

1. Background
The COVID-19 disease is a highly contagious viral disease first noticed in Wuhan, China, and led to the outbreak of pneumonia in other regions of the world. The World Health Organization declared this disease a public health emergency in January 2020 (1, 2) and a pandemic in March 2020 (3). According to the WHO report, 574856 definitive cases of COVID-19 infection and 32953 deaths caused by COVID-19 were reported in Iran by October 27, 2020 (4). The statistics on individuals with COVID-19 is increasing quickly as the disease is easily transmitted through droplets and aerosols emerge during talking, coughing, and sneezing directly or indirectly among those not observing social distancing with keeping close contact with each other (< 6 feet). Asymptomatic patients play a critical role in this transmission process. Unfortunately, medical staff, including dentists, are more at risk for COVID-19 than other individuals in society. In the dental office environment, aerosols are produced because of rotating devices and water spray, and these aerosols then combine with saliva and blood in patients’ mouths, resulting in high contamination with bacteria, fungi, and viruses. These aerosols stay suspended in the office air for a long period or deposit on surfaces, thereby causing pathogenesis. In other words, dentists are directly or indirectly exposed to these infectious particles, and there is an increased risk of COVID-19 transmission in dental offices (1, 2, 5-11). Accordingly, designing effective infection control programs is vital to prevent the spread of the COVID-19 virus (8).
The Ministry of Health of the Islamic Republic of Iran issued guidelines on the operation of dental offices during the outbreak, which include strategies to reduce the transmission risk of the COVID-19 infection in the dental environment, and dentists are required to comply with them. Similar to international guidelines in this field, the guidelines address the use of personal protective equipment by dentists, office staff, and patients, disinfection and sterilization requirement sand methods in office environment and equipment, proper office ventilation, screening patients for COVID-19, patient appointment, social distancing, and educational brochures for patients in offices (2, 6-10).
The critical point in all the guidelines is that all clients have to be considered as infected, the infection control protocol should be observed equally for all patients, and treatments should be limited to emergency ones. Relevant knowledge of a topic can affect a person’s attitude and performance. Cagetti et al. in Italy reported the dentists’ awareness of COVID-19 in Milan, where the infection rate was higher compared to other Italian cities, to be about 71% (12). Duruk et al. concluded that only 68% of Turkey dentists were aware of COVID-19, and only 12% wore N95 Masks during the treatment procedures (10). In a previous study using a questionnaire, it was revealed that dentists’ awareness and compliance with infection control during the treatment procedures of patients with viral infections were not highly satisfactory (13-16). Moreover, dental centers with many patients or centers offering cheap dental treatment services are unwilling to implement preventive recommendations on infection control (17, 18). Non-compliance with the infection control principles, especially regarding COVID-19, is frequently observed in Iran like many countries.
2. Objectives
Implementing infection control principles is essential, and increasing dentists’ awareness is of paramount importance to promote infection control methods further. Accordingly, the present study was to evaluate the Ahvazian dentists’ awareness, understanding, and attitudes towards COVID-19 and detect the need to control the viral infection.
