


1. Background
Today, the central role of the physician-patient relationship has been proven in the successful delivery of primary health care and in the efficiency of medical services. Also, studies have shown that having an effective relationship not only helps the patient to feel better, but also helps to restore the patient's complete health. On the other hand, establishing an effective relationship between physician and patient often leads to increased physician job satisfaction (1).
Basically, the physician's relationship with the patient is formed when the patient consciously demands the physician's services and the physician consciously accepts him as a patient. This bilateral communication, consent-based relationship is often described as a contractual relationship. The formation of this relationship means the imposition and obligation of a series of legal duties and requirements (and moral and professional), and therefore understanding the time of the beginning and end of this relationship is very important (2).
In general, researchers' studies show that establishing an appropriate relationship between physician and patient is a key element in patient and (even physician) satisfaction and it is very effective in attracting patient cooperation to follow treatment instructions and patient participation in the treatment process and the reception of treatment plans (3). In this study, while introducing the concept of physician-patient relationship and how it is formed in the context of time, an attempt has been made to introduce and compare the models in physician-patient relationships and the most obvious strengths and weaknesses of each communication model should be introduced and finally we can achieve an effective communication-cultural model.
1.1. Emmanuel Communication Models
In 1992, Emmanuel described five models of physician-patient communication that since, they have been referenced in many other articles (4). They believe that in the last two decades there have been extensive discussions about the patient's role in treatment decisions in order to put an end to the conflict between autonomy and patient health and the patient's personal values towards therapeutic values. In this regard, in defining the ideal physician-patient relationship, Emanuel has presented five models based on understanding the goals of physician-patient interaction, physician requirements, the role of patient values and the concept of his autonomy, which are summarized below:
1.1.1. Patriarchal Model
In this model, the physician-patient relationship is such that to ensure the patient receives the best therapeutic intervention to promote his health. In this regard, physicians use their skills to determine the patient's medical condition and diagnose the best tests and treatments. They then present a set of "selected information" to the patient and encourage him to accept the intervention that the physician considers best. In this model, the physician with full force announces the start time of the intervention. What is chosen between the patient's autonomy and recovery, or between the patient's value choice and his health, is recovery and return his health. In fact, in this model, it is the physician who determines the end and the means to an end. Just as the "father knows best," it is the physician who sets and guides goals, despite the fact that goals such as health, salvation, or beauty are very private and very personal matters (5).
The active-passive Hollander model, which is based on the severity of the disease (acute, non-acute, and chronic), is essentially patriarchal and very similar to the parent-young child relationship. In this model, the patient is like a helpless person who seeks the specialized knowledge of a physician. Treatment is something higher than the patient and his role and is done regardless of the outcome. This model can be justified only in acute or emergencies cases (6).
The most important ethical principle in the Veatch's Priest model is the principle of "profit and do not harm the patient." In this model, the physician is considered a worthy human in medical science as well as toward the values and beliefs that shape patients' treatment choices (5). Ozar organizational communication model can also be included in this group. What prevails in this model is the medical profession (7). In this model, there is a clear distinction between professionals (knowledgeable and skilled) and ordinary people. Although the patient and his needs form the basis of the medical profession, the patient in this model is passive, receptive and inactive. Because he is not educated, he has no skills and therefore he is uninformed. Thus, although the needs that are met are patient-related, it is in fact the physician who determines what the patient needs. The assumption of this model is that patients do not have the ability to understand the information needed to make decisions about health care related to their body and therefore, they have assigned this task to doctors. The role of patients in this model is only to provide an accurate report of the facts (their experience) (8).
