


1. Background
Celiac disease (CD) is an immune system disorder that is clinically present among genetically susceptible subjects (1, 2). The soluble part of gluten, gliadin, plays a major role in the pathogenesis of this disorder and may result in villous atrophy and crypt hyperplasia (3). These mucosal alterations and immune reactions can result in a wide range of Gastrointestinal and/or other organ complications (4-6). The global prevalence of celiac disease is about 0.5 to 1.5%, while epidemiologic investigations estimate that atypical or silent and undiagnosed cases are much more prevalent than typical ones, which probably increase the real prevalence up to 6% in some community populations (7-13).
Between 80 and 90% of celiac patients remain undiagnosed. Because of late diagnosis, these patients may develop various complications, including malabsorption, anemia, bone loss, infertility, depression, or even cancer (14-18). Despite the increasing prevalence of CD and potential complications of this disorder, the only effective treatment of this condition is a lifelong commitment to a gluten-free diet (GFD) (19-21). While an effective treatment of CD necessitates a lifelong commitment to GFD, this regimen is more expensive than a normal diet and carries a social liability (22-24).
2. Objectives
we should have strong evidence to persuade not only CD patients to be committed to GFD but also health care workers, advisory teams, and social services to have more effective participation and observance. In this regard, the current study evaluated the quality of life (QOL) of CD patients after commencing GFD in the Khuzestan province of Iran.
3. Method
In a cross-sectional study, we assessed the QOL of CD patients registered in the celiac society of Khuzestan province for more than one year before the study. The CD diagnosis was based on the subject's clinical history, histological appearance of the small intestinal mucosa, and their clinical responses to the withdrawal of gluten (25). The CD cases were evaluated and compared before and at least one year after commencing GFD by using the QOL SF-36 questionnaire. During the routine clinical meeting or by phone calls, all of the participants were requested to fill a questionnaire while their personal information remained confidential. The CD patients were asked to rank their general health, as part of the SF-36 questionnaire, on a five-point scale compared to one year ago. For the quantitative estimate of the QOL parameters and calculation of a ‘transformed score’, formulae provided with the SF-36 questionnaire. The Health Survey Questionnaire Short Form 36 (SF-36) was developed in the USA for use in the Rand Corporation's Health Insurance Experiment (26). The measure has been translated into 120 languages and used around the world to gauge the health of local populations (27-29).
The inclusion criterion included a history of CD for at least one year before the study as registered in the celiac society of Khuzestan province and the exclusion criterion was the patients’ unwillingness or refusal to participate in the study. Subjects also signed a consent form before participation in the study. The rate of commitment to GFD was evaluated by comparing the serum level of CD serologic markers (anti-TTG, anti-EMA, and anti-gliadin antibodies) before and after GFD, and defined as optimal (serum level of zero or close to the lower limit of normal), sub-optimal (decreased serum level of anti-bodies but close to the upper limit of normal), and non-compliant (no decrease or even a raise in the titer). The study was approved by the Ethics Committee of Ahvaz Jundishapur University of Medical Sciences (IR.AJUMS.REC.1398.161).
The collected data were analyzed by SPSS version 19 using the t test and the chi-square test. In all the tests, P < 0.05 was considered significant.
4. Results
Overall, 200 CD patients (66 males and 134 females) were included. The average age of male and female participants was 26.3 and 30.34 years, respectively (61% between 20 and 60-years-old). Based on the serum level of serologic markers, 146 (73%) cases were defined as optimal GFD cases, and 54 (27%) patients as suboptimal ones.
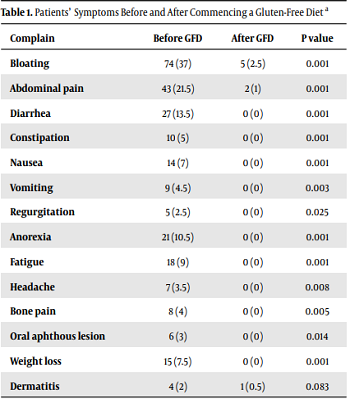
After at least one year since commencing GFD, complaints such as bloating (P = 0.001), abdominal pain (P = 0.001), diarrhea (P = 0.001), nausea (P = 0.001), vomiting (P = 0.03), reflux and regurgitation (P = 0.025), anorexia (P = 0.001), fatigue (P = 0.001), headache (P = 0.008), oral aphthous lesions (P = 0.014), weight loss (P = 0.001), and bone pain (P = 0.005) significantly improved while other symptoms such as muscular pain (P = 0.157), dermatitis (P = 0.083), and numbness (P = 0.317) did not show any major improvement (Table 1).