3. Methods
This cross-sectional study was conducted in the Oral Diseases Department of the Ahvaz jundishapur University of Medical Sciences. The statistical population encompassed all 227 Ahvazian dentist who were the WhatsApp group members of the Ahvaz General Dentists Association (227 group members out of about 507 Ahvazian dentists) to validate the content of the developed questions. This group had been created by the Ahvaz General Dentists Association, and only dentists working in Ahvaz were allowed for membership after obtaining approval from the relevant association. This WhatsApp group had a history of 10 years, via which all dentists were getting informed about the scientific and professional news on dentistry. Accordingly, the dentists who were the members of this group participated in this research. The members of the group (n = 227 (were asked for cooperation. Before sharing the questionnaire link in the group, their medical ID No. was received to ensure that they were dentists. To observe information confidentiality, the respondents were not asked to record their detailed personal information. Inclusion criteria were being a dentist and familiarity with the Persian language, and the exclusion criterion was unwillingness to participate in the study. The participants filled in the questionnaires anonymously, and no personal information was collected. The study was approved by the Ethics Committee of the Ahvaz Jundishapur University of Medical Sciences (Code: IR.AJUMS.REC.1399.427) and observed the principles outlined in the Declaration of Helsinki for human investigations. After reviewing relevant articles and international guidelines, the authors, who were members of the Iranian Association of Oral medicine, developed the questionnaire (10, 12, 15, 19, 20). The questionnaire was prepared in Persian and included questions on demographic characteristics, dentists’ knowledge, their attitudes and perceptions of COVID-19, and their practice of infection control in clinics. The questionnaire’s questions were in the multiple-choice form and were divided into several sections: dentists’ demographic characteristics, dentists’ knowledge of the incubation period, symptoms, the transmission methods of COVID-19, the COVID-19 infection control techniques, and dentists’ attitudes towards treating patients with COVID-19.
The questions and their objectives were submitted to five oral and maxillofacial specialists to confirm their validity in evaluating awareness. They were asked to score each question based on its coordination with the objectives (one for highly coordinated questions and three for low-coordinated questions). Then the questions rated two or three by the majority of experts were removed from the questionnaire. The experts confirmed its formal validity as well. Cronbach’s coefficient for 15 dentists was 0.75 after eliminating the questions decreasing reliability in evaluating the reliability of the questionnaire.
This study started on 2020.09.22 and ended on 2020.10.06. At the beginning of the study, 3712 cases of COVID-19 infection and 175 deaths caused by the COVID-19 infection were reported. The research data were collected using an online questionnaire (https://porsline.ir/ website), and the link was sent to the participants. The collected were analyzed using SPSS software version 21. Descriptive analysis was used to describe the study items. Mean and standard deviation were used to describe the continuous variables, and the percentage was used for the categorical data.
4. Results
4.1. Characteristics of Participants
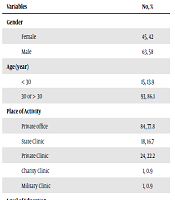
One hundred and eight dentists (45 females and 63 males) answered the questions, indicating an approximate participation rate of 63% (108 dentists out of 171 dentists who read the message). The participants in the study were 40-49 years old (34.3%), who were mainly working in private clinics (n = 84), and 62% of the participants were active. Further, 81% of the participants were general dentists, and 19% had a dental specialty. Table 1 presents the participants’ demographic characteristics. Almost 60% of the dentists had received no training on the principles of dental infection control, and 66% did not take the COVID-19 training course. Thirty-four participants (31.5%) had a person with COVID-19 in their family. The mean response time to the questionnaire by dentists was about nine minutes.
| Variables | No, % |
|---|---|
| Gender | |
| Female | 45, 42 |
| Male | 63, 58 |
| Age (y) | |
| < 30 | 15, 13.9 |
| 30 or > 30 | 93, 86.1 |
| Place of activity | |
| Private office | 84, 77.8 |
| State clinic | 18, 16.7 |
| Private clinic | 24, 22.2 |
| Charity clinic | 1, 0.9 |
| Military clinic | 1, 0.9 |
| Level of education | |
| General dentist | 87, 80.6 |
| Specialist dentist | 21, 19.4 |
Demographic Characteristics of Dentists
4.2. Knowledge of COVID-19 Incubation Period, Symptoms, and Transmission Methods
In this study, 69 (63.9%), 25 (23.1%), 8 (7.4%), and 6 (5.6%) dentists answered the questionnaire during days 1-14, 7-14, 2-7, and 7-21, respectively. In response to the incubation period of the COVID-19 disease, 9 (63.9%) dentists considered 1-14 days, and 25 (23.1%) dentists answered 7-14 days, 8 (7.4%) dentists assumed 2-7 days, and 6 (5.6%) persons reported 7-21 days. Table 2 presents the dentists’ responses to the COVID-19 symptoms. A majority of dentists reported fever (n = 105, 97.2%) and shortness of breath (n = 105, 97.2%), dry cough (n = 103, 95.4%), and the decreased sense of smell (n = 101, 93.5%) as the symptoms of the COVID-19 infection. Further, the decreased sense of taste (n = 94.87%), headache (n = 79, 73.1%), color change in tongue and oral mucosa (n = 22, 20.4%), and decreased saliva (n = 16, 14.8%) were the other symptoms in this regard. The probability of asymptomatic COVID-19 was also reported to be 77.8% (n = 84). When dentists were asked about the symptoms to be considered in diagnosing patients suspected of COVID-19, the presence of respiratory symptoms in the last two weeks was reported in 103 cases (95.4%), history of contact with suspected patients during the last two weeks was reported in 104 cases (96.3%), and travel to places with the highest disease prevalence during the last two weeks was reported in 100 cases (92.6%). Moreover, most dentists provided correct answers regarding the COVID-19 transmission methods.
