temporal cortex thickness: In the coronal plane, anterior to the pons level.
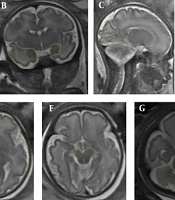
 show the brain cortical thickness assessment. A, Frontal and occipital lobe cortical thickness measurements (in the axial plane, at the level of the cavum septum pellucidum); B, Insular cortical thickness measurements (in the axial plane, right below the plane of the cavum septum pellucidum); C, Temporal lobe cortical thickness measurement (in the coronal plane, just anterior cut to the pons level). The two parts were measured from the inner side to the outer side.")
T2-weighted magnetic resonance images (MRI) show the brain cortical thickness assessment. A, Frontal and occipital lobe cortical thickness measurements (in the axial plane, at the level of the cavum septum pellucidum); B, Insular cortical thickness measurements (in the axial plane, right below the plane of the cavum septum pellucidum); C, Temporal lobe cortical thickness measurement (in the coronal plane, just anterior cut to the pons level). The two parts were measured from the inner side to the outer side.
In each region, measurements were carried out in two parts from the inner side to the outer side. We calculated the average of bilateral cortical thickness for each region and then corrected it by dividing it by BPD/2. The brain area was determined in the following regions (Figure 2):
- Occipital lobe area: In the first para-sagittal plane, near the falx, posterior to the parieto-occipital sulcus.
- Temporal lobe area: In the coronal plane, anterior to the pons level.
- Frontal lobe area: In the axial plane, right above the cavum septum pellucidum and lateral ventricles, anterior to the Rolandic fissure.
- Parietal lobe area: In the axial plane, right above the cavum septum pellucidum and lateral ventricles, posterior to the Rolandic fissure.
- Cerebellum: In the axial plane, at the level of the middle cerebellar peduncle.
- Pons: At the same level described for the cerebellum.
- Midbrain: In the axial plane, at the level of the midbrain.
- Whole brain surface area (WBA): In the axial plane, at the level of the cavum septum pellucidum.
- Whole intracranial area: At the same level of WBA by tracing the cursor inside the bony calvarium.
 demonstrate different brain lobe areas. A, Frontal and parietal lobe areas (in the axial plane, right above the cavum septum pellucidum and lateral ventricles); B, Temporal lobe and hippocampus areas (in the coronal plane, right anterior to the pons level); C, Occipital lobe area (in the first para-sagittal plane, near the falx, posterior to the parieto-occipital sulcus); D, Whole brain area (WBA) (in the axial plane, at the level of the cavum septum pellucidum); E, Whole intracranial area (at the same level of WBA by tracing the cursor inside the bony calvarium); F, Midbrain area; G, Cerebellum and pons areas (in the axial plane, at the level of the middle cerebellar peduncle).")
T2-weighted magnetic resonance images (MRI) demonstrate different brain lobe areas. A, Frontal and parietal lobe areas (in the axial plane, right above the cavum septum pellucidum and lateral ventricles); B, Temporal lobe and hippocampus areas (in the coronal plane, right anterior to the pons level); C, Occipital lobe area (in the first para-sagittal plane, near the falx, posterior to the parieto-occipital sulcus); D, Whole brain area (WBA) (in the axial plane, at the level of the cavum septum pellucidum); E, Whole intracranial area (at the same level of WBA by tracing the cursor inside the bony calvarium); F, Midbrain area; G, Cerebellum and pons areas (in the axial plane, at the level of the middle cerebellar peduncle).
We attempted to acquire standard, motionless images, while removing oblique images. All measurements were performed twice and delineated by a cursor-guided free-hand trace; the mean of each measurement was used for the analysis. Next, the mean of bilateral area for each region was calculated. The corrected brain area was determined by dividing each brain area by WBA; the corrected WBA was calculated by dividing WBA by the whole intracranial area.
3.5. Data Analysis
SPSS version 22 (IBM Corp., Armonk, NY, USA) was used for statistical analysis. Data are summarized using mean and standard deviation (SD) for quantitative variables and using frequency and percentage for qualitative variables. For data analysis, first, the normal distribution of quantitative data was investigated using Kolmogorov-Smirnov test (K-S test). Comparison between the groups was made using Fisher’s exact test, chi-square test, and t-test. P-values less than 0.05 were considered statistically significant.
