



1. Background
The word “ataxia”, which is derived from a Greek term, is composed of two parts, that is, “a” meaning “without” and “taxis” meaning “order” (1). Generally, ataxia refers to a disorder where motor coordination is absent. It is recognized as a threatening symptom due to uncertainties and lack of evidence on how clinicians can identify its underlying cause. Commonly, ataxia is associated with cerebellar diseases. However, it is not specific to these disorders, as many other conditions may be predisposing factors for ataxia, such as peripheral nerve and muscular disorders (2).
Acute ataxia (AA) is the most common cause of childhood ataxia, accounting for 30 - 50% of all cases. It may be caused by various conditions, including post-infectious inflammatory disorders, toxins, tumors, stroke, middle-ear infections, acute disseminated encephalomyelitis (ADEM), and Guillain-Barre syndrome (GBS) (3, 4). Among these etiologies, post-infectious inflammatory disorders, which are commonly associated with varicella zoster virus, are the most prevalent ones (5). Neuroimaging can play a significant role in diagnosis and treatment planning. In some etiologies, such as stroke, tumors, and ADEM, imaging studies can represent the characteristic findings of the etiology. However, imaging studies are negative for the most prevalent etiologies, including post-infectious cerebellar disorders, GBS, and toxin ingestion (6).
2. Objectives
This study aimed to evaluate the neuroimaging findings of children with AA and to investigate the possible association between clinically urgent neurological pathology (CUNP) based on neuroimaging and different signs, symptoms, and laboratory test results.
3. Patients and Methods
3.1. Study Design
This cross-sectional study was conducted on all children with AA under the age of 18 years, presenting to the emergency department of Children’s Medical Center, Tehran, Iran, from March 2009 to February 2020. This center is a tertiary educational hospital, affiliated to Tehran University of Medical Sciences (TUMS), Tehran, Iran.
3.2. Patient Identification
The participants were selected based on the international classification of diseases-9 (ICD-9) codes. The keywords searched in the electronic medical records were as follows: ADEM, brain tumor, encephalitis, cerebellitis, GBS, meningitis, migraine, drug poisoning, stroke, and ataxia. Subsequently, potential cases were reviewed manually.
3.3. Patient Population
All patients presenting with AA, who underwent magnetic resonance imaging (MRI), computed tomography (CT) scan, or both, were included in this study. On the other hand, patients with a history of neurological or medical disorders explaining ataxia (e.g., known brain mass, ataxia telangiectasia, epilepsy, and ventricular shunts), claudication or gait abnormalities due to pain or weakness (pseudo-ataxia), traumatic brain injury (TBI), and severe loss of consciousness (unresponsive patients) were excluded. Also, patients were removed if their medical records had key information (e.g., no brain imaging) missing.
3.4. Data Collection
The patients’ electronic medical records were reviewed by the principal investigator (MI). Five variable categories were extracted: Demographic information, clinical history, laboratory findings, imaging results, and in-hospital outcomes. The demographic data included age and sex. Variables extracted from the patients’ clinical history included the duration of symptoms before presentation, a recent history of febrile illness (i.e., presence of fever or body temperature above 38°C in the last month), focal neurologic deficits (e.g., ophthalmoplegia), and accompanying signs and symptoms (e.g., nausea, vomiting, fever, and headache).
Moreover, laboratory findings, including electrolyte levels, white blood cell count, and the results of cerebrospinal fluid analysis and toxicology studies, were reviewed. The imaging results were extracted from the radiology reports available in the medical records. The diagnosis documented in the discharge summary was considered as the final diagnosis. Some clinical features depending on the patient’s verbal communication ability, such as vertigo, were considered missing in non-verbal children. If there was no information related to a variable in the patient’s medical record, it was considered missing.
3.5. Definitions
In this study, AA was defined as difficulty walking/standing or truncal instability within 30 days before presentation (6). Clinically urgent neurological pathology (CUNP) was defined as any neuroimaging finding, which normally prompts a medical or surgical intervention (7, 8). Such findings mainly include ADEM, brain tumors, brain abscesses, and infarctions. Brain MRI and CT scan were considered as eligible imaging studies.
3.6. Outcomes
The primary outcome of this study was determining the proportion of various causes of AA among patients. The secondary outcome was investigating the association of CUNP with different factors.
3.7. Ethical Considerations
This study was approved by the Ethics Committee of TUMS, Tehran, Iran (IR.TUMS.CHMC.REC.1399.031).
3.8. Statistical Analysis
Mean and standard deviation (SD) were calculated for continuous variables with a normal distribution, and frequency was calculated for categorical variables. Also, median and interquartile range (IQR) were measured when a continuous quantitative variable did not show a normal distribution. The data distribution of continuous variables was assessed by two-sample Kolmogorov-Smirnov test. Moreover, Pearson’s chi-square and Fisher’s exact tests were used to compare categorical variables. Independent samples t-test was also conducted for comparison of continuous numerical variables. Additionally, bootstrapping was performed to calculate the confidence intervals (CIs). IBM SPSS version 22 (released in 2013, IBM SPSS Statistics for Windows, IBM Corp., Armonk, NY, USA) was used for all statistical analyses. A P-value less than 0.05 was considered statistically significant.
4. Results
4.1. Demographic Data
After reviewing the electronic medical records of 3,810 patients, 119 cases were selected for this study. The mean and median age of the study population were 4.9 and 4 years, respectively, with an IQR of 2-7 years. Overall, 51% of the population was female. Also, the mean age of female and male patients was 4.8 and 5.1 years, respectively. A more comprehensive description of the study population is presented in Table 1.
| Variables | Mean ± SD | Percentage (positive No./total No.) | 95% CI | Median | IQR |
|---|---|---|---|---|---|
| Demographics | |||||
| Age (y) | 4.9 ± 3.4 | - | 4.3 - 5.6 | 4 | 2 - 7 |
| Sex, female | - | 51.3 (61/119) | 43 - 60.5 | - | - |
| Clinical history | |||||
| Duration of symptoms (d) | 6.1 ± 7.1 | - | 4.8 - 7.5 | 3 | 1 - 10 |
| Recent febrile illness a | - | 61.5 (72/117) | 52.1 - 70.1 | - | - |
| Drug misuse | - | 4.3 (5/117) | 0.9 - 8.5 | - | - |
| Varicella infection b | - | 10.1 (12/119) | 5 - 16 | - | - |
| Vertigo | - | 17.6 (21/119) | 10.9 - 24.4 | - | - |
| Otalgia | - | 3.4 (4/119) | 0.8 - 6.7 | - | - |
| Nausea or vomiting | - | 50.4 (57/113) | 41.6 - 59.3 | - | - |
| Nystagmus | - | 8.2 (8/97) | 3.1 - 14.4 | - | - |
| Dysarthria | - | 14.3 (17/119) | 8.4 - 21 | - | - |
| Altered state of consciousness | - | 8.5 (10/117) | 3.4 - 13.7 | - | - |
| Hyporeflexia | - | 20.6 (20/97) | 12.4 - 28.9 | - | - |
| Ophthalmoplegia | - | 12.7 (14/110) | 6.4 - 19.1 | - | - |
| Meningeal irritation c | - | 5 (6/119) | 1.7 - 9.2 | - | - |
| Torticollis | - | 1.7 (2/115) | 0 - 4.3 | - | - |
| Headache | - | 21 (25/119) | 13.4 - 28.6 | - | - |
| Focal neurologic deficit | - | 19.3 (21/109) | 11.9 - 26.6 | - | - |
| Fever d | - | 14.2 (16/113) | 8 - 21.2 | - | - |
| Rash e | - | 10.7 (12/112) | 5.4 - 17 | - | - |
| Laboratory | |||||
| Serum magnesium (mg/dL) | 2.1 ± 0.3 | - | 2 - 2.2 | 2.1 | 1.9 - 2.3 |
| Serum sodium (mEq/L) | 139.3 ± 3.1 | - | 138.6 - 140 | 140 | 137 - 141 |
| Serum phosphorus (mg/dL) | 4.8 ± 0.8 | - | 4.6 - 5 | 4.7 | 4.2 - 5.3 |
| Imaging | |||||
