




1. Background
Universities are pivotal social settings for young adults, fostering romantic relationships during a developmental phase characterized by heightened emotional needs and the pursuit of stable partnerships (1). The termination of these relationships can trigger love trauma syndrome (LTS), a condition marked by acute psychological symptoms that impair functioning across multiple domains (2). The LTS encompasses hyperarousal, avoidance, intrusive memories, and emotional dysregulation, reflecting the profound distress tied to romantic breakups (3). This study uniquely examines LTS by directly comparing two therapeutic interventions, highlighting a novel contribution to addressing its psychological impact among university students.
Research by Rosner et al. delineates LTS’s multifaceted symptoms, including affective (e.g., sadness, distress), separation-related (e.g., intrusive thoughts, yearning), and cognitive (e.g., reduced self-esteem, impaired trauma processing) manifestations (4). Davis et al. suggest that LTS elicits grief, depression, anger (5), and core insecurities, with del Palacio-González et al. noting prevalent symptoms like depressive affect, anger, and somatic complaints (6). These emotional sequelae underscore the necessity of effective emotion regulation to mitigate LTS’s impact (7). Impaired emotion regulation often exacerbates negative affective states, fostering learned helplessness and reducing adaptive coping (8).
Emotion regulation is closely linked to distress tolerance, defined as the ability to endure aversive psychological states (9). Individuals with low distress tolerance perceive emotions as intolerable, resist acceptance, and avoid negative feelings, resulting in functional impairments (9). Conversely, high distress tolerance supports adaptive emotional regulation, reducing maladaptive responses (10). The LTS, as a significant stressor, frequently precipitates psychological distress, particularly among young adults, with varied responses ranging from resilience to mood and functional impairments. Enhancing distress tolerance is thus critical for alleviating LTS’s adverse effects. Within the studied cultural context, individuals experiencing LTS often hesitate to disclose their struggles due to social and familial constraints, potentially leading to alexithymia — difficulty identifying and expressing emotions — and reduced distress tolerance (11). The high prevalence of LTS among students, combined with its physical and psychological toll, underscores the urgency of targeted interventions. This study’s novelty lies in its direct comparison of therapeutic approaches to address these culturally nuanced challenges, filling a gap in the literature.
Cognitive behavioral psychodrama group therapy (CBPGT) integrates cognitive-behavioral and psychodramatic techniques to address maladaptive patterns and foster positive experiences (12). Structured in warm-up, enactment, and sharing phases, CBPGT employs cognitive strategies to identify distortions, role-playing to explore negative cognitions, and reflective sharing to process experiences (13). Its group setting promotes experiential learning and emotional exposure (14, 15). Reality therapy, conversely, enhances distress tolerance by emphasizing reality confrontation, personal responsibility, and adaptive choices (16). It focuses on present-oriented moral evaluations and internal control, applicable to diverse behaviors (17-19). Firozi and Vakili demonstrated its efficacy in improving coping and reducing rumination (20).
No prior studies have directly compared CBPGT and reality therapy for LTS, despite their potential to address its emotional and cognitive challenges. This research fills this gap by evaluating their relative efficacies, offering new insights into optimizing interventions for university students. By examining culturally influenced barriers, such as limited disclosure and support, this study underscores the necessity of tailored therapeutic approaches to enhance distress tolerance and emotional regulation, advancing both clinical practice and research on LTS.
2. Objectives
This research explored the potential of CBPGT and reality therapy, to ameliorate deficits in distress tolerance among students displaying symptoms of love trauma.