4. Results
4.1. Demographics and Clinical Indicators
A total of 42 fetuses with IUGR were included in the IUGR group, and 28 fetuses with a similar gestational age (around 28 - 38 weeks) were included in the control group. The mean GA was 34 + 1 weeks in the IUGR group and 34 weeks in the control group (P = 0.98). The IUGR group included 24 fetuses with IUGR subtype A and 18 fetuses with IUGR subtype B. The maternal and fetal characteristics, as well as perinatal outcomes of the study groups, are presented in Table 1. Only one death (stillbirth) in subtype A was reported. The UA PI > 95th percentile, MCA PI < 5th percentile, and UtA PI > 95th percentile were detected in 11 (45%), 4 (16.6%), and 5 (21%) fetuses with subtype A IUGR, respectively. Absent or reversed diastolic flow in an umbilical artery or abnormal flow in the ductus venosus was not found in any of the IUGR subgroups (no case of severe hypoxia).
| Variables | IUGR subtype A (n = 24) | IUGR subtype B (n = 18) | P-value | IUGR (n = 42) | Control group (n = 28) | P-value |
|---|---|---|---|---|---|---|
| Maternal characteristics | ||||||
| Age (y) | 29.33 ± 5.53 | 30.39 ± 4.94 | 0.593 | 29.79 ± 5.25 | 29.81 ± 2.67 | 0.792 |
| Height (cm) | 162.04 ± 5.57 | 161.28 ± 4.35 | 0.768 | 161.71 ± 5.04 | 157.64 ± 14.63 | 0.470 |
| Weight (kg) | 77.37 ± 15.09 | 77 ± 12.20 | 0.932 | 77.21 ± 13.77 | 73.43 ± 12.52 | 0.247 |
| BMI (kg/m2) | 29.44 ± 5.47 | 29.63 ± 4.75 | 0.903 | 29.52 ± 5.11 | 28.15 ± 4.41 | 0.250 |
| Preeclampsia | 4 (16.7) | 1 (5.6) | 0.02 | 5 (11.9) | 0 (0) | 0.001 |
| Fetal characteristics | ||||||
| Age (weeks) | 33 + 6 | 34 + 1 | 0.690 | 34 + 1 | 34 | 0.98 |
| Weight (g) | 1704.83 ± 487.7 | 1829.1 ± 562.8 | 0.448 | 1758 ± 517.8 | 1954 ± 662 | 0.157 |
| Sex (female) | 12 (50) | 10 (55.6) | 0.721 | 22 (52.4) | 6 (21.4) | 0.010 |
| HC < 5% | 13 (54.2) | 4 (22.2) | 0.0002 | 17 (40) | 0 (0) | < 0.0001 |
| Perinatal outcomes | ||||||
| Birth weight (g) | 2194.76 ± 544.98 | 2616.3 ± 363.4 | 0.011 | 2377. ± 514.6 | 2965.7 ± 733.13 | < 0.0001 |
| GA at birth (weeks) | 36 + 6 | 37 + 2 | 0.330 | 37 + 1 | 37 + 2 | 0.978 |
| NICU admission | 8 (38.1) | 3 (18.8) | 0.012 | 11 (29.7) | 8 (28.6) | 0.89 |
| Intrauterine stillbirth | 1 (5) | 0 (0) | 1 | 1 (2.9) | 0 (0) | 1 |
Maternal and Fetal Characteristics and Perinatal Outcomes of the Study Groups a
4.2. MRI Examination
The brain white and grey matter signal and morphology were normal in all fetuses, and no obvious hypoxic ischemic events as hemorrhagic changes were detected. The corrected cortical thickness in the insula and temporal lobe was significantly lower in the IUGR group in comparison with the control group (0.034 vs. 0.043 and 0.036 vs. 0.047, respectively; P < 0.05) (Figure 3). However, there was no significant difference in the cortical thickness of frontal and occipital lobes (Table 2). The insular, frontal, and occipital corrected cortical thicknesses were lower in IUGR subtype A as compared to subtype B; however, the difference was not significant (Table 3).
 and control groups. The bars show mean ± SD for each group, and asterisks indicate P < 0.05.")
The polynomial contrast analysis demonstrates a difference in the corrected cortical thickness of different brain regions between the Intrauterine growth restriction (IUGR) and control groups. The bars show mean ± SD for each group, and asterisks indicate P < 0.05.