Interpretive model: The purpose of the physician-patient relationship in this model is to clarify the patient's values and what he really wants. In the interpretive model, the patient is helped to choose from the available interventions the one that implements his values. The role of the physician here is similar to the informational model, with the difference that the physician, in addition to the role of the informant, tries to interpret and clarify the patient's values for the patient and therefore the doctor tries to involve the patient in the joint process of understanding his values with the doctor. Therefore, in this model, the patient's values are not necessarily fixed and known to the patient, rather, it is often undeveloped and the physician must be enlightened in aligning these values with the patient, and ultimately, the physician determines the best interventions and tests that are consistent with the patient's values. It should be noted that in this model, it is not the physician who dictates, but the patient who ultimately determines which values and treatment process best align with his true personality. Also, the physician will not make any judgments about the patient's values, but will help him to understand his values and apply them in the medical context. Therefore, the physician is a consultant in this model. Also, in this model, autonomy means self-understanding. This means that the patient comes to know who he is and how different treatment options are based on his identity.
1.1.2. Informative Model
Scientific model, engineering model and customer-oriented model are other names that are used for the informational model. In this model, the purpose of the physician-patient relationship is that the physician provides all the relevant information and the patient chooses the desired treatment intervention based on the best compliance with his values, and then the physician performs the selected intervention.
In fact, in this model, physicians, instead of considering themselves as primary service providers of the patient, they have found themselves as servants of science (5). Thus, there is a clear distinction between facts and values, in the informative model. The patient's values are well defined and what the patient does not have are the clinical facts. The facts that the physician is responsible for providing them and is one of his requirements. In this model, there is no place for the physician's values, his understanding of the patient's values, or his judgment of the patient's values. The physician provides specialized techniques and conditions by which the patient can exercise control. The concept of patient autonomy in this model is control over medical decisions. In his engineering model, Veatch sees the physician as a plumber who, in addition to repairs, also connects the pipes without considering other relevant information - the constructive conversations that the patient needs to make decisions about his care. The physician in this model lacks moral integrity (7).
Instrumental model: In this model, patient values are irrelevant. The doctor's goal is somewhere beyond the patient, and sometimes the patient sacrifices for it. For example, it deals with a larger goal such as society or the achievement of scientific goals. Tuskegee and Willow Druck's studies are examples of the implementation of this model (9).
In the instrumental model, the patient is assumed to have no autonomy and an attempt is made to prevent the patient from attempting anything that goes against the pre-selected main goal of the physician-patient relationship. The physician's attention to the patient is only to achieve something outside the patient; at the same time, the patient may or may not benefit from this relationship (10). In this communication model, the patient has no choice but to accept only the treatment that the doctor has chosen for him. As mentioned, this communication model is often realized during biomedical research and can have a research-therapeutic nature.
1.1.3. Consultative Model
The purpose of physician-patient communication in this model is to help the patient to determine and select the best health-related value, so that it is most effective in clinical settings. The physician's role is to draw information about the patient's clinical condition and then to help clarify a variety of values that are rooted in existing treatment options. The highest level of this model is where the physician and the patient engage in an idea of what health-related values the patient can and ultimately pursue.
In the counseling model, the physician speaks only of values that have affected the patient's health or have been affected by his or her condition. In fact, the physician's intention is nothing but to persuade the patient morally, and his role is the role of a friend or teacher who engages the patient in a conversation about which path to take. In this model, the physician not only shows what the patient can do, but also tells the patient what is the best act and so shows what the patient should do and which treatment decision is commendable (1).
1.2. Theoretical Literature
Among the various models and theories that have been proposed for the physician-patient relationship, Foucault's model specifically analyzes the physician-patient relationship. In his theory, Foucault refers to the influence of the physician-patient relationship on the structure of general society. Because the structure of the disciplinary society, in order to improve its supervision over the activists of the society, uses medical science and the power of examination and accurate knowledge of the physician in order to establish order. Thus, for Foucault, the physician-patient relationship is not based on attention to the patient's needs and a comprehensive understanding of his condition. The physician and the patient experience a relationship with a conflict of interest and goals that ultimately leads to patient dissatisfaction (11).