| CUNP, present | - | 31.1 (37/119) | 22.7 - 39.5 | - | - |
| MRI, CUNP+ | - | 41.9 (13/31) | 25.9 - 59.4 | - | - |
| CT, CUNP+ | - | 13.8 (9/65) | 7.1 - 23.7 | - | - |
| Both, CUNP+ | - | 65.2 (15/23) | 44.9 - 82 | ||
| Final diagnosis | |||||
| ADEM | - | 7.6 (9/119) | 3.4 - 12.6 | - | - |
| APCA | - | 24.4 (29/119) | 16.8 - 31.9 | - | - |
| Drug intoxication | - | 4.2 (5/119) | 0.8 - 8.4 | - | - |
| Acute cerebellitis | - | 7.6 (9/119) | 3.4 - 12.6 | - | - |
| Encephalitis | - | 4.2 (5/119) | 0.8 - 8.4 | - | - |
| Meningitis | - | 3.4 (4/119) | 0.8 - 6.7 | - | - |
| Stroke | - | 4.2 (5/119) | 0.8 - 8.4 | - | - |
| Seizure | - | 0.8 (1/119) | 0 - 2.5 | - | - |
| Tumor | - | 16.8 (20/119) | 10.1 - 23.5 | - | - |
| Guillain-Barre syndrome | - | 15.1 (18/119) | 9.2 - 21.8 | - | - |
| Other etiologies | - | 11.8 (14/119) | 6.7 - 17.6 | - | - |
| Outcomes | |||||
| Length of hospital stay (d) | 7.4 ± 6.1 | - | 6.3 - 8.6 | 6 | 3.5 - 10 |
Descriptive Statistics of the Patients
4.2. Neuroimaging Results
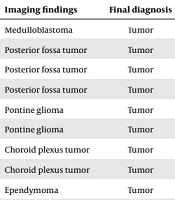
Thirty-one patients only underwent MRI, 64 patients only underwent CT, and 24 patients underwent both imaging modalities. Overall, 37 (31.09%) patients were diagnosed with CUNP. Fifteen patients with CUNP underwent both MRI and CT scan, 13 patients underwent only MRI, and nine patients only underwent CT scan. As shown in Table 2, the frequency of pathologies found on the images of patients with CUNP was as follows: Tumor, ADEM, stroke, meningitis, encephalitis, and acute cerebellitis, respectively. However, the most common final diagnoses were acute post-infectious cerebellar ataxia (APCA) (29/119), tumor (20/119), and GBS (18/119), respectively (Table 1).
| Count | Imaging (CT/MRI) | Imaging findings | Final diagnosis |
|---|---|---|---|
| 3 | CT | Medulloblastoma | Tumor |
| 2 | Both | Posterior fossa tumor | Tumor |
| 1 | CT | Posterior fossa tumor | Tumor |
| 1 | MRI | Posterior fossa tumor | Tumor |
| 3 | Both | Pontine glioma | Tumor |
| 2 | MRI | Pontine glioma | Tumor |
| 2 | CT | Choroid plexus tumor | Tumor |
| 1 | MRI | Choroid plexus tumor | Tumor |
| 1 | MRI | Ependymoma | Tumor |
| 1 | Both | Cerebellar tumor | Tumor |
| 1 | MRI | Suprasellar tumor | Tumor |
| 1 | MRI | Pilocytic astrocytoma | Tumor |
| 2 | Both | Left cerebellar stroke | Stroke |
| 1 | MRI | Basilar and carotid dissection | Stroke |
| 1 | CT | Cerebellar stroke | Stroke |
| 1 | CT | ICH | Stroke |
| 5 | Both | ADEM | ADEM |
| 4 | MRI | ADEM | ADEM |
| 1 | MRI | Mastoiditis | Meningitis |
| 1 | Both | Encephalitis | Encephalitis |
| 1 | Both | Brain stem encephalitis | Others |
| 1 | CT | Acute cerebellitis | Acute cerebellitis |
The Imaging Findings of Patients with CUNP
4.2.1. Comparison of Patients with and Without Clinically Urgent Neurological Pathology
As shown in Table 3, the features of patients (demographic features, clinical history, laboratory findings, abnormal EEG, and length of stay in hospital) with and without CUNP were compared, and some significant differences were found. These features included the duration of symptoms, recent history of febrile illness, nausea and/or vomiting, hyporeflexia, ophthalmoplegia, headache, focal neurologic deficit, fever, serum concentrations of sodium and phosphate, and the length of hospital stay.