| Variables | IUGR group (n = 42) | Control group (n = 28) | P-value |
|---|---|---|---|
| Cortical thickness (mm) | |||
| Insula | 0.034 ± 0.007 | 0.043 ± 0.012 | 0.001 |
| Frontal lobe | 0.031 ± 0.005 | 0.033 ± 0.013 | 1 |
| Occipital lobe | 0.031 ± 0.007 | 0.034 ± 0.013 | 0.250 |
| Temporal lobe | 0.036 ± 0.007 | 0.047 ± 0.027 | 0.010 |
| Area (cm2) | |||
| Frontal lobe | 0.214 ± 0.028 | 0.209 ± 0.029 | 0.374 |
| Temporal lobe | 0.086 ± 0.024 | 0.086 ± 0.022 | 0.611 |
| Occipital lobe | 0.105 ± 0.024 | 0.100 ± 0.016 | 0.274 |
| Hippocampus | 0.017 ± 0.008 | 0.0125 ± 0.003 | < 0.001 |
| Cerebellum | 0.147 ± 0.021 | 0.130 ± 0.019 | 0.001 |
| Midbrain | 0.043 ± 0.015 | 0.043 ± 0.007 | 0.983 |
| Pons | 0.031 ± 0.014 | 0.028 ± 0.003 | 1 |
| WBA | 0.806 ± 0.170 | 0.812 ± 0.027 | 0.028 |
The Corrected Brain Area and Corrected Cortical Thickness in the IUGR and Control Groups
| Variables | IUGR subtype A (n = 24) | IUGR subtype B (n = 18) | P-value |
|---|---|---|---|
| Cortical thickness (mm) | |||
| Insula | 0.032 ± 0.005 | 0.036 ± 0.009 | 0.104 |
| Frontal lobe | 0.029 ± 0.003 | 0.032 ± 0.007 | 0.104 |
| Occipital lobe | 0.030 ± 0.006 | 0.032 ± 0.007 | 0.562 |
| Temporal lobe | 0.037 ± 0.006 | 0.036 ± 0.007 | 0.415 |
| Area (cm2) | |||
| Frontal lobe | 0.208 ± 0.029 | 0.222 ± 0.024 | 0.169 |
| Temporal lobe | 0.085 ± 0.015 | 0.088 ± 0.034 | 0.668 |
| Occipital lobe | 0.105 ± 0.021 | 0.105 ± 0.028 | 0.627 |
| Hippocampus | 0.015 ± 0.003 | 0.019 ± 0.012 | 0.334 |
| Cerebellum | 0.146 ± 0.022 | 0.148 ± 0.019 | 0.791 |
| Midbrain | 0.045 ± 0.019 | 0.041 ± 0.007 | 0.368 |
| Pons | 0.028 ± 0.011 | 0.034 ± 0.017 | 0.44 |
| WBA | 0.785 ± 0.220 | 0.831 ± 0.049 | 0.566 |
Differences in the Corrected Brain Area and Corrected Cortical Thickness in IUGR Subtype A and Subtype B
The IUGR fetuses had significantly smaller corrected WBA (0.806 vs. 0.812; P = 0.028). The corrected area of the cerebellum and the hippocampus was smaller in normally grown fetuses (0.130 vs. 0.147 and 0.0125 vs. 0.017, respectively; P < 0.05) (Figure 4); however, other corrected areas of the brain were not significantly different between the IUGR and control groups (Table 2). The corrected area of the frontal lobe, temporal lobe, cerebellum, and hippocampus in subtype A was smaller than subtype B, but the difference was not significant (Table 3).
 and control groups. The bars show mean ± SD for each group, and asterisks represent P < 0.05.")
The polynomial contrast analysis demonstrates a difference in the corrected brain areas in different lobes between the Intrauterine growth restriction (IUGR) and control groups. The bars show mean ± SD for each group, and asterisks represent P < 0.05.
5. Discussion
The present results demonstrated that the corrected cortical thickness in the insula and temporal lobes was significantly thinner in the IUGR fetuses as compared to the control group. Also, WBA was significantly smaller in the IUGR group. The corrected areas of the cerebellum and the hippocampus were smaller in the controls. Several studies have suggested that IUGR, due to placental insufficiency, is associated with specific structural and functional changes in the cortical development of the brain (5, 9). The IUGR neonates show delayed cortical development at birth, as well as brain cortical thickness and volume reduction (3, 20).
The insula is an important part of the limbic system, with a major role in cognition and awareness (20). In the present study, the corrected cortical thickness of the insula was thinner in IUGR fetuses as compared to the control group. These results are compatible with the findings reported by Egana‐Ugrinovic et al., which showed that IUGR fetuses had a reduced insular cortical thickness compared to the controls. A possible mechanism is that this area is vulnerable to long-term hypoxia (8). Moreover, our IUGR group had a significantly thinner corrected temporal cortical thickness. Our results are consistent with another study, which showed reduced gray matter volume in the bilateral temporal lobe in IUGR fetuses compared to the controls (14). However, further research is needed to have a better understanding of the effects of growth restriction on the temporal cortical thickness.