Another effective theoretical model is the Goffman model. In his theories, Goffman often refers to the analogy of the interaction scene between individuals and the theater scene, in which human actors play roles like actors. According to Goffman, the physician and the patient evaluate each other's behavior in the first encounter, and based on this evaluation, they decide to continue the relationship and, if the relationship continues, what strategies to adopt or end the relationship. In fact, according to Goffman, patients' performance in relation to the physician is based on their assessment of the relationship and is unique. Patients' interests can be side by side or in conflict with the doctor (12).
2. Methods
The research method used in this descriptive study is correlation and using the calculated correlation coefficients, he has developed a structural model. The statistical population of this study is all patients admitted to medical centers affiliated to Kermanshah University of Medical Sciences and Health Services in 2019, from which 171 were selected as a sample. Inclusion criteria in the study include patients who have been hospitalized for at least two days. The sample size was determined using Cochran's formula. Because the statistical population is unknown and the value of p is also unknown, the value of p was considered 0.5. Therefore, according to the formula, the number of samples (z = 1.96, pq = 0.5 and d = 0.075) was calculated to be 171. One of the sampling methods that in some cases is more appropriate than other methods is the available sampling method which is used in this research.
In this study, a questionnaire was used. Vakili and colleagues' standard questionnaire for communication with patients, to assess interpersonal communication skills and a researcher-made questionnaire for observing physician ethics and patient satisfaction taken from the charter of Patients' Rights approved by the Ministry of Health that are asked patients or their companions .
Formal validity and content validity were considered to examine the validity in the present study. In order to achieve the content validity and formal validity of the measuring instrument, before the implementation, the validity of the instrument was checked by the opinion of relevant experts and researchers as well as knowledgeable people, and this process continued to some extent until the researcher achieved the desired validity. The analysis of test data was done in two descriptive and inferential categories. Data analysis was performed in two main stages: (1) descriptive analysis of data; (2) analytical analysis of data, first the information obtained from the questionnaires was extracted and adjusted in the general information table. Then all the data are analyzed by computer and through SPSS (20.0) software, smartPLS3 in two parts of descriptive and analytical methods. In descriptive analysis, after describing the demographic variables, the scores obtained from the implementation of research questionnaires are calculated and reported and at the analytical level, the data analysis is performed using independent and paired t-test, Pearson correlation and analysis of variance with SPSS software.
Cronbach's alpha coefficient is estimated to determine the reliability of the questionnaire. In this study, Cronbach's alpha results showed that the reliability of the questionnaire was appropriate.
| Questionnaire | Cronbach's Alpha |
|---|---|
| Vakili | 0.7 |
| Observance of medical ethics of physician | 0.7 |
Based on the results of Table 1, it is clear that the reliability of the internal consistency method and the calculation of Cronbach's alpha for the Vakili's standard questionnaire of communication with the patient and the questionnaire of medical ethics is 0.7, which indicates the appropriateness of the questionnaires.
3. Results
Among the 171 patients participating in this study, 52% are women and 48% are men. 65% were married and 68% were over 30 years old. 8% of them had a master's degree and 48% had a lower than diploma degree. Regarding the correlation between the research variables, the results showed that the correlation between the functional or role-oriented model with the relationship with the patient was negative and equal to -0.167. The correlation between patriarchal model and patient relationship was 0.158. The correlation between the informative model and the patient relationship was 0.332. The correlation between the interpretive model and patient relationship was 0.306 and the correlation between the consultative model and patient relationship was 0.457. The correlation between instrumental model and patient relationship was not significant. The correlation between the bilateral participation model and the relationship with the patient was 0.329 and the correlation between the contract model and the relationship with the patient is -0.278. The correlation between the detailed model and patient relationship was -0.275.
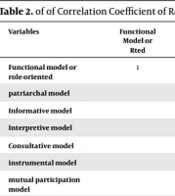
Investigating the linear relationship between predictor and standard variables. Pearson correlation has been used to investigate the relationship between predictor and standard variables. The results indicate that there is a correlation between research variables and standard variable. Therefore, the first hypothesis has been observed (Table 2).
| Variables | Functional Model or Rted | Patriarchal Model | Informative Model | Interpretive Model | Consultative Model | Instrumental Model | Mutual Participation Model | Contractual Model | Detailed Model | Communication with the Patient |
|---|---|---|---|---|---|---|---|---|---|---|
| Functional model or role-oriented | 1 | -0.121 | -0.299** | -0.327** | -0.293** | 0.122 | -0.066 | 0.252** | 0.371** | -0.167* |
| Patriarchal model | 1 | 0.204** | 0.279** | 0.348** | 0.046 | -0.007 | -0.021 | 0.147 | 0.158* | |
| Informative model | 1 | .545** | 0.678** | -0.368** | 0.342** | -0.165* | -0.329** | 0.332** | ||
| Interpretive model | 1 | 0.668** | -0.066 | 0.416** | -0.131 | -0.191* | 0.306** | |||
| Consultative model | 1 | -0.174* | 0.428** | -0.267** | -0.282** | 0.457** | ||||
| Instrumental model | 1 | 0.071 | 0.342** | 0.134 | -0.104 | |||||
| Mutual participation model | 1 | -0.092 | -0.244** | 0.229** | ||||||
| Contractual model | 1 | 0.373** | -0.287** | |||||||
| Detailed model | 1 | -0.275** | ||||||||
| Communication with the patient | 1 |
Regarding the correlation between the research variables, the results showed that the correlation between the functional or role-oriented model with the patient relationship was negative and equal to -0.167. The correlation between patriarchal model and patient relationship was 0.158. The correlation between the informative model and the patient relationship was 0.332. The correlation between the interpretive model and patient relationship was 0.306 and the correlation between the consultative model and patient relationship was 0.457. The correlation between instrumental model and patient relationship was not significant. The correlation between the bilateral participation model and the relationship with the patient was 0.329; and the correlation between the contract model and the relationship with the patient is -0.278. The correlation between the detailed model and the relationship with the patient was -0.275.
4. Discussion
Some factors affect the quality of the physician-patient relationship and help to increase the effective physician-patient relationship. One of these factors is the type of communication model between physician and patient. Patient satisfaction with the type of relationship can largely indicate the proper performance of services.
Based on the results, it was found that the patriarchal model was able to predict patient satisfaction with an effect coefficient of 0.13 and a significance level of P < 0.01. Therefore, the research hypothesis was confirmed that "there is a significant relationship between patriarchal model and patient satisfaction". The research hypothesis was also confirmed that "there is a significant relationship between counseling model and patient satisfaction". This hypothesis was also confirmed that there is a significant relationship between the contract model and patient satisfaction.
However, based on the results, it was found that the interpretive model could not predict patient satisfaction with a coefficient of effect of 0.07. Therefore, the research hypothesis was rejected that "there is a significant relationship between the informative model and patient satisfaction". The interpretive model could not predict patient satisfaction with an effect factor of 0.035. Therefore, the research hypothesis that was rejected "there is a significant relationship between the interpretive model and patient satisfaction". Therefore, the research hypothesis was rejected that "there is a significant relationship between instrumental model and patient satisfaction". Based on the results, it is clear that the bilateral participation model could not predict patient satisfaction with an effect factor of 0.083. Therefore, the research hypothesis is also rejected that "there is a significant relationship between the model of mutual participation and patient satisfaction".
Today, efforts are made to make the patient the main focus of the treatment process and to provide all medical services for him. Therefore, patient satisfaction can largely indicate the correct performance of services; Satisfaction that does not come from high technology alone but also the behavior of staff and their performance is very important. The needs, expectations, expectations and experiences of the patient from receiving health services are manifested in the complex phenomenon of satisfaction with the treatment process. Satisfaction of the patient indicates that the healthcare staff is aware of the importance of responding to the patient's biological and psychological and social needs and feel responsible for it. The result of patient satisfaction from treatment process is the patient's trust in the treatment system. The patient's trust is manifested in his cooperation with the physician, and the cooperation that is demonstrated through the acceptance and implementation of the physician's instructions leads to the faster recovery of the patient and his return to society. But as it was obvious in proving the hypotheses, the relationship between the three models of patriarchy, contractual and consultative were models that had a meaningful relationship with patient satisfaction in this study. In all three models, the relationship between physician and patient is weak and only the treatment of the disease is considered by the physician and the relationship with the patient is not important and the final decision is with the physician. The patient does not interfere in the physician's decision during treatment. Medicine is more a business than a profession. You feel that the doctor is higher than you.
Physician-patient interactions are a complex process, and inappropriate communication can become a problem, especially when it comes to the patient's knowledge of the disease, how to care, motivation, and hope and advance the treatment process (13). Today, in developed countries, the dominant pattern of communication is the exchange of information, and the health consumer movement has led to the prevalence of participatory decision-making and patient-centered communication patterns (14).
One of the characteristics of a good model is its originality in the base, its flexibility and comprehensiveness, and its obstruction. To achieve this goal, the foundation of an efficient model must be properly selected and its intellectual framework must induce flexibility, comprehensiveness and barrier in its structure. Proposed models such as the suggested models (Zass, Emmanuel AJ, Hollander, etc.), which are based on disease, patient autonomy, etc., have an originality based on empirical observations and have not provided appropriate learning (15). The proverb that not everyone can be driven with one stick. Or the phrase: there is no need for new models, just ask the patient indicates the inefficiency of single models in providing a comprehensive and barrier communication model (16). It is undeniable that any physician-patient relationship is unique in terms of the form of communication, the purpose of the relationship, the effectiveness of each encounter between physician and patient, and the specific expectations of the parties to each other. In addition, each of these dimensions varies in different cultures and time periods. Therefore, most of the introduced models are related to culture and history. Also, unequal clinical background and conditions have been effective in their design. Therefore, basically, these communication models should be considered as dynamic models that depend on the culture and conditions of the society that produces them; and so it can be concluded that they will not be universally easily. Therefore, it is necessary for Islamic societies to design and explain their own communication model. The need for one or more models of efficient Islamic communication is fully felt to be implemented in the culture and form of Islamic societies. It is obvious that such a model is no exception to the above rule and can be studied and implemented only in the form of the doctrine of Islam. Because the basis of this model requires the acceptance of Islamic principles and sub-principles.
But medical centers in Iran can be divided into three categories: (1) public, (2) private, and (3) semi-private. Doctors, nurses and all medical personnel in public health centers such as hospitals and educational clinics, due to the support and backing that the government provides in line with its social policies to protect, preserve and establish the rights of individuals in society, each one is considered a kind of government employee. Compared to those who work in the private sector, these people have unique characteristics that have the potential to affect the physician-patient relationship.
Also, most of the patients referred to government health centers are from middle and lower levels of society. Although there are several reasons for these groups to go to government centers, it can be argued that the high cost of treatment in the private sector is one of the most important reasons for people to go to government centers. Therefore, considering the above factors and other special reasons that guide people to choose to refer to these centers, it can be concluded that one of the dominant features of patients' visits to these centers is the definite receipt of one of the government health services. Therefore, it can be assumed that referrals that are only for information or consultation only about a disease or possible treatment options (although much less common in private centers), are significantly more lower in government centers.
4.1. Limitations Available to the Researcher
- One of the most important limitations of this study was the lack of cooperation of some patients in filling out the questionnaire. Due to the dangerous condition of the corona and the impatience of some patients, some of them were reluctant to cooperate.
Lack of cooperation of hospital staff and restrictions on the distribution of questionnaires in coronary conditions were other limitations of this study.
- Restriction of access to the statistical community: Usually, patients were not always present in the hospitals and I had to go to the hospital for several days to fill in the questionnaire, which was not easy to coordinate with the patients and the hospital staff.
- Bureaucracy and high strictness in the distribution of questionnaires in hospitals were other problems in the research.
- Researcher time limit.
