



1. Background
The orbit is a cone-shaped structure in the midline of the face, which resembles a pyramid and surrounds the organs of vision. It is a cavity with its apex located posteriorly and its base situated anteriorly, containing projections for the attachment of muscles and ligaments. The orbit contains extraocular muscles, adipose tissue, and many important neurovascular structures. It is also closely associated with the anterior cranial fossa, middle cranial fossa, and paranasal sinuses (1). There are holes and slits in the apex of the orbit through which nerves and vessels pass (2). The optic nerve reaches the orbit by passing through the optic foramen and the annulus of Zinn (3). Because of this relationship, a disease in the orbit can spread to the sinus and intracranial regions, and vice versa. To understand the effects of different diseases on the orbit and neighboring structures, it is necessary to have adequate knowledge of the anatomy of the orbit and its surrounding structures and determine their relationships with each other; this is also of great significance for performing a safe orbital surgery (1).
Orbital decompression is performed to reduce intraorbital pressure by removing the fat tissue and bone around the orbit. In this surgical procedure, pressure on the optic nerve is minimized by increasing the orbit volume (4). There are four main techniques for orbital decompression, including transorbital, transcranial, transantral, and transnasal techniques (5). The transnasal technique is being used more frequently for orbital decompression due to the development of endoscopy technologies and improvement of endoscopic instruments. Generally, proper equipment, experienced personnel, and adequate anatomical knowledge are required to perform this procedure (6). Ethmoiditis with orbital complications and ethmoidal mucoceles, Graves' orbitopathy, exophthalmos, diplopia, optic neuropathy, advanced proptosis, orbital hemorrhage, and orbital tumors are indications for orbital decompression (6-9). To achieve maximum decompression, surgeons need to open the orbit up to the apex, including the optic foramen and the annulus of Zinn (3).
2. Objectives
This study aimed to determine the position of the sphenoid sinus relative to the optic foramen based on computed tomography (CT) scan, which is necessary for orbital decompression surgery, in the Central Anatolia Region. Unlike previous studies on this subject, we found that the foramen opticum is more often located anteriorly than the anterior aspect of the sinus sphenoidalis.
3. Patients and Methods
This study was carried out in Niğde Ömer Halisdemir Medical Faculty Hospital (Niğde, Central Anatolia, Turkey). All procedures adhered to the tenets of the Declaration of Helsinki, and ethical approval was obtained from the Ethics Committee of Niğde Ömer Halisdemir University (protocol number: 2021/39). All eligible CT scans, acquired in our hospital between March 15 and April 15, 2021, were included in this study.
In this cross-sectional study, a total of 64 patients from the Turkish population of Central Anatolia were included. The patients were selected by purposive sampling method. The cranial CT images of 64 patients (128 orbits) were evaluated retrospectively using the hospital's picture archiving and communication system (PACS). Cranial CT images were obtained using a Somatom Sensation 64 CT scanner (Siemens Medical Solutions, Erlangen, Germany) available in the hospital. Patients included in this study were admitted to the hospital with headache, while their CT images, which were evaluated by an experienced radiologist, were reported as normal. Patients over the age of 18 years with normal CT images were included in the study. On the other hand, patients with a history of orbital or sinus surgery and CT scans with any significant sinus or orbital abnormalities were excluded.
All the measurements required for this study were performed by a single radiologist. Overall, 32 men and 32 women, aged 20 - 67 years, participated in this study. Axial, coronal, and sagittal multiplanar paranasal CT images of the patients were available with a bone window setting as thin sections (0.625 mm). All examinations were evaluated as multiplanar images where various anatomical localizations and measurements could be defined.
3.1. Orbital Measurements
3.1.1. Distance Between the Optic Foramen and Anterior Surface of the Sphenoid Sinus
The medial end of the optic foramen was identified in thin axial CT slices. It was measured by determining the distance between the medial part of the optic foramen (a part of the optic canal opening into the orbit) and the intersection of the anterior surface of sphenoid sinus with the medial orbital wall.
3.1.2. Medial Orbital Wall Length
It refers to the distance between the medial part of the optic foramen and the anterior lacrimal crest.