| Variable | No, % |
|---|---|
| Incubation period (day) | |
| 1 - 14 | 69, 63.9 |
| 2 - 7 | 8, 7.4 |
| 7 - 14 | 25, 23.1 |
| 7 - 21 | 6, 5.6 |
| Symptoms | |
| Fever | 105, 97.2 |
| Dry coughs | 103, 95.4 |
| Shortness of breath | 105, 97.2 |
| Skin rash | 53, 49.1 |
| Diarrhea | 89, 82.4 |
| Decreased sense of smell | 101, 93.5 |
| Decreased sense of taste | 94, 87 |
| Saliva reduction | 16, 14.8 |
| Headache | 79, 73.1 |
| Problems such as tongue and oral mucosa discoloration | 22, 20 |
| Probablyasymptomatic | 84, 77.8 |
| I do not know. | 2, 1.9 |
| Transfer Method | |
| Coughing and sneezing | 107, 99.1 |
| Shaking hands and kissing | 106, 98.1 |
| Touching handles and tables | 99, 91.7 |
| Eating and drinking | 42, 38.9 |
Dentists’ Awareness of COVID-19 Infection
4.3. Knowledge About COVID-19 Transmission Methods in Dental Settings
Most of the dentists reported that frequent handwashing with soap and water or the use of alcoholic solutions (n = 105, 97.2%), wearing personal protective equipment by clinic staff (n = 102, 95.4%), regular cleaning and disinfection of surfaces (n = 104, 96.3%) should be considered as techniques to prevent the COVID-19 transmission. Almost all dentists reported that regular replacement of gloves (n = 107, 99.1%) and masks (n = 97, 89.8) is essential in preventing the COVID-19 transmission to other patients and dentists.
4.4. Perception of COVID-19
In this study, 103 (95.4%) dentists considered COVID-19 disease as a dangerous and extremely dangerous disease, four (3.7%) dentists considered it to be moderately dangerous, one person (0.9) considered it safe, and 106 (98.2%) individuals reported it a a serious challenge to the health system.
4.5. Attitudes and Practices of Dentists on COVID-19
About 88.9% of the dentists (n = 96) preferred to refrain from providing dental treatment for patients with COVID-19, and 87% (n = 94) of the dentists sent patients with cough and sneezing visiting their clinic to the hospital with no treatment, and 13% (n = 14) of the participants referred the patient to the hospital after treatment. Furthermore, 106 (98.1%) dentists believed that patients should sit down away from each other, wear masks in waiting rooms, and wash their hands before sitting on the unit. Moreover, 105 (97.2%) dentists also believed that if clinic staffs have flu-like symptoms, they are not allowed to be present in the clinic, and 8.3% (n = 9) of the dentists did not know what to do if they had the COVID-19signs and symptoms. Furthermore, 93 (86.9%) dentists had studied the protocol proposed by the Ministry of Health to reopen a dental clinic during the COVID-19 outbreak. The dentists’ practice of the basics of infection control is presented in Table 3.