3. Methods
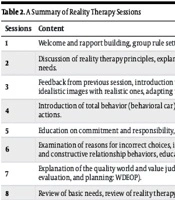
This study employed a quasi-experimental design with a pre-test, post-test, and two-month follow-up protocol, incorporating a control group. The target population consisted of university students in Najafabad during 2023 exhibiting symptoms of LTS. A sample size of 45 participants was determined using G*Power software, based on a significance level of α = 0.05, a power of 0.90, and an expected medium effect size, ensuring adequate statistical power. Participants were recruited via convenience sampling, meeting specific inclusion criteria, and randomly allocated to three groups (n = 15 each) using a computer-generated random number sequence to ensure unbiased assignment: Two experimental groups and one control group. The first experimental group received an 8-week CBPGT intervention, comprising weekly 90-minute sessions. The second experimental group underwent an 8-week reality therapy intervention, also with weekly 90-minute sessions. Session durations were consistently 90 minutes across both interventions, as detailed in Tables 1 and 2, which summarize CBPGT and reality therapy session content. The control group participated in weekly 90-minute unstructured discussion sessions focused on general university life, without therapeutic components, to control for social interaction effects. A two-month follow-up assessment evaluated the durability of intervention effects. Inclusion criteria included a score below 20 on the Ross Love Trauma Scale, selected as the cutoff based on Ross’s validation study indicating mild to moderate LTS symptoms, ensuring relevance to the study’s focus; enrollment in university for at least two semesters; age between 18 - 25 years; no diagnosed mental or physical disorders; and provision of informed consent. Exclusion criteria included absence from more than two intervention sessions. Fidelity to CBPGT and reality therapy protocols was ensured through therapist training, adherence to manualized session plans, and weekly supervision by certified psychologists, with 20% of sessions randomly audited for protocol compliance.
| Sessions | Content |
|---|---|
| 1 | Welcome and group preparation, member and leader introductions, discussion of confidentiality principles, treatment structure and techniques education, explanation of emotional breakup concept and harms, introduction to ATR and DTR forms, and recommendation of self-help book reading. |
| 2 | Discussion of completed ATR and DTR forms, introduction to CBT concepts (core beliefs, cognitive distortions, negative automatic thoughts), discussion of alexithymia, emotional regulation, stress, distress tolerance, explanation of psychodrama, and conducting a practice model. |
| 3 and 4 | Review of assigned homework, discussion of challenging situations, explanations of emotions and feelings, protagonist selection, warm-up activities (ATR, genogram, auxiliary ego selection), use of hot seat and monologue techniques, relaxation practice, psychodrama enactment, and processing group dynamics. |
| 5 and 6 | Discussion of stressor components, explanation of affective and emotional alexithymia, assessment of readiness to be a protagonist, ATR completion, exposure practice, genogram completion, use of double, role reversal, and future projection techniques, psychodrama enactment, and group participation. |
| 7 and 8 | Review of social skills, review of automatic thoughts and intermediate beliefs, review of cognitive distortions, discussion of member experiences, ensuring resolution of issues, discussion of concept forgetting, therapist report, Q &A, and post-test administration |
Abbreviations: ATR, automatic thought record; DTR, dysfunctional thought record; CBT, cognitive-behavioral therapy, Q &A, question and answer.
| Sessions | Content |
|---|---|
| 1 | Welcome and rapport building, group rule setting, member introductions, assessment of member needs, presentation of session structure and goals. |
| 2 | Discussion of reality therapy principles, explanation of 5 basic human needs, needs assessment in members, examination of member attitudes towards basic needs. |
| 3 | Feedback from previous session, introduction to the quality world, reassessment of needs, education on the difference between real and quality worlds, replacing idealistic images with realistic ones, adapting to the external world. |
| 4 | Introduction of total behavior (behavioral car) and its components, education on evaluating behavior effectiveness, assistance in evaluating current behavior actions. |
| 5 | Education on commitment and responsibility, planning responsible behaviors. |
| 6 | Examination of reasons for incorrect choices, introduction of external and internal control psychology, understanding four conflicts, introduction of destructive and constructive relationship behaviors, education on assessing destructive behaviors. |
| 7 | Explanation of the quality world and value judgment system, education on the comparison place, education on responsible planning method (wants, doing, evaluation, and planning: WDEOP). |
| 8 | Review of basic needs, review of reality therapy concepts, review of problem-solving skills, discussion of goals and achievement, post-test administration. |
Abbreviation: WDEOP, wants, doing, evaluation, and planning.
