


1. Background
Chronic kidney disease (CKD) is a term used to refer to various disorders which affect the structure and function of the kidneys. The incidence of this disease is different in various parts of the world. However, the incidence of this disease in most countries is more than 200 people per million people per year (1).
End-stage renal disease (ESRD) is a severe form of CKD. Therefore, ESRD is an irreversible decrease in the physiological function of the kidney, which leads to death without dialysis or kidney transplantation (2). The causes of ESRD include diabetes, hypertension, and chronic glomerular disease (3). The average annual incidence of ESRD is 171 per million In Europe (4), while it is 336 per million in the United States (5). The incidence of ESRD in the United Kingdom is 100 per million per year (6). According to epidemiological studies, 190,000 people have ESRD worldwide, of whom 1,450,000 people undergo hemodialysis (7).
In the study conducted by Aghighi et al. in 1997, a more than 130% increase occurred in the number of ESRD patients in Iran, which indicates the importance of paying attention to this disease (8). In another study, the incidence of ESRD in Iran increased from 38.5 per million in 1998 to 49.9 in 2000 (9). Based on the results, we had more than 24,000 ESRDs in Iran in 2008, the number of which is increasing (10).
During the last two decades, the short-term and long-term survival of grafts and patients has significantly improved since the 1960s with the development of surgical techniques, new immunosuppressive drugs, especially cyclosporine, and the introduction of new anti-rejection drugs as a standard method (11). During the last three decades, it has been recommended that transplantation be exclusive between biological relatives for kidney transplantation (12), the effect of which is to improve the suppression of the immune system, drug interactions, infections, and malignancies in people receiving contraception and family planning (13). KDPI scoring system determines the kidney longevity index, which serves as a donor profile index and ranges between 0 to 100%. The factors affecting this index include high blood pressure, diabetes, ethnicity, and age in the donor (14, 15). Kidney transplantation has problems such as postoperative complications, bleeding, infection, vascular thrombosis, and urinary complications. The most common cause of death is shortly after transplantation. Re-transplantation is related to the use of more severe immunosuppressive drugs, increased infection and cardiovascular complications, along with an increased risk of death during the first three months of transplantation (15).
Also, 5 - 24% of kidney transplant patients lose their graft during the first five years of transplantation and return to the list of ESKD patients due to transplant rejection or transplant-related infections (cytomegalovirus-poliovirus infection), and re-transplantation is the best choice to improve long-term survival, as well as the quality of life among patients (16). However, this operation is associated with high risks, including high levels of antibody panel (16, 17)
In addition, some studies have shown that the two-year survival rate of a living donor in Sweden is 76% (18, 19), while the survival rate of transplants in the first, third, and fifth years in Mexico was 90%, 73%, and 65%, respectively (20).
2. Objectives
The present retrospective descriptive and analytic study was done to evaluate the survival rate of grafts between the first and second transplant recipients of Imam Khomeini Hospital in Urmia.
Examining the first and second transplants of live transplant donors and comparing the survival rate of grafts in people who have had a transplant rejection was considered as the novelty of this study. This study was performed to compare the survival rate among the recipients of the first and second transplants.
3. Methods
3.1. Setting
The present study is a retrospective and descriptive and analytical study. The inclusion criterion was all patients who had undergone the first or second transplant. All methods were performed in accordance with the relevant guidelines, regulations, and ethical standards of the responsible committee approving the research at Imam Khomeini Hospital in Urmia and the Iranian Registry of Clinical Trials and with the Declaration of Helsinki, as revised in 2000.
3.2. Participants
The statistical population included all the first and second kidney transplant patients referring to the transplant center of Imam Khomeini Hospital in Urmia who underwent surgery from 1991 to 2016.
3.3. Sample Size Calculation
We studied 245 kidney transplant patients for 25 years in Imam Khomeini Hospital in Urmia.
3.4. Study Population and Sampling Method
The study was considered as a retrospective cohort analysis. Data were collected using the checklist based on the considered variables. The necessary information was extracted from the patients' medical records by considering the patient rights. The condition of the transplanted kidney was evaluated based on the amounts of creatