








1. Background
One of the significant health crises of the present age is the COVID-19 virus, or Coronavirus epidemic, which has severely impacted the psychological and physical well-being of many individuals (1-3). The primary signs and symptoms of COVID-19 infection include nausea, vomiting, fatigue, bruising, headache, and dry cough (4). Preliminary studies suggest that individuals with underlying health conditions, particularly cardiovascular disorders, are at a higher risk of developing severe complications and mortality due to COVID-19 (5-10).
The COVID-19 virus poses the greatest threat to patients with pre-existing conditions, particularly those with a history of heart disease, due to its effects on respiratory infections. These respiratory infections caused by the virus inflict the most damage on individuals with underlying conditions, especially those with cardiovascular disease (11).
Given that individuals with underlying health issues are at greater risk from COVID-19 compared to others and that one of the highest-risk groups for COVID-19-related mortality includes patients with heart conditions, particularly congenital heart disease, it is crucial to focus on these populations. Additionally, the coronavirus pandemic has significantly increased psychological consequences in the general population, including those affected by the virus (12).
Considering the limited information available about the psychological symptoms of COVID-19 in patients with congenital heart disease, it is essential to address the needs of this vulnerable group.
With the emergence of the Coronavirus, studies on the effectiveness of quarantine and its wide-ranging health consequences have increased (13). Coronavirus disease has significantly altered people's living conditions, causing confusion and bringing about destructive effects such as fear, anxiety, depression, and insomnia (4, 12, 14). The spread of the Coronavirus disease has led people in many countries to remain at home or in quarantine centers. The uncertainty surrounding the progression and duration of the epidemic imposes additional psychological pressure on the public. A possible explanation for these mental health issues may be the worry and anxiety about contracting the disease and fears related to managing and controlling it (15). Research indicates that symptoms of anxiety and depression are on the rise due to social distancing, fatigue, and exhaustion associated with quarantine (16-18).
In the context of the COVID-19 pandemic, the concept of fatigue has entered the literature. Quarantine fatigue refers to the negative physical and psychological effects resulting from isolating and restricting the movement of individuals potentially exposed to an infectious disease (19). The imposition of quarantine has been linked to an increase in psychological issues, including worry, obsessive behaviors, paranoia, depression, and post-traumatic stress disorder. The most common triggers of stress and psychological disorders, such as anxiety, depression, and fear of the Coronavirus, among individuals in quarantine are: Fear of infection or contaminating others, prolonged quarantine periods, insufficient support, lack of access to medical care and adequate food, and, ultimately, fatigue and impatience caused by quarantine (20).
Studies have investigated the determinants of quarantine fatigue, emphasizing various theoretical concepts and frameworks.
In this regard, a study in Sri Lanka found that women, frontline medical staff, quarantined individuals, and psychiatric patients are at higher risk of mental disorders (21). Similarly, a study in China revealed that women who experienced quarantine reported depression, anxiety, sadness, substance abuse, insomnia, and psychosis among the public. Mental disorders in quarantined individuals often manifest as acute stress disorder, post-traumatic stress disorder, substance abuse and dependence, irritability, anxiety, insomnia, poor performance, numbness, and depression (4, 12, 14, 22).
Aliakbari Dehkordi et al., in their study on patients infected with the Coronavirus, found that these patients experience several psychosocial consequences, including negative emotions such as depression, anxiety, fear of death, feelings of rejection, reduced social activities, and decreased effective communication with family and those around them. They also reported that 75% of the participants in their study stated their quality of life had declined after the infection. These individuals believed their lives were wasted in quarantine due to a lack of entertainment, which contributed to their depression (23).
The Coronavirus epidemic has posed serious threats to people's physical health and lives while also causing widespread psychological issues, such as fear, depression, and anxiety, particularly among heart patients. Research literature also indicates that social isolation has a negative impact on people's psychological health. The loneliness resulting from quarantine, along with the fatigue it generates, is associated with an increased risk of mental health problems, including anxiety and depression (24). The results of studies on the effects of quarantine on mental health have reported issues such as rejection, loneliness, anger, depression, anxiety, lack of self-respect, reduced self-control, fear, boredom, emotional problems, disruptions in daily activities, and negative effects on coping and psychological functions. Recent meta-analyses have also reported significant findings regarding the effects of quarantine and isolation on mental health, including rejection, loneliness, anger, depression, anxiety, lack of self-esteem, reduced self-control, fear, boredom, emotional problems, disruptions in daily activities, and negative effects on coping and psychological functions (25, 26). On the other hand, fear of illness, financial problems due to quarantine, temporary or permanent unemployment, limited social communication, uncertainty about the end of the pandemic, worry for family and friends, and fear of the future are also factors contributing to mental health issues.