3.1. Instrument
The Distress Tolerance Scale is a self-report questionnaire developed by Simons and Gaher in 2005. The items of this scale assess distress tolerance based on an individual's abilities to endure emotional distress, cognitive appraisal of distress, the degree of attention to negative emotions when they occur, and regulatory efforts to tolerate distress. This scale consists of 15 questions and four subscales: Emotional distress tolerance, absorption by negative emotions, cognitive appraisal of distress, and regulation of efforts to alleviate distress. The items of this scale are scored on a five-point Likert scale. Higher scores on this scale indicate higher distress tolerance (21). The scale demonstrated strong internal consistency, with a reported reliability coefficient of 0.77 (22).
3.2. Statistical Analyses
To evaluate the impact of the interventions, data analysis was conducted using SPSS Statistics, Version 27. The form of data distribution for all variables was assessed using the Kolmogorov-Smirnov test to confirm normality assumptions. Descriptive statistics, including means and standard deviations, were calculated for each variable (e.g., LTS scores, distress tolerance) at pre-test, post-test, and two-month follow-up. Repeated-measures analysis of variance (ANOVA) was employed to examine the main effects of time (within-subjects) and group (between-subjects), as well as their interaction, with a significance level set at α = 0.05. Bonferroni post-hoc tests were conducted to determine the statistical significance of mean differences between the experimental groups (CBPGT and reality therapy) and the control group, ensuring precise identification of intervention effects.
4. Results
Participants in the present study consisted of 45 male and female students with a mean age of 24.65 years. Descriptive findings, including the means and standard deviations of the pre-test, post-test, and control phases for the components of distress tolerance, separated by the CBPGT, reality therapy, and control groups, are presented in Table 3.
| Variables and Phases | CBPGT Group | Reality Therapy Group | Control Group |
|---|---|---|---|
| Emotional distress tolerance | |||
| Pre-test | 11.10 ± 1.02 | 10.90 ± 1.20 | 10.90 ± 1.37 |
| Post-test | 17.20 ± 1.50 | 17.55 ± 2.63 | 10.95 ± 1.27 |
| Follow-up | 17.00 ± 1.33 | 17.40 ± 2.39 | 10.89 ± 1.72 |
| Susceptibility to negative emotional absorption | |||
| Pre-test | 11.40 ± 1.09 | 11.20 ± 1.05 | 11.30 ± 1.92 |
| Post-test | 17.35 ± 2.30 | 17.55 ± 2.25 | 11.25 ± 1.19 |
| Follow-up | 17.85 ± 1.13 | 17.65 ± 2.22 | 11.32 ± 1.93 |
| Cognitive appraisal of distress severity | |||
| Pre-test | 10.75 ± 2.90 | 10.90 ± 1.85 | 10.80 ± 0.89 |
| Post-test | 18.15 ± 2.63 | 18.50 ± 1.58 | 10.75 ± 0.94 |
| Follow-up | 17.15 ± 2.39 | 17.60 ± 2.13 | 10.80 ± 1.43 |
| Regulatory efficacy of distress-alleviating efforts | |||
| Pre-test | 12.15 ± 1.03 | 12.40 ± 2.58 | 12.25 ± 1.25 |
| Post-test | 16.55 ± 2.35 | 16.90 ± 2.13 | 12.30 ± 1.17 |
| Follow-up | 16.60 ± 2.75 | 16.70 ± 1.14 | 12.32 ± 1.74 |
Abbreviation: CBPGT, cognitive behavioral psychodrama group therapy.
As evidenced by Table 4 and the statistically significant within-subjects effects, a significant difference was observed across the three time points (pre-test, post-test, and follow-up) for the components of distress tolerance (P = 0.001). Furthermore, the significant between-subjects effect of group indicated a significant difference in tolerance levels between the experimental and control groups (P = 0.001). The within-subjects eta-squared values demonstrated that 84%, 75%, 80%, 66%, 87%, and 61% of the within-subjects variance in emotional distress tolerance, absorption by negative emotions, cognitive appraisal of distress, and regulation of efforts to alleviate distress, respectively, were accounted for by the effects of CBPGT and reality therapy.