| Variable | No, % |
|---|---|
| Before contacting any patient, I observe hand hygiene, including proper handwashing with soap and water or hand disinfection with alcohol-based solutions. | 97, 89.8 |
| I have learned the necessary points about COVID 19, and I ask her (him) to follow it. | 100, 92.6 |
| I wear an N95, N99, or similar for the patient before and during dental treatment procedure. | 82, 75.9 |
| I wear a regular mask for the patient before and during dental treatment procedure. | 46, 42.6 |
| I wear eye protection for the patient before and during dental treatment procedure. | 86, 79.6 |
| I wear face protection for the patient before and during dental treatment procedure. | 78, 72.2 |
| I wear a hat for the patient before and during dental treatment procedure. | 65, 60.2 |
| My assistant uses eye protection. | 59, 54.6 |
| My assistant uses an N95, N99, or similar. | 44, 40.7 |
| I refrain from eating and drinking in the examination, treatment, and waiting rooms. | 61, 56.5 |
| The surface and back cover of the unit are replaced before the next patient enters the room. | 60, 55.6 |
Dentists’ Practice Concerning COVID-19 Infection
5. Discussion
The coronavirus epidemic (COVID-19) is an emergency and a public health concern. All individuals, including dentists, are at risk for COVID-19 infection during this epidemic (21). Our results showed that a majority of the dentists in Ahvaz were aware of the COVID-19 symptoms, its transmission methods, and the infection control protocol in dental clinics; however, they had no appropriate practice of the aforementioned points. This finding is similar to those reported by Nasser et al. (21) in Lebanon, suggesting that a majority of the Lebanese dentists had satisfactory knowledge, while approximately half of the dentists had poor practice.
The present finding is also similar to a multinational study by Kamate et al. (22) and studies by Khader et al. in Jordan (15), studies by Saqlain et al. in Pakistan (23), and another study in Iran by Sarkarat (24). All these studies indicated that a relatively high proportion of dentists had appropriate knowledge of the coronavirus protection techniques. However, as the questions became more technical, the percentage of correct answers decreased (24). Although the dentists had high levels of knowledge for some questions, their awareness of some items was not satisfactory. These findings are comparable to other studies.
Dentists in our study had full knowledge of the COVID-19 symptoms, which is similar to findings reported by Khadir (15) and Sarkarat (24) on Jordanian and Iranian dentists’ knowledge of COVID-1 and in contrast with those reported by Baser (25), and Abolfotouh (26). In the present study, 89.8% of the dentists were aware of handwashing; however, in another study in Iran by Sarkarat (24), the responses to two questions on handwashing were not satisfactory. On the other hand, in our study, the dentists had different levels of knowledge about the COVID-19incubation period. The COVID-19 incubation period is estimated to vary from 5-6 days to 14 days on average (27). Our findings showed that only 23.1% of the dentists reported 7-14 days in this regard. This is similar to the findings of Khader’s study in Jordan (15). In this regard, inconsistencies in the findings of studies on awareness may be due to dentists’ lack of up-to-date information. Regarding the findings of this study and similar studies, dentists are obliged to follow preventive measures for all patients at all times (14).
The pandemic nature of COVID-19, many media and policymakers’ attention to this issue, and public education programs held via mass media by officials have increased the knowledge of all community members, including dentists, about the COVID-19 symptoms (28). Due to the critical nature of this disease and given the findings of this study and similar studies, dentists should follow and update their information about different aspects of COVID-19. Dentists’ knowledge of the main COVID-19 symptoms helps them identify threats and adopt appropriate measures in this regard, and this would play an essential role in controlling the spread of this disease (14). Individuals’ awareness about the COVID-19 incubation period is critical since it helps us determine the safe period for providing dental treatment to suspected patients. Baseer and Abolfotouh showed that dentists are less aware of the symptoms of infectious respiratory diseases compared to other health professionals; however, they need close contact and communication with patients to provide dental treatment (25, 26). In this regard, knowledge about handwashing is extremely important in controlling diseases such as MERS or COVID-19 and needs to be promoted (25).