3.1.3. Distance Between the Optic Foramen and the Carotid Prominence in the Sphenoid Sinus
It was measured by determining the distance between the medial part of the optic foramen and the carotid prominence on the posterior surface of the sphenoid sinus.
3.1.4. Distance Between the Anterior Surface of the Sphenoid Sinus and the Carotid Prominence
It was measured between the anterior surface of the sphenoid sinus and the carotid prominence in the posterior sphenoid sinus.
After measurements, the relationship between the optic foramen and the anterior surface of the sphenoid sinus was examined and categorized as anterior, posterior, and equal to each other. Cases with the same optic foramen position in the right and left orbits were considered as symmetrical, while cases with different positions of the optic foramen were considered as asymmetrical.
3.2. Statistical Analysis
Descriptive statistics are expressed as mean ± SD for continuous variables and as percentage (range) for categorical variables. The confidence intervals (95% CIs) are presented in the tables.
4. Results
The present study was performed on 32 male and 32 female patients. As described in Table 1, the position of the optic foramen relative to each other in the right and left orbits was either symmetrical or asymmetrical (Figure 1).
| Sex | Asymmetry | Symmetry | Total |
|---|---|---|---|
| Female | |||
| N | 8 | 24 | 32 |
| Females (%) | 25.0 | 75.0 | 100.0 |
| Total (%) | 32.0 | 61.5 | 50.0 |
| Male | |||
| N | 17 | 15 | 32 |
| Males (%) | 53.1 | 46.9 | 100.0 |
| Total (%) | 68.0 | 38.5 | 50.0 |
| Total | |||
| N | 25 | 39 | 64 |
| Total (%) | 39.1 | 60.9 | 100.0 |
Position of the Optic Foramen Relative to Each Other in the Eyes
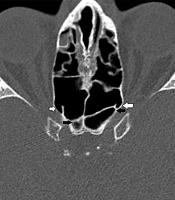
 is located anteriorly to the anterior surface of the sphenoid sinus (black arrow). On the left, the optic foramen (white arrow) is located posteriorly to the anterior surface of the sphenoid sinus (black arrow).")
Asymmetrical location: On the right, the optic foramen (white arrow) is located anteriorly to the anterior surface of the sphenoid sinus (black arrow). On the left, the optic foramen (white arrow) is located posteriorly to the anterior surface of the sphenoid sinus (black arrow).
The localization of the optic foramen relative to the anterior aspect of the sphenoid sinus is shown in Table 2. In the left orbit, the anterior aspect of the sphenoid sinus and the optic foramen were in equal positions in 21.9% of women (n = 7) and 25% of men (n = 8), while in the right orbit, the corresponding frequencies were 21.9% (n = 7) and 31.3% (n = 10), respectively. The optic foramen was opposite to the anterior aspect of the sphenoid sinus in 62.5% (n = 20) of women and 40.6% (n = 13) of men in the left orbit, while in the right orbit, the corresponding rates were 56.3% (n = 18) and 40.6% (n = 13), respectively.
In the left orbit, the optic foramen was posterior to the anterior aspect of the sphenoid sinus in 15.6% of women (n = 5) and 34.4% of men (n = 11), while in the right orbit, the corresponding frequencies were 21.9% (n = 7) and 28.1% (n = 9), respectively. By evaluating both men and women, in the left orbit, the optic foramen was in an equal position to the anterior aspect of the sphenoid sinus in 23.4% of cases (n = 15), in front of it in 51.6% of cases (n = 33), and posterior to it in 25% of cases (n = 16). The corresponding values in the right orbit were 26.6% (n = 17), 48.4% (n = 31), and 25% (n = 16), respectively (Table 2 and Figures 2 - 3).
| Sex | Left orbit | Right orbit | Total | ||||
|---|---|---|---|---|---|---|---|
| Equal | Anterior | Posterior | Equal | Anterior | Posterior | ||
| Female | 7 (21.9) | 20 (62.5) | 5 (15.6) | 7 (21.9) | 18 (56.3) | 7 (21.9) | 32 (100.0) |
| Male | 8 (25.0) | 13 (40.6) | 11 (34.4) | 10 (31.3) | 13 (40.6) | 9 (28.1) | 32 (100.0) |
| Total | 15 (23.4) | 33 (51.6) | 16 (25.0) | 17 (26.6) | 31 (48.4) | 16 (25.0) | 64 (100.0) |
Position of the Optic Foramen Relative to the Anterior Aspect of the Sphenoid Sinus Based on Sex a

The optic foramen anterior to the anterior surface of the sphenoid sinus. The anterior surface of the sphenoid sinus is indicated by a black arrow, and the intersection of the optic foramen with the medial orbital wall is indicated by a white arrow.