There is no published study comparing different lobe areas in IUGR fetuses comprehensively. Since volume measurement in routine clinical practice is more time-consuming, and we aimed to find a less time-consuming and simple method for routine practice, we measured different brain areas in this study. On the other hand, we were aware that assessing the whole volume of a lobe or structure (such as the hippocampus) using the routine formula (Cavalieri’s principle) (9) is not as accurate as tracing one free region of interest (ROI) for a brain structure in a fixed and defined plane. Regarding the brain areas, our results showed that the WBA in the IUGR group was significantly lower than the controls, which is compatible with previous studies (5, 9, 15, 21). These differences may be due to the effect of placental insufficiency on DNA synthesis or reduction of brain cell size and count, synaptogenesis, and total brain weight (22, 23). In contrast to the mentioned studies, only one study found no significant difference in the whole brain volume between the IUGR and normal fetuses (24).
It is worth mentioning that in this study, the corrected area of the cerebellum was larger in the IUGR group as compared to the controls. We assessed the corrected area of the cerebellum by dividing the cerebellar area by WBA; the WBA was smaller in the IUGR group. This finding may show that the cerebellum is less affected by IUGR compared to other brain regions. Our results are almost consistent with a study by Sanz-Cortes et al., which assessed the corrected cerebellar volume by dividing the cerebellar volume by the whole brain volume. They showed a significantly larger cerebellar ratio in the IUGR fetuses (25).
Moreover, Bruno et al. showed that there was no significant difference in the cerebellar volume between the IUGR and control groups (26). Research using ultrasound has also shown the preservation of transcerebellar diameter in IUGR fetuses (27). All of the mentioned studies have emphasized the preservation of cerebellar size in IUGR fetuses. However, a study by Polat et al. found a decreased cerebellar/supratentorial volume ratio in IUGR fetuses (28), and Anderscavage et al. demonstrated a smaller cerebellar volume in IUGR fetuses (29). Due to inconsistent results, further research is needed to evaluate the growth restriction effect on the fetal cerebellum.
Hippocampus is an important grey matter structure, sensitive to placental insufficiency, hypoxia, lower nutritional supply, and maternal stress (30-32). An animal study showed the adverse molecular and cellular effects of IUGR on the hippocampus structure (33). In our study, the IUGR fetuses had a significantly larger corrected hippocampus area; similar to the cerebellar area, this region may be less affected by IUGR. Moreover, Padilla et al. studied neonatal IUGR and AGA groups and found no significant difference in the hippocampus volume between these groups (15). On the contrary, Lodygensky et al. suggested that the total hippocampal volume was affected by IUGR; they reported a significantly smaller hippocampus volume in IUGR fetuses as compared to the controls (7).
The present study showed no significant difference in the frontal and occipital corrected areas between the IUGR and control groups. Although there is no study evaluating different brain lobe areas, our findings are in line with a study by Padilla et al., which demonstrated similar frontal and occipital relative volumes in the IUGR fetuses and controls (15). Some studies on older subjects also showed smaller frontal lobe volumes in the IUGR group; the difference in the relative frontal lobe volume may be no longer observable up to one year of age (15). On the other hand, a study using sonographic biometry showed decreased frontal lobe dimensions in IUGR neonates as compared to the controls (34). It was found that the frontal lobe might have a delayed growth pattern in IUGR (33). Based on these findings, the preservation of the frontal lobe area in IUGR fetuses in our study might be due to the developmental process of the frontal lobe and the lower gestational age during assessment.
Although some parameters in the IUGR group (such as pons area) were slightly higher than the control group, the difference was not significant. Also, slightly higher values in group B underrated the slightly lower values in group A. This can be related to the fact that these fetuses with normal Doppler results and moderately decreased weight are small, but not really growth restricted. Also, some discrepancies may be due to the fact that our control group was selected among cases referred for non-CNS pathologies and were not completely normal.
This study had some limitations. First, the sample size was relatively small, especially for comparing slight differences between the IUGR subtypes. Second, we manually traced all brain areas, which could be subject to inter- or intra-reader variability. Third, the number of IUGR fetuses and the controls was not similar. Many non-IUGR cases referred for fetal MRI to our center had a lower gestational age than the IUGR cases. Therefore, for matching the gestational age of the two groups, we faced limitations in including the control fetuses. Finally, because our control group was selected among fetuses with other pathologies, the postnatal outcomes were not significantly different between the IUGR and control groups.
In conclusion, our findings showed that IUGR has selective effects on the brain morphometrics. The IUGR fetuses have a thinner cortical thickness in the insular and temporal lobes and smaller whole brain areas. Also, the cerebellum and hippocampus are less affected by growth restriction. Further detailed investigations are needed in the future to evaluate the morphometric effects of IUGR on the insula, cerebellum, hippocampus, and temporal lobe and to evaluate their association with neurological outcomes.