Regarding the dentists’ perception of the COVID-19 disease, the findings showed that above 95% of the dentists considered the COVID19 disease to be highly dangerous and dangerous, and above 98% of these individuals considered it as a serious health problem. Furthermore, dentists’ perception of the dangers of this disease made about 90% of dentists be unwilling to provide treatment for the COVID-19 patients, and a majority of the dentists (98.1%) asked their patients to wear masks in the waiting room and observe social distancing. However, in Khadir’s study, 71% of the dentists considered COVID-19 a moderate risk, and about 21% did not consider it necessary for patients to sit down away from each other and wear a mask in the waiting room (15). This inconsistency of the findings might be due to differences in prevalence and mortality rates in Iran (300 persons per day on average) and Jordan (one person per day on average) (4, 15)
Although this study showed relatively high levels of knowledge, perception, and attitude towards COVID-19, the practice level was not satisfactory in some cases. For example, most of the dentists in our study considered frequent hand washing and the use of personal protective equipment as methods to prevent the COVID-19 infection transmission; however, in practice, 75.9% of the dentist and 40.7% of their assistants wore N95 or N99 Masks or similar, 79.6% of the dentists and 54.6% of their assistants wore eye protection equipment, and 72.2 % of the dentists wore face protection before and during dental treatment procedures for the patient. These findings are consistent with those of a study in Lebanon, which revealed about half of the respondents (58.7%) followed precautionary measures (21). Since appropriate knowledge of a disease can lead to more positive attitudes and more effective protection and prevention practices , and given that acceptable knowledge is essential (22), the present research, consistent with some other studies (15, 22), showed that the association among knowledge, attitude, and practice cannot be understood simply and other factors such as professional ethics, work experience, updated information sources of COVID-19, the access to or the lack of access to personal protective equipment, and others should be considered.
In our study, 86.9% of the dentists had studied the protocol issued by the Ministry of Health to reopen a dental clinic during the COVID-19 outbreak. In Lebanon (21), 73.37% of dentists used official government websites such as the WHO website as the main source of information. Not studying the protocol proposed by the Ministry of Health by several dentists in this study (13.1%) can justify the dentists’ different behaviors in dealing with suspected staffs or patients. For example, the dentists in this study had different attitudes towards patients who were coughing and sneezing. About 22.2% of the dentists did not visit the patients; however, 64.8% of the dentists without providing any treatment referred the patient to hospital after admission, and 13% of the dentists referred patients to the hospital after treatment. A few dentists (2.8%) were allowed to work in clinics based on the protocol of the Ministry of Health of Iran. Moreover, the access or lack of access to equipment can affect dentists’ practice. This finding was confirmed by Tysiac-mista and Dziedzic in Netherlands, concluding that the access to or the lack of access to personal protective equipment plays a major role in dentists’ decision to pursue their work during the coronavirus pandemic (29).
In this study, the number of males was more than the females. The heterogeneity might be attributed to the fact that there are more male dentists in Iran and Ahvaz. Although there are no reliable statistics in this regard, studies on the dentists’ community have also confirmed the number of male dentists was more than that of female dentists (24, 30, 31)
The present study had some limitations, including small sample size and limited samples in Khuzestan province. Moreover, only those who had access to the WhatsApp social network during the short data collection period had a chance to participate in the study, and they evidently had access to the COVID-19 information on this social network. However, all the dentists who had access to this social media did not complete the questionnaire, and the participation rate was 63%. These factors might have resulted in some bias in the results; hence, the findings cannot be generalized to all dentists.
5.1. Conclusions
The Ahvazian dentists are aware of the symptoms of COVID-19, its transmission, and the infection control protocol in dental clinics. However, they did not fully observed the protocols on wearing personal protective equipment for themselves and clinic staff; hence, barriers to using personal protective equipment should be eliminated, and the implementation of the protocols in dental clinics should be monitored more strictly.