Among the factors affecting people are the psychological effects of quarantine fatigue and stress caused by the COVID-19 pandemic. This stress is a predictor of anxiety and depression in individuals (27). In recent years, anxiety has increasingly been a focus in medical research related to the disease COVID-19. Due to its unknown nature and the cognitive ambiguity it creates, COVID-19 has caused significant anxiety and worry for people across societies (28). Fear of the unknown has always been a source of anxiety for humans (29), and this anxiety is heightened in heart patients, as they are part of the vulnerable and at-risk group for contracting the Coronavirus. Therefore, the presence of anxiety, tension, or emotional disturbance may lead to disruptions in daily functions (30). The results of numerous studies on COVID-19 patients indicate the prevalence of various psychological disorders, including coronavirus anxiety, pervasive anxiety, death anxiety, depression, sleep quality problems, and emotional changes, all with high rates of occurrence among these patients (4, 31-33).
Additionally, coronavirus anxiety, which may potentially be linked to quarantine fatigue, refers to the fear of the Coronavirus. Disturbances in the daily lives of people affected by the coronavirus disease include issues such as changes in how people earn a living, economic problems, feelings of helplessness and despair, and a loss of a sense of safety. Other concerns include limitations on socializing, production, and recreation, the fear of infection due to being in public spaces, contact with contaminated surfaces, and close contact with others. Worries about financial bankruptcy have also caused avoidance and withdrawal from daily activities and social isolation, which, in turn, has destroyed opportunities for human relationships and social support (34), contributing to quarantine fatigue.
Another factor related to quarantine fatigue is depression. The uncertain death rate and the rapid spread of COVID-19 have caused significant psychological reactions among people, including anxiety, fear, panic, anger, and depression (Nasirzadeh et al., 2020) (35). Several studies have examined psychological disorders such as depression during the COVID-19 outbreak (2, 36). Depression is a disorder characterized by symptoms such as hopelessness, low mood, sadness, low self-esteem, and feelings of worthlessness. These symptoms lead to a decrease in self-worth, a lack of interest in life, and a reduction in efforts to achieve important life goals. Depression is also associated with deterioration in health status and even suicide attempts (29, 37, 38). The results of studies show that people who were quarantined, or whose family and friends were quarantined, or those who believed they were infected with the disease, exhibited higher levels of depression (39). People in quarantine may also experience anxiety, discrimination, boredom, loneliness, guilt, and depression. Mental health support should be provided to those in need, especially children and the elderly (32).
Given the coronavirus epidemic and the serious threats it poses to people's physical health and lives, as well as the importance of investigating quarantine fatigue and its psychological consequences, it is crucial and necessary to address this issue at this time. Special attention should be given to the psychological health of the general public, especially individuals with heart disease. Additionally, the COVID-19 virus, which causes respiratory infections, results in the greatest damage and the highest mortality rate among people with pre-existing health conditions, particularly those with heart disease. The death rate from COVID-19 is significantly higher in the elderly and individuals with underlying conditions, especially cardiovascular patients, compared to healthy individuals (10). People with underlying diseases are more vulnerable to COVID-19 than others. Studies have also shown that heart patients, particularly those with congenital heart disease, are among the groups at higher risk of death from COVID-19. Therefore, it is essential to prioritize the care of this patient group. To improve medical care, attention should be given not only to the physical aspects of treating COVID-19 but also to the psychological well-being of patients, especially those with congenital heart disease.
Despite the fact that fear of COVID-19, depression, and anxiety related to the virus and its impact on quarantine consequences have been examined in various studies, no studies have been found that specifically investigate the relationship between the three variables—fear of COVID-19, depression, and COVID-19 anxiety—and how they are related to quarantine fatigue. Additionally, determining which psychological variables may predict quarantine fatigue in patients with congenital heart disease is of practical importance. Given the high prevalence of COVID-19 and the need to prioritize the health of patients with congenital heart disease, understanding the predictors of quarantine fatigue will help health professionals implement targeted interventions to reduce its consequences, improve coping strategies, and enhance adaptability.