| Variables | CUNP (n = 37) | No CUNP (n = 82) | OR (95% CI) | P-value | ||
|---|---|---|---|---|---|---|
| Mean ± SD (95% CI) | Percentage (positive No./total No.) | Mean ± SD (95% CI) | Percentage (positive No./total No.) | |||
| Demographics | ||||||
| Age (y) | 4.2 ± 3.1 (3.3 - 5.2) | - | 5.3 ± 3.5 (4.6 - 6) | - | - | 0.12 |
| Sex, female | - | 59.5 (22/37) | - | 47.6 (39/82) | 1.62 (0.74 - 3.5) | 0.23 |
| Clinical history | ||||||
| Duration of symptoms (d) | 11.1 ± 9.7 (7.9 - 14.4) | - | 3.9 ± 4 (3.1 - 4.8) | - | - | < 0.001 |
| Recent febrile illness | - | 44.4 (16/36) | - | 69.1 (56/81) | 0.36 (0.16 - 0.8) | 0.01 |
| Drug misuse | - | 0 (0/36) | - | 6.2 (5/81) | - | 0.32 |
| Varicella infection | - | 2.7 (1/37) | - | 13.4 (11/82) | 0.18 (0 - 1.4) | 0.10 |
| Vertigo | - | 21.6 (8/37) | - | 15.8 (13/82) | 1.46 (0.5 - 3.9) | 0.45 |
| Otalgia | - | 2.7 (1/37) | - | 3.7 (3/82) | 0.73 (0.1 - 7.3) | 1.00 |
| Nausea or vomiting | - | 64.7 (22/34) | - | 44.3 (35/79) | 2.3 (1 - 5.3) | 0.047 |
| Nystagmus | - | 9.4 (3/32) | - | 7.7 (5/65) | 1.24 (0.3 - 5.6) | 1.00 |
| Dysarthria | - | 13.5 (5/37) | - | 14.6 (12/82) | 0.91 (0.3 - 2.8) | 0.87 |
| Altered state of consciousness | - | 5.6 (2/36) | - | 9.9 (8/81) | 0.54 (0.1 - 2.7) | 0.72 |
| Hyporeflexia | - | 0 (0/22) | - | 26.7 (20/75) | - | 0.01 |
| Ophthalmoplegia | - | 35.5 (11/31) | - | 3.8 (3/79) | 13.93 (3.5 - 54.7) | < 0.001 |
| Meningeal irritation | - | 8.1 (3/37) | - | 3.7 (3/82) | 2.32 (0.4 - 12.1) | 0.37 |
| Torticollis | - | 2.9 (1/35) | - | 1.3 (1/80) | 2.32 (0.1 - 38.2) | 0.52 |
| Headache | - | 32.4 (12/37) | - | 15.9 (13/82) | 2.55 (1 - 6.3) | 0.04 |
| Focal neurologic deficit | - | 42.4 (14/33) | - | 9.2 (7/76) | 7.26 (2.6 - 20.5) | < 0.001 |
| Fever | - | 25 (9/36) | - | 9.1 (7/77) | 3.33 (1.1 - 9.8) | 0.02 |
| Rash | - | 2.8 (1/36) | - | 14.5 (11/76) | 0.17 (0 - 1.4) | 0.10 |
| Laboratory findings | ||||||
| Serum magnesium (mg/dL) | 2.1 ± 0.3 (2 - 2.2) | - | 2.1 ± 0.3 (2-2.2) | - | - | 0.90 |
| Serum sodium (mEq/L) | 138.3 ± 3.2 (137.3 - 139.4) | - | 139.8 ± 2.9 (139.1 - 140.4) | - | - | 0.02 |
| Serum phosphorus (mg/dL) | 4.3 ± 0.6 (4 - 4.6) | - | 4.9 ± 0.8 (4.7 - 5.1) | - | - | 0.01 |
| WBC, leukocytosis a | - | 45.5 (15/33) | - | 32 (24/75) | 1.77 (0.8 - 4.1) | 0.18 |
| CSF analysis, abnormal b | - | 17.4 (4/23) | - | 17.9 (5/28) | 0.97 (0.2 - 4.1) | 1.00 |
| Urine toxicology, positive c | - | 20 (1/5) | - | 12 (3/25) | 1.83 (0.2 - 22.4) | 0.54 |
| EEG | ||||||
| EEG, abnormal d | - | 20 (1/5) | - | 31.6 (6/19) | 0.54 (0 - 5.9) | 1.00 |
| Outcomes | ||||||
| Length of hospital stay (d) | 11 ± 7.8 (8.6 - 13.7) | - | 5.8 ± 4.3 (5 - 6.8) | - | - | < 0.001 |
Comparison of Patients with and Without CUNP
5. Discussion
This cross-sectional study was conducted on the neuroimaging findings of children with AA, admitted to a large tertiary care center over 10 years. Children with at least one neuroimaging study were recruited in this study; consequently, our results only apply to patients with brain MRI or CT scan. Nearly 31% of the study population showed CUNP on neuroimaging. The most significant factors associated with the presence of CUNP included a longer duration of symptoms, ophthalmoplegia, focal neurologic deficit, and fever. On the other hand, a recent history of febrile illness and hyporeflexia were associated with the reduced presence and observation of CUNP on imaging.