| Variables and Sources | SS | df | MS | F | P | ηp2 |
|---|---|---|---|---|---|---|
| Emotional distress tolerance | ||||||
| Time | 706.13 | 2 | 353.06 | 305.84 | 0.001 | 0.84 |
| Group × time | 35.93 | 4 | 87.73 | 76.00 | 0.001 | 0.72 |
| Group | 732.03 | 1 | 732.03 | 113.69 | 0.001 | 0.80 |
| Susceptibility to negative emotional absorption | ||||||
| Time | 704.21 | 2 | 352.10 | 179.70 | 0.001 | 0.75 |
| Group × time | 357.08 | 4 | 89.27 | 45.56 | 0.001 | 0.61 |
| Group | 711.34 | 1 | 711.34 | 164.31 | 0.001 | 0.85 |
| Cognitive appraisal of distress severity | ||||||
| Time | 870.87 | 2 | 435.43 | 236.79 | 0.001 | 0.80 |
| Group × time | 436.15 | 4 | 109.03 | 59.29 | 0.001 | 0.67 |
| Group | 872.74 | 1 | 872.74 | 156.27 | 0.001 | 0.84 |
| Regulatory efficacy of distress-alleviating efforts | ||||||
| Time | 350.14 | 2 | 175.07 | 114.92 | 0.001 | 0.66 |
| Group × time | 169.52 | 4 | 42.38 | 27.82 | 0.001 | 0.49 |
| Group | 345.81 | 1 | 345.81 | 65.88 | 0.001 | 0.69 |
Abbreviations: SS, sum of squares; MS, mean square.
To assess the differential effectiveness of CBPGT and reality therapy, Bonferroni post-hoc analyses were conducted following repeated-measures ANOVA. As presented in Table 3, both CBPGT and reality therapy significantly improved distress tolerance components (P = 0.001), with no statistically significant difference observed between the two interventions in enhancing distress tolerance outcomes. Similarly, Table 5 confirms comparable efficacy across groups. Thus, CBPGT and reality therapy were equally effective in improving distress tolerance among participants.
| Variables and Groups | Mean Difference | SE | P-Value |
|---|---|---|---|
| Emotional distress tolerance | |||
| CBPGT-reality therapy | -0.18 | 0.32 | 0.571 |
| CBPGT-control | 4.18 | 0.32 | 0.001 |
| Reality therapy-CBPGT | 4.36 | 0.32 | 0.001 |
| Susceptibility to negative emotional absorption | |||
| CBPGT-reality therapy | 0.06 | 0.26 | 0.802 |
| CBPGT-control | 4.25 | 0.26 | 0.001 |
| Reality therapy-CBPGT | 4.18 | 0.26 | 0.001 |
| Cognitive appraisal of distress severity | |||
| CBPGT-reality therapy | -0.23 | 0.30 | 0.553 |
| CBPGT-control | 4.55 | 0.30 | 0.001 |
| Reality therapy-CBPGT | 4.78 | 0.30 | 0.001 |
| Regulatory efficacy of distress-alleviating efforts | |||
| CBPGT-reality therapy | -0.23 | 0.30 | 0.432 |
| CBPGT - control | 2.81 | 0.30 | 0.001 |
| Reality therapy-CBPGT | 3.05 | 0.30 | 0.001 |
Abbreviation: CBPGT, cognitive behavioral psychodrama group therapy.
5. Discussion
The current study investigated the efficacy of CBPGT and reality therapy in enhancing distress tolerance among students exhibiting LTS. This study found that CBPGT and reality therapy significantly enhanced distress tolerance among university students with LTS, with no notable differences in their effectiveness. These results align with and extend prior research on therapeutic interventions for emotional distress. For instance, Davis et al. highlighted that emotional regulation difficulties following romantic breakups contribute to distress, suggesting that interventions like CBPGT and reality therapy, which target adaptive coping, are well-suited to mitigate such effects (5). Similarly, Nashtban et al. demonstrated that group-based cognitive-behavioral interventions improve distress tolerance in students, supporting CBPGT’s efficacy through its structured role-playing and cognitive restructuring components (15). Houseinzadeh et al. further reported that reality therapy enhances distress tolerance in married women, emphasizing its role in fostering personal responsibility and present-focused decision-making, consistent with our findings (19).