2. Objectives
Based on the existing literature and the lack of studies showing the diagnostic role of these variables in quarantine fatigue among patients with congenital heart disease, this research aimed to investigate the predictive role of fear of COVID-19, symptoms of depression, and COVID-19-related anxiety in quarantine fatigue among patients with congenital heart disease.
3. Methods
The current research design is descriptive-correlational and was conducted to investigate the predictive role of fear of COVID-19, symptoms of depression, and COVID-19-related anxiety in quarantine fatigue among patients with congenital heart disease.
3.1. Statistical Analysis
The current research design is descriptive-correlational, conducted with the aim of investigating the relationship between fear of COVID-19, quarantine fatigue, and depression in patients with congenital heart disease. The statistical population includes all patients with congenital heart disease referred to Shahid Rajaee Hospital and the (X-Country) Heart Center. To estimate the sample size, Sample Power software was used, and with a power of 90%, 105 patients were selected and tested from among the patients with congenital heart disease using the available sampling method. Due to the use of the available sampling method and the researchers' discretion in choosing the sample size, no drop-out in the sample size was observed.
The inclusion criteria for the present study were: (1) Congenital anatomical heart disease confirmed by echocardiography, heart tests, or surgery; (2) ability to read and understand the content of the questionnaire and complete the consent form; (3) age over 18 years. Exclusion criteria included other medical and psychological conditions that could limit participation in the study, fatigue, unwillingness to participate, and lack of written and verbal consent.
In this research, to test the hypotheses, four questionnaires were used: The Coronavirus Anxiety Scale (CAS), Depression Scale (DS), Fear of COVID-19 Scale (FCV-19S), and Quarantine Fatigue Scale.
3.2. The Coronavirus Anxiety Scale
This scale was developed by Lei et al. to identify potential cases of dysfunctional anxiety related to the coronavirus crisis. It helps assess the history of anxiety and other components, as well as measure the physiological symptoms caused by the coronavirus. The scale uses a 5-point Likert scale ranging from 0 (not at all) to 4 (almost every day) over the past two weeks. A high score on a specific item or a high total score (≥ 9) may indicate signs of problems that may require further evaluation or treatment. Confirmatory factor analysis showed that the CAS measures a reliable one-dimensional construct (α = 0.93), which is consistent across gender, race, and age. Additionally, the CAS has good construct validity and has been reported as a reliable and efficient measure (39).
3.3. Depression Scale
This test is one of the most widely used and well-known self-assessment tools. To date, more than 1,000 studies have been conducted on it, contributing to its widespread recognition. These studies have demonstrated that the diagnostic power of this tool in identifying depressed individuals is comparable to that of long and expensive clinical interviews. The test consists of 21 items related to different symptoms, and the subject is asked to rate the severity of these symptoms on a 4-point scale, ranging from 0 to 3. It takes 5 to 10 minutes to complete. The score range is from a minimum of 0 to a maximum of 63; however, only in cases of very severe depression will scores of 40 or 50 be obtained. Typically, the scores for clinically depressed and maladjusted individuals range from 12 to 40. The items of the Beck Depression Inventory are primarily based on the observation and summarization of common attitudes and symptoms among depressed individuals. Since its development about 30 years ago, Beck's Depression Inventory has undergone extensive psychometric evaluation. A detailed analysis of various attempts to determine internal consistency has shown that the obtained coefficients range from 0.73 to 0.92, with an average of .86.
Evaluation of content, structural, and differential validity, as well as factor analysis, have generally yielded favorable results. The content of the Beck-II Depression Inventory was developed with the consensus of clinical experts regarding the pathological symptoms of depressed patients. It also includes six of the nine categories of depression diagnostic criteria according to the Diagnostic and Statistical Manual of Mental Disorders. In (X-COUNTRY), research conducted by Stefan-Dabson et al., which examined the Beck Depression Inventory in a large sample of patients with major depressive disorder, showed that the inventory can be reliably used to diagnose and measure the severity of depression both before and after treatment, and on multiple occasions (40). The results of factor analysis and validity assessments from this study support its suitability for evaluating the outcomes of any type of clinical trial. Specifically, by considering the three factors of depression, it is possible to identify the dimensions in which changes occur. According to the results of this research, the reliability coefficient of the Beck Depression Inventory for all 21 items is 0.91 (40).
