Congenital pulmonary venolobar syndrome (CPVS) is a group of several congenital abnormalities of the thorax. Hypogenetic lung and partial anomalous pulmonary venous return (PAPVR) is the most common anomaly of the group. Other major components are interruption of the pulmonary artery and/or inferior vena cava, pulmonary sequestration, systemic pulmonary arterializations and an accessory diaphragm. Minor components are tracheal trifurcation, eventration and partial absence of the diaphragm, phrenic cyst, horseshoe lung, superior vena cava anomalous and absence of the left pericardium (
1,
2,
4) (
Figure 4). Anomalous pulmonary venous drainage is an extracardiac left-to-right shunt which leads the pulmonary venous flow into the right side circulation. The disease has partial and total forms. Right-to-left shunt by a septal defect or patent ductus arteriosus is mandatory in the total form (
5). PAPVR may accompany atrial septal defects and hypogenetic lung. Hypogenetic lung is a component of CPVS (
4,
5,
6). Scimitar syndrome is a subtype of PAPVR in CPVS group. Hypogenetic lung may occur not only on the right side, but also in the left pulmonary lobe (
5,
6,
7). Scimitar vein usually collects anomalous blood to the infradiaphragmatic portion of the inferior vena cava, although the suprahepatic vena cava, hepatic veins, portal vein, azygos vein, coronary sinus and right atrium drainage may also be seen. Left atrium drainage known meandering pulmonary vein (
4,
7). Our patient has an anomalous scimitar vein which originates from the right pulmonary vein. The branches of scimitar vein drained to the supradiaphragmatic portion of the inferior vena cava. Scimitar syndrome is a rare congenital cardiopulmonary malformation and existence of horseshoe lung is extremely uncommon. This syndrome is a subtype of PAPVR in CPVS. Female involvement is higher. Familial determination is extremely rare. The syndrome is usually asymptomatic and has an incidental finding in adults; however, it is more symptomatic in early ages. Right pulmonary lobe hypoplasia exlains dextroposition of the heart and the mediastinum shift. Congenital heart disease also increases the diagnostic ratio in childhood (
8). Pulmonary aplasia is complete absence of the lobe tissue and airways. The rudimental bronchus shows sudden occlusion (
4). Horseshoe lung is characterized as fusion of the pulmonary lobes with an isthmus in the midline. The lobes may or may not be separated by a pleural mem- brane. The membrane is a clue of nonunion; therefore, this pseudofusion displays congenital pseudohorseshoe lung. Nonexistence of the pleural membrane is a true horseshoe lung malformation (
2,
3). We believe that this terminology should only be used in congenital malformations. Many diseases such as necrotizing pneumonia cause volume loss and a destroyed lung. The nonaffected lobe may expose compensatory hypertrophy. Acquired pulmonary diseases may lead to inflammatory conditions and fibrosis in the lung tissue. This situation may cause an acquired horseshoe appearance. Pulmonary hypoplasia may exist in scimitar syndrome. Aplasia of the pulmonary artery shines a light on pulmonary lobe agenesis or hypoplasia. The hypoplastic tissue is drained by peripheral bronchial arteries of the systemic collateral circulation (
4). Scimitar syndrome is characterized by hypoplasia of the right pulmonary lobe and pulmonary artery with anomalous venous connection (
9,
10,
11). Diaphragmatic anomalies exist in CPVS. These anomalies include congenital weakness, eventration, accessory leaf and congenital diaphragmatic defects. Elevation of hemidiaphragm and abdominal tissue herniation may occur in scimitar syndrome (
4,
8). Small posterior diaphragmatic hernia (Bochdalek hernia) appears in 6% of the population and left side involvement has dominance. Morgagni hernia is less common. The defect usually occurs in the ventromedial area of the right leaf (
6). Hemivertebral anomalies may also exist in the disease (
8).



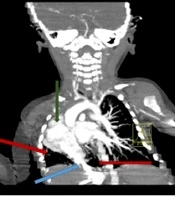
. B, CT scan of the lung base. The branches of the anomalous venous structure are visible (arrows). C,D, Distal branches drained to the inferior vena cava (arrows). Abdominal fatty tissue and a part of the liver (curved arrow) are herniated to the posterobasal region of the thorax. (Bochdalek’s hernia)")