In the present study most children with AA had no clinically urgent findings on neuroimaging. Evidence suggests that APCA, as the most common etiology of AA in children (6, 8, 9), does not require further imaging workups. However, patients with the following risk factors can benefit from imaging studies: Age > 3 years, duration of symptoms > 3 days, meningeal irritation and focal neurologic signs, hyporeflexia, history of trauma, and ophthalmoplegia (7, 8, 10).
The current findings are mainly consistent with previous studies. However, since our study population was heterogeneous, only patients with neuroimaging findings were included; therefore, some differences are expected. One of the most striking differences between the present study and previous research is that hyporeflexia was not associated with AA in the current study, whereas some studies found it to be a risk factor. This discrepancy may be attributed to the relatively large number of patients with GBS in our study, as they naturally do not have positive findings on the brain MRI or CT scan. Similarly, a recent history of febrile illness possibly suggests a viral infection and indicates APCA, which is not visible in neuroimaging.
Most previous studies support neuroimaging if a patient has a focal neurologic deficit, signs of increased intracranial pressure, marked asymmetry of ataxia, longer duration of symptoms (e.g., > 3 days), or older age (e.g., > 3 years) (7, 8, 10, 11). The UpToDate currently suggests neuroimaging for patients with an altered state of consciousness, focal neurologic signs, cranial neuropathies, marked asymmetry of ataxia , suspicion of a mass lesion, or positive history of trauma (12). However, none of the mentioned studies discuss when neuroimaging results should be suspected. Generally, some pathologies may not manifest in some imaging modalities. Considering the associations discovered in this study, a reevaluation of patients using another more sensitive imaging modality is necessary if the patient has no CUNP in the first imaging study, but has at least one of the following signs and symptoms: A longer duration of symptoms, ophthalmoplegia, focal neurologic deficit, or fever at presentation.
The present study had some limitations. First, it only included patients with neuroimaging studies; therefore, the results cannot be generalized to all children with AA. Second, the used imaging modalities were not consistent; therefore, comparison of these two modalities is flawed. Third, AA was defined as ataxia occurring within the last 30 days of presentation. Consequently, our population may have more life-threatening etiologies compared to other studies, thereby overstating the prevalence of CUNP. Fourth, since data collection was only performed by two people in this study, the population may be subject to selection bias. Fifth, this retrospective study had all the limitations attributed to this type of design, such as lack of follow-up. Finally, the study population was too small to reveal other significant associations; therefore, more extensive studies or meta-analyses are suggested in the future.
In conclusion, APCA was the most common cause of AA in children undergoing neuroimaging studies in our center. As some pathologies might not be detected using some imaging modalities, patients with risk factors, such as a longer duration of symptoms, ophthalmoplegia, focal neurologic deficit, and fever, who have no positive findings on initial imaging, should undergo further imaging with higher sensitivity. On the other hand, patients with hyporeflexia and a recent history of febrile illness might benefit more from other diagnostic modalities.