3.4. The Fear of COVID-19 Scale
The Fear of COVID-19 Scale is a self-assessment tool developed by Ahorsu et al. to evaluate the symptoms of fear related to the viral disease COVID-19. This scale consists of 7 items. The scoring is based on a 5-point Likert scale, ranging from 1 (strongly disagree) to 5 (strongly agree). The lowest score for each subject is 1, and the highest score is 5. The total score is calculated by summing the individual responses, with a range of scores between 7 and 35. A higher score indicates greater fear of the Coronavirus (41). Ahorsu et al. measured this scale in a sample of 717 participants in (X-Country). The items on this scale were developed through an extensive review of existing fear scales, expert evaluations, and interviews with participants. According to the findings, the Pearson correlation coefficient of this scale ranged from 0.47 to 0.56. Additionally, the internal consistency was found to be 0.82, and the test-retest reliability was 0.72. The concurrent validity of the questionnaire was 0.42 with the Hospital Anxiety and Depression Scale and 0.11 with depression, while the validity with the scale of perceived vulnerability to disease, perceived infectivity, and aversion to germs was 0.48 and 0.46, respectively (41).
3.5. The Lockdown Fatigue Scale (LFS)
This scale was designed by Labragio and Balad to evaluate the symptoms of quarantine-related fatigue aimed at controlling the spread of the Coronavirus. The scale consists of 10 items, each answered on a 5-point Likert scale, ranging from "never" (1) to "always" (5). The highest possible score is 50. The score is classified into four levels of fatigue: Low fatigue (1 - 12), mild fatigue (13 - 25), moderate fatigue (26 - 37), and severe fatigue (38 - 50). The internal consistency of the scale is 0.84, the content validity is 0.93, and the retest reliability is 0.91.
In this research, the implementation method was individual. After obtaining consent from the patients within a specified period, the researcher provided the required information in the form of a questionnaire. Explanations were given to participants on how to complete the questionnaire, and after a set period, the completed questionnaires were collected from the patients and their companions. Throughout the study, the researchers ensured that all ethical considerations were followed, including the freedom of participants to choose whether or not to participate. Participants were also assured that their personal information would remain confidential during the study. The researchers took care to avoid any actions or activities that could endanger the health of the participants or others.
In the end, data analysis was conducted on 105 complete questionnaires. Descriptive statistics (mean and standard deviation) and inferential statistics (Pearson correlation and multiple regression) were performed using SPSS software, version 21.
4. Results
In this study, the sample consisted of 105 participants. Among them, 6 were male (approximately 6%) and 99 were female (approximately 94%). Regarding marital status, 5 participants were single (5%), 99 were married (94%), and 1 participant was divorced (1%). The age distribution of the participants was as follows: 20 participants were aged 18 - 25 years (19%), 35 participants were aged 26 - 30 years (33%), 32 participants were aged 31 - 35 years (31%), 16 participants were aged 36 - 40 years (15%), and 2 participants were aged over 41 years (2%).
In terms of education level, 55 participants had a diploma or sub-diploma education (52%), 41 had a bachelor's degree (39%), and 9 had a master's degree or higher (9%). Additionally, nearly 44% of the sample reported having a family history of heart disease.
Among the 105 participants with congenital heart disease, the majority were women (94.3%), married (94.3%), had a family diploma (43.8%), and did not have a family history of heart disease (56.2%). The largest group (33.3%) was in the age range of 26 - 30 years. The mean age of the participants was 30.35 ± 5.36 years. The detailed demographic information of the participants is presented in Table 1.
| Variables | No. (%) |
|---|---|
| Gender | |
| Female | 99 (94.3) |
| Male | 6 (5.7) |
| Age (y) | |
| 18 - 25 | 20 (19.0) |
| 26 - 30 | 35 (33.3) |
| 31 - 35 | 32 (30.5) |
| 36 - 40 | 16 (15.2) |
| ≥ 41 | 2 (1.9) |
| Marital status | |
| Single | 5 (4.8) |
| Married | 99 (94.3) |
| Divorced | 1 (1.0) |
| Education | |
| High school | 9 (8.6) |
| Diploma | 46 (43.8) |
| Bachelors’ degree | 41 (39.0) |
| Masters’ degree | 8 (7.6) |
| General Ph.D | 1 (1.0) |
| Family history of the disease | |
| Yes | 46 (43.8) |
| No | 59 (56.2) |
Demographic Information of the Participants
The descriptive characteristics of the research variables are presented in Table 2. Among the total participants, 20% (21 people) had low depression, 28.6% (30 people) had mild depression, 21.9% (23 people) had moderate depression, 21.9% (23 people) had relatively severe depression, and 7.6% (8 people) had severe depression. Regarding Coronavirus anxiety, 97.1% (102 people) did not experience dysfunctional anxiety related to the Coronavirus, while 2.9% (3 people) had dysfunctional anxiety, scoring 9 or above on the Coronavirus Anxiety Scale. These individuals had a significant clinical disorder due to their anxiety about the Coronavirus. The results of the Coronavirus fear scale indicate a moderately high average level of fear of the virus. In terms of quarantine fatigue, 24.8% (26 people) experienced high or severe fatigue, 26.7% (28 people) reported moderate fatigue, 43.8% (46 people) had mild fatigue, and 4.8% (5 people) reported low fatigue.