| Complain | Before GFD | After GFD | P value |
|---|---|---|---|
| Bloating | 74 (37) | 5 (2.5) | 0.001 |
| Abdominal pain | 43 (21.5) | 2 (1) | 0.001 |
| Diarrhea | 27 (13.5) | 0 (0) | 0.001 |
| Constipation | 10 (5) | 0 (0) | 0.001 |
| Nausea | 14 (7) | 0 (0) | 0.001 |
| Vomiting | 9 (4.5) | 0 (0) | 0.003 |
| Regurgitation | 5 (2.5) | 0 (0) | 0.025 |
| Anorexia | 21 (10.5) | 0 (0) | 0.001 |
| Fatigue | 18 (9) | 0 (0) | 0.001 |
| Headache | 7 (3.5) | 0 (0) | 0.008 |
| Bone pain | 8 (4) | 0 (0) | 0.005 |
| Oral aphthous lesion | 6 (3) | 0 (0) | 0.014 |
| Weight loss | 15 (7.5) | 0 (0) | 0.001 |
| Dermatitis | 4 (2) | 1 (0.5) | 0.083 |
Patients’ Symptoms Before and After Commencing a Gluten-Free Diet a
The average scores of QOL before and after GFD were 0.74 and 3.41, respectively, which demonstrated significant improvement (P = 0.001) (Table 2). This improvement was even seen among cases with sub-optimal compliance (average QOL score 3.28, P = 0.001).
| Parameter | Average Score Before GFD | Average Score After GFD | P Value |
|---|---|---|---|
| General health | 0.76 | 2.4 | 0.016 |
| Limitations of activities | 0.76 | 4.2 | 0.001 |
| Physical health problems | 0.59 | 3.6 | 0.003 |
| Emotional health problems | 0.88 | 5.1 | 0.001 |
| Social activities | 0.94 | 2.9 | 0.012 |
| Energy and emotions | 0.67 | 2.6 | 0.024 |
| Pain | 0.58 | 3.1 | 0.001 |
| Average | 0.74 | 3.41 | 0.001 |
The Average Scores of QOL Parameters Based on the SF-36 Questionnaire Before and After a Gluten-Free Diet
5. Discussion
In general, to quantify the degree of impairment in many chronic diseases like CD, we evaluate the quality of life parameters, but there are not enough studies that have assessed the gluten-free diet's role in the QOL of celiac patients detected by serological screening. Therefore, we examined the effect of GFD in CD patients who may ingest gluten. Despite having typical gluten-triggered lesions of the small-bowel mucosa, these patients have nonspecific, minor, or even specific symptoms. The study showed that the QOL parameters of screen-detected CD patients differed significantly before and after commencing GFD. Compared to similar studies, the number of CD patients in our study was good enough to detect a significant difference (20, 30, 31).
After one year of using GFD, three of the SF-36 parameters did not significantly differ in our subjects, compared to the last year, but other parameters improved significantly. However, the value of using a strict lifelong GFD in cases that have minor or nonspecific symptoms is still unknown (31). Also, in such patients, symptoms may manifest clinically later in their life, with malabsorption signs (32). In some subjects, even with absent gastrointestinal symptoms, the symptoms may also occur with extra-intestinal complications (33-35). Thus, the early detection of celiac disease in these cases and their treatment may help improve such complications (36).
The QOL in treated celiac patients may be affected by different factors. According to a recent report, the burden of disease in CD women using GFD for several years was worse than that in men, despite similar QOL measures (37). Another study also described how CD patients with typical symptoms of Irritable Bowel Syndrome (IBS) often report impaired QOL in all parameters and fail to obtain an optimal subjective sense of well-being, despite improvements in some QOL parameters after GFD (38). Depression and anxiety are often prevalent in CD patients. As previously described, psychological general well-being and abdominal discomfort are highly personal and subjective matters that depend on the environment and personality (39). We used validated and standardized questionnaires to assess these common features, allowing us to assess the GFD role in the QOL of CD patients (40). One of our main findings was that after the introduction of GFD, most subjects reported improved psychological well-being, which is contrary to a recent report (41). Another important finding of this study was an impressive improvement in gastrointestinal symptom scores of the CD patients. These findings are in agreement with the Mustalahti et al. report (31).
Overall, our study suggested that the QOL of patients with CD improved after one year of GFD although we could not determine whether this improvement was permanent or not. In this regard, Hallert et al. reported that after over a 10-year follow-up, CD patients failed to achieve the same level of well-being as normal people (42). Thus, our observation about the QOL improvement in CD patients may only be temporary. In our study, the overall improvement in QOL was observed after one year of commencing GFD. The limitation of this study was its design as a retrospective one.
5.1. Conclusion
In conclusion, the CD is a chronic disease with a wide range of presentations that can affect different aspects of life and influence the QOL. Our findings suggest that at least one year of a gluten-free diet is useful and may improve the QOL of CD patients even among those with suboptimal compliance. Nonetheless, more studies are needed to prove the long-term benefits or even harms of CD patients' treatment with a gluten-free diet.