The optic foramen is posterior to the anterior surface of the sphenoid sinus. The anterior surface of the sphenoid sinus is indicated by a white arrow and the optic foramen by a black arrow.
The mean distance between the optic foramen and the anterior surface of the sphenoid sinus, depending on whether the optic foramen is anterior, equal, or posterior to the anterior surface of the sphenoid sinus, is presented in Table 3.
| Parameters | N | Mean ± SD | Min | Max | 95% Confidence Interval for Mean Values | |
|---|---|---|---|---|---|---|
| Min | Max | |||||
| OF-AFS (right) (mm) | ||||||
| Equal | 17 | 0.00 ± 0.00 | 0.0 | 0.0 | 0.00 | 0.00 |
| Anterior | 31 | 6.97 ± 3.39 | 2.6 | 16.2 | 5.73 | 8.22 |
| Posterior | 16 | 4.1 ± 1.64 | 1.2 | 7.1 | 3.22 | 4.97 |
| OF-AFS (left) (mm) | ||||||
| Equal | 15 | 0.00 ± 0.00 | 0.0 | 0.0 | 0.00 | 0.00 |
| Anterior | 33 | 6.97 ± 3.03 | 2.4 | 12.4 | 5.9 | 8.05 |
| Posterior | 16 | 4.15 ± 2.36 | 0.7 | 10.5 | 2.88 | 5.41 |
Mean Values of Parameters Based on the Position of the Optic Foramen Relative to the Anterior Surface of the Sphenoid Sinus
The mean values of parameters, including the medial orbital wall length, distance between the optic foramen and the anterior surface of the sphenoid sinus, distance between the optic foramen and the carotid prominence (Figure 4), and distance between the anterior surface of the sphenoid sinus and the carotid prominence, stratified by sex, are presented in Table 4.
 and the carotid prominence (black arrow).")
The anterior surface of the sphenoid sinus (white arrow) and the carotid prominence (black arrow).
| Parameters | Sex | Orbit | N | Mean ± SD | 95% Confidence Interval for Mean Values | |
|---|---|---|---|---|---|---|
| Min | Max | |||||
| MOWL | Female | Right | 32 | 38.40 ± 3.01 | 38.21 | 39.64 |
| Male | 32 | 39.44 ± 2.66 | ||||
| Female | Left | 32 | 38.04 ± 3.1 | 38.27 | 39.8 | |
| Male | 32 | 40.03 ± 2.71 | ||||
| AFS-CP | Female | Right | 32 | 7.32 ± 4.88 | 6.32 | 8.64 |
| Male | 32 | 7.64 ± 4.5 | ||||
| Female | Left | 32 | 6.78 ± 4.99 | 6.13 | 8.67 | |
| Male | 32 | 8.03 ± 5.16 | ||||
| OF-CP | Female | Right | 32 | 9.2 ± 1.76 | 8.57 | 9.53 |
| Male | 32 | 8.91 ± 2.06 | ||||
| Female | Left | 32 | 9.22 ± 2.02 | 8.36 | 9.38 | |
| Male | 32 | 8.52 ± 2.04 | ||||
The Mean Values of Parameters Based on Sex
5. Discussion
In this study, the relationship between the optic foramen and the sphenoid sinus was evaluated in CT images of individuals in the Central Anatolia Region, Turkey. According to the findings, the position of the optic foramen was symmetrical in the two orbits in 60.9% of cases. Based on the measurements, the optic foramen was mainly opposite to the anterior aspect of the sphenoid sinus in both females and males; this finding was more prominent in females. In the right orbit, the mean distance of the optic foramen from the anterior aspect of the sphenoid sinus was +6.97 mm when it was located opposite to it, while it was -4.1 mm when it was located posterior to the anterior surface. Also, in the left orbit, the mean distance was calculated to be +6.97 mm when the optic foramen was anterior to the anterior aspect of the sphenoid sinus and -4.15 mm when it was posterior to it.
Orbital decompression is a surgery performed to reduce increased orbital pressure (10). Adequate knowledge of orbital anatomy is essential for a safe orbital decompression (1). In a study by Alsuhaibani et al., medial orbital decompression could provide more orbital volume compared to lateral orbital decompression (10). In transnasal orbital decompression, the medial orbital wall and parts of the orbital floor are removed (11). The segment of the medial orbital wall close to the orbital apex is in the neighborhood of important anatomical structures, such as the sphenoid sinus, carotid artery, optic canal, and skull base. It is crucial for surgeons to be familiar with the anatomical features of this region (12).
The orbits of female participants in this study were located anteriorly to the anterior surface of the sphenoid sinus in 59.4% of cases, posteriorly to the anterior surface of the sphenoid sinus in 18.75% of cases, and in an equal position to the anterior surface of the sphenoid sinus in 21.9% of cases. On the other hand, in men, they were located anteriorly to the anterior surface of the sphenoid sinus in 40.6% of cases, posteriorly to the anterior surface of the sphenoid sinus in 31.25% of cases, and in an equal position to the anterior surface of the sphenoid sinus in 28.15% of cases. To achieve maximum orbital decompression, the medial orbital wall needs to be opened up to the apex, including the optic foramen (9). It was necessary to enter the sphenoid sinus for this intervention in 18.75% of women and 31.25% of men. The risk increases even more for surgeons because of the relationship between the sphenoid sinus and important anatomical structures, such as the carotid artery, optic canal, and skull base (12).
In this regard, Aujla et al., in their study on 50 individuals, evaluated the position of the optic foramen relative to the anterior aspect of the sphenoid sinus. They categorized the position of the optic foramen to be anterior or posterior to the sphenoid sinus (3). However, in the present study, we considered the optic foramen to be in an anterior, posterior, or equal position to the sphenoid sinus. Moreover, the sex factor was considered in the current study. In the study by Aujla et al., the optic foramen was posterior to the anterior aspect of the sphenoid sinus in approximately 54% of the orbits and asymmetrical in the right and left orbits in 20% of cases; however, in the present study, the rate of asymmetry was higher (39.1%) (3). Regarding sex, asymmetry was less frequent in women (25%) than in men (53.1%). In the study by Aujla et al., the optic foramen was mostly posterior to the anterior surface of the sphenoid sinus, whereas in our study, the optic foramen was mostly anterior to the anterior surface of the sphenoid sinus (3); this difference might be attributed to race and sex (13).
The current study measured the medial orbital wall length in the right and left orbits, which ranged from 38 mm to 40 mm in men and women on average. This finding is in line with the results reported in studies by Abed et al., Akdemir et al., Aujla et al., Karakas et al., and Singh et al. (40.56 mm; 37.35 ± 2.73 mm; 38.9 mm; 41.7 ± 3.1 mm; and 41.21 ± 0.86 mm, respectively) (3, 14-17). Based on the results of our study, the distance between the carotid prominence and the anterior surface of the sphenoid sinus was 7.05 mm (1.05 - 17.0 mm) in women and 7.84 mm (1.2 - 17.3 mm) in men. The distance between the carotid prominence and the optic foramen was 9.2 mm (4.1 - 13.2 mm) in women, while it was 8.71 mm (4.12 - 12.6 mm) in men on average. However, in the study by Aujla et al., the distances between the carotid prominence and the anterior surface of the sphenoid sinus and between the carotid prominence and the optic foramen were measured to be 1.1 - 17.5 mm and 4.8 - 12.3 mm, respectively (3). Surgeons who perform procedures in this region need to be familiar with the relationship between the optic foramen and the carotid artery and the anterior surface of the sphenoid sinus. The results reported by Aujla et al. and the values calculated in our study seem to be compatible (3).
In conclusion, based on the results of CT scans, the optic foramen was mainly located opposite to the anterior aspect of the sphenoid sinus; this position was more frequent in females (59.4%) than in males (40.6%). Besides, the optic foramen were symmetrical in the two orbits in 60.9% of cases. The collected data can help surgeons in orbital decompression procedures or other surgeries that are performed posterior to the orbit; it should be noted that there may be differences depending on race and sex.