| Variables | Descriptive Indicators | Skewness | Kurtosis | |||
|---|---|---|---|---|---|---|
| Minimum - Maximum | Mean ± SD | Z Statistic | SE | Z Statistic | SE | |
| Depression | 0 - 24 | 10.42 ± 6.25 | 0.230 | 0.236 | -0.917 | 0.467 |
| Coronavirus anxiety | 0 - 15 | 1.56 ± 2.75 | 1.980 | 0.236 | 1.618 | 0.467 |
| Fear of the Coronavirus | 7 - 34 | 20.02 ± 5.99 | -0.336 | 0.236 | 0.037 | 0.467 |
| Quarantine fatigue | 11 - 50 | 27.39 ± 10.69 | 0.234 | 0.236 | -1.262 | 0.467 |
Descriptive Results of Research Variables
To investigate the relationship between fear of the Coronavirus, depression, and Coronavirus anxiety with quarantine fatigue, Pearson's correlation coefficient was used. The use of this test requires certain assumptions, which were examined prior to conducting the inferential analysis. One of these assumptions is the normality of the distribution of the research variables, which was assessed using the Skewness and Kurtosis indices. The values of Skewness and Kurtosis fall within the range of (-1.96, 1.96), indicating that the research variables are normally distributed and their distribution is symmetrical (Table 2). The second assumption is that the relationship between the criterion variable and predictor variables is linear when all other predictor variables are held constant. The significance level of the F-test, used to assess the linearity of the relationship between the predictor variables and the criterion, was smaller than the predetermined alpha value (α = 0.05). This result confirms the linearity of the relationship between the variables under investigation. Another assumption of regression analysis is the absence of high correlation between predictor variables (i.e., linear multicollinearity), which was examined using two statistics: Tolerance and the variance inflation factor. Data analysis showed no evidence of linear multicollinearity between the independent variables, as the tolerance values were close to one, and the variance inflation factor was below two. Therefore, since the assumptions for both the correlation test and regression analysis were met, it is appropriate to use these tests to examine the research hypotheses.
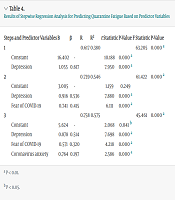
The results of the Pearson correlation test (Table 3) showed a positive and significant correlation between fear of the Coronavirus (r = 0.520, P = 0.001), depression (r = 0.617, P = 0.001), and Coronavirus anxiety (r = 0.466, P = 0.000) with quarantine fatigue. Additionally, to determine the role of fear of the Coronavirus, depression, and Coronavirus anxiety in predicting quarantine fatigue, a stepwise regression analysis was conducted (Table 4).
| Steps and Predictor Variables | B | β | R | R2 | t Statistic | P-Value | F Statistic | P-Value |
|---|---|---|---|---|---|---|---|---|
| 1 | 0.617 | 0.380 | 63.205 | 0.000 a | ||||
| Constant | 16.402 | - | 10.188 | 0.000 a | ||||
| Depression | 1.055 | 0.617 | 7.950 | 0.000 a | ||||
| 2 | 0.739 | 0.546 | 61.422 | 0.000 a | ||||
| Constant | 3.005 | - | 1.159 | 0.249 | ||||
| Depression | 0.916 | 0.536 | 7.880 | 0.000 a | ||||
| Fear of COVID-19 | 0.741 | 0.415 | 6.111 | 0.000 a | ||||
| 3 | 0.758 | 0.575 | 45.461 | 0.000 a | ||||
| Constant | 5.624 | - | 2.068 | 0.041 b | ||||
| Depression | 0.878 | 0.514 | 7.698 | 0.000 a | ||||
| Fear of COVID-19 | 0.571 | 0.320 | 4.218 | 0.000 a | ||||
| Coronavirus anxiety | 0.764 | 0.197 | 2.586 | 0.000 a |
Results of Stepwise Regression Analysis for Predicting Quarantine Fatigue Based on Predictor Variables
The results of the stepwise regression analysis show that, in the first step, the variable that entered the analysis and remained was depression, indicating that this variable had the greatest effect compared to the other predictor variables. In stepwise regression analysis, the final step is usually considered the basis of the analysis. In the third step, Coronavirus anxiety was entered into the analysis as the last variable. The correlation coefficient calculated in this step was 0.758, and the coefficient of determination was 0.575. The F value obtained indicates that the calculated regression model is significant at the 99% confidence level. According to the calculated coefficient of determination, 56% of the variance in quarantine fatigue can be explained by the three predictor variables: Depression, fear of the Coronavirus, and anxiety.
Furthermore, in the secondary results of the study, the variables of fear of COVID-19, depression, Coronavirus-related anxiety, and quarantine fatigue were analyzed as dependent variables based on age, marital status, education, and gender using multivariate analysis of variance (MANOVA). The results showed no significant differences based on age (F = 1.25, df = 4, P > 0.05), marital status (F = 0.81, df = 24, P > 0.05), education (F = 0.34, df = 4, P > 0.05), or gender (F = 0.95, df = 1, P > 0.05).
5. Discussion
The present study aimed to investigate the predictive role of fear of COVID-19, depression, and coronavirus anxiety on quarantine fatigue in patients with congenital heart disease. The research findings regarding the relationship between the variables indicate a significant positive correlation between fear of COVID-19, quarantine fatigue, and depression in heart patients. Among the research variables, depression symptoms, fear of COVID-19, and coronavirus anxiety had the most explanatory power in predicting quarantine fatigue in congenital heart patients. Although there are studies that have not directly examined the effects of these variables on quarantine fatigue in congenital heart disease patients, the results of the present study are consistent with the findings of Yang et al., Li et al., Chen et al., Mazza et al., and Santini et al. (4, 12, 16-18).
In relation to the role of depression symptoms in predicting chronic fatigue caused by COVID-19, it can be concluded that one of the factors that increases the risk of depression during the coronavirus period is the feeling of losing control over one's life. The presence of stressors during the COVID-19 era, reduced physical mobility, limited social support, and lack of access to standard stress-coping solutions, such as psychological, religious, and sports interventions, can exacerbate this risk. Additionally, factors like job loss and other responsibilities can transform the risk of depression into a stressor through the loss of control over life (42). In other words, during the spread of the virus, a person's routine is disrupted, making it harder to predict or plan for the future. People feel their control over life is diminished, which leads to feelings of insecurity. This lack of security generates anxiety, which in turn creates negative consequences in the form of quarantine fatigue (43).
Moreover, during the coronavirus outbreak, changes in people's social and personal lives, driven by critical conditions, values, and social goals, can contribute to quarantine fatigue. For instance, isolation and quarantine can result in increased fatigue (44). On the other hand, individuals in quarantine due to COVID-19 may lose psychological support from family and friends, increasing pressure and depression, which can further contribute to quarantine fatigue (26). Additionally, during quarantine, people might develop ineffective beliefs about health and illness, making incorrect and catastrophic interpretations of their feelings and physical changes. This can lead to an increase in depression, which affects their ability to make decisions on how to manage the disease (45) and consequently results in higher levels of quarantine fatigue.
Another finding of the present study showed that fear of the coronavirus disease has a significant relationship with quarantine fatigue in heart patients. In explaining the connection between fear of the coronavirus and quarantine fatigue, it can be pointed out that the COVID-19 pandemic, as both an individual and social crisis, causes stress and fear of illness in individuals and society. This fear threatens mental health, disrupts the quality of interpersonal relationships within families, and leads to feelings of social rejection (35). Studies have shown that people who follow news related to the coronavirus experience more fear and anxiety, and these news stories and rumors within society can amplify anxiety both at the individual and societal levels. Fear of getting sick, economic and job-related problems due to quarantine, temporary or permanent unemployment, limited social interactions, uncertainty about the end of the pandemic, concern for family and friends, and fear of the future are among the psychological effects of the coronavirus that contribute to quarantine fatigue and the stress associated with it (27). On the other hand, during the coronavirus epidemic and in the absence of a definitive treatment for the disease, people experienced heightened fear and confusion. Therefore, individuals who cannot use optimal coping strategies to manage these emotions may interpret even the slightest symptoms as signs of infection, leading to high levels of stress and anxiety about the coronavirus. This, in turn, can contribute to the onset of quarantine fatigue (46).
In other words, during the COVID-19 epidemic, the media and the environment have emphasized the issues surrounding this disease and compliance with health guidelines, as bodily sensations and their interpretation can be influenced by environmental factors. The increasing concerns about health, anxiety, and the fear of contracting the disease lead to heightened anxiety related to the coronavirus (47). Therefore, much emphasis on worrying topics focuses people's attention, and this focus on traumatic aspects can lead to anxiety in individuals (48). The more these traumatic issues are related to human health and endanger a person's life, the more they attract attention and cause increased anxiety (4). As a result, when people experience symptoms such as stress and fear due to the spread of the coronavirus during the pandemic, they feel more afraid and worried and tend to follow the news related to COVID-19. Consequently, due to the fear of infection and constant exposure to coronavirus-related news, they experience greater anxiety. Therefore, it is logical that fear of the coronavirus can predict quarantine fatigue (49).
In explaining the role of coronavirus anxiety in quarantine fatigue, it can be noted that one of the factors related to quarantine fatigue is the quality of life experienced by patients during the outbreak of COVID-19. An excessive increase in anxiety due to COVID-19 in some individuals weakens the body's immune system in dealing with the disease and can even affect people's rational decision-making and social behavior. Severe levels of anxiety are associated with catastrophizing physical changes, engaging in maladaptive coping behaviors, and causing distress, social disability, and disruptions in work performance, which often lead to frequent visits to medical centers. This, in turn, results in a reduction in the quality of life and increased quarantine fatigue, particularly in heart patients (50). People with low anxiety about COVID-19 may also engage in various non-adaptive behaviors, such as excessive hand washing, social withdrawal, and panic shopping (51), which can significantly contribute to quarantine fatigue. On the other hand, anxiety caused by COVID-19 disrupts health outcomes, such as physical complaints, domestic participation, and career progress, due to increased emotional suppression and failure to satisfy psychological needs (52). All these factors lead to a decrease in people's quality of life, which can exacerbate quarantine fatigue. In general, the results of the present study showed that patients with congenital heart disease experienced high levels of quarantine fatigue, anxiety, depression, and fear of COVID-19.
An examination of the research literature indicates that studies have been conducted regarding the relationship between research variables and the level of quarantine fatigue. This study investigated and highlighted the predictive role of fear of COVID-19, symptoms of depression, and COVID-19-related anxiety on quarantine fatigue in patients with congenital heart disease. Therefore, training and interventions aimed at addressing the psychological consequences of COVID-19—specifically to reduce depression, anxiety, and fear of contracting the virus—have shown positive results. These programs can be considered preventive measures to help individuals overcome the quarantine fatigue they experience.
Among the limitations of this research was its implementation in patients hospitalized at Shahid Rajaei and Heart Hospitals in (X-Country). Therefore, the generalization of the results to patients hospitalized at home or those suffering from other types of diseases should be done with caution. Another limitation is that this study was conducted at a single point in time, and the researchers did not have control over recent events in the patients' lives. It is suggested that future studies be conducted longitudinally with a larger sample size.
Because the available sampling method was used in this research, the generalizability of its results should be approached with caution. Therefore, it is recommended to use a random sampling method in future studies to enhance the generalizability of the findings among patients with congenital heart disease. Additionally, the data for this study were collected using a questionnaire. Future research could benefit from using other measurement methods, such as semi-structured interviews, continuous observations, or other qualitative approaches.
It is also suggested to develop an intervention program focused on introducing preventive measures related to COVID-19 anxiety to reduce fear and anxiety about contracting the virus. Furthermore, educating patients on adaptive strategies for dealing with the disease during this era and the positive outcomes of such strategies could also be part of prevention programs to help people manage the psychological impact of COVID-19.
Finally, it is recommended to conduct studies on physical, social, and spiritual care in patients with heart disease during specific stages of their condition, particularly during the COVID-19 pandemic, to further advance our understanding of this subject.