Reality therapy facilitates the development of emotional awareness, thereby empowering individuals to regulate negative affective states, including anxiety, depression, hopelessness, and unresolved past experiences, and subsequently enhance psychological adjustment (23). Moreover, reality therapy seeks to promote the modulation of emotional expression in response to both conscious and unconscious environmental demands (17). Consequently, reality-based psychotherapy enables individuals to exert control over the nature, timing, and mode of emotional experience and expression, as well as the duration and intensity of behavioral, experiential, and physiological aspects of emotional processes. This process aids in the prevention of psychological distress and impulsive negative affect, which can exacerbate mental health challenges, ultimately fostering positive affect, improved distress management, reduced anxiety (as a negative effect), and enhanced distress tolerance (16). Notably, individuals often employ maladaptive coping mechanisms, such as rumination, self-blame, other-blame, and catastrophizing, when confronted with stressful circumstances. In this context, reality therapy equips trained students with self-regulation strategies to mitigate over-evaluation, rumination, and negative self-talk, and to cultivate positive emotional experiences and perceptions within their personal and social interactions (24). Establishing constructive relationships founded upon positive affect promotes heightened psychological and emotional tranquility, which, in turn, contributes to increased psychological distress tolerance.
The effectiveness of CBPGT in enhancing distress tolerance among students with LTS can be attributed to its targeted approach to modifying maladaptive cognitive and emotional patterns (2). CBPGT specifically addresses distress tolerance components — such as emotional acceptance and regulation — through role-playing, a core psychodramatic technique that allows participants to externalize and reframe anxiety-inducing cognitions in a supportive group setting (14). For instance, role-playing scenarios enable participants to practice adaptive responses to distressing triggers, fostering emotional regulation and reducing avoidance behaviors (12). Additionally, CBPGT incorporates self-monitoring exercises, relaxation techniques, and cognitive restructuring to replace irrational thoughts with rational alternatives, redirecting focus from fear-based stimuli to positive ideations (25). These strategies enhance participants’ ability to tolerate aversive emotional states by promoting cognitive flexibility and emotional clarity. In contrast, reality therapy targets distress tolerance by emphasizing personal responsibility and intentional decision-making, encouraging participants to confront reality and make adaptive choices that align with their goals (17). By fostering accountability and present-focused coping, reality therapy strengthens participants’ capacity to manage distress without resorting to maladaptive strategies like rumination, complementing CBPGT’s experiential approach with a focus on behavioral control (19).
During the therapeutic intervention, participants acquire strategies to modify detrimental or intrusive thought patterns that exert deleterious effects on their behavior, thereby alleviating concerns regarding their partner's physical and psychological well-being. Furthermore, therapists facilitate the identification of problematic belief systems as a preliminary step in addressing maladaptive cognitions and behaviors. This process is crucial for understanding the interplay between thoughts, emotions, and situational contexts in the development of maladaptive behavioral responses. Session structures also emphasize the examination of overt behaviors contributing to the presenting problem. Participants engage in the acquisition and experiential application of novel skills that are transferable to real-world scenarios. Moreover, the group therapeutic context provides a supportive network, mitigating social isolation and consequently reducing anxiety and stress, ultimately fostering cognitive defusion.
5.1. Limitations
This study has notable limitations. The sample, drawn exclusively from university students in Najafabad, may introduce bias, limiting generalizability to broader populations, such as non-students or diverse cultural groups. Convenience sampling further restricts representativeness. Additionally, the study’s focus on a specific cultural context may not account for varying social norms influencing LTS expression, potentially affecting the applicability of findings elsewhere.
5.2. Conclusions
Based on these findings, university counseling programs could consider integrating both CBPGT and reality therapy as valuable options for students struggling with LTS and difficulties in tolerating distress. Offering these group therapy modalities could provide targeted support in enhancing students' emotional resilience. Future research could specifically investigate the comparative effectiveness of CBPGT against other evidence-based therapies known to improve distress tolerance, such as dialectical behavior therapy skills training groups, in this specific population. Understanding the nuances of how each approach impacts different facets of distress tolerance could further refine intervention strategies. Ultimately, this study highlights the potential of both CBPGT and reality therapy to significantly improve how students with LTS cope with emotional distress, offering promising avenues for support within university mental health services.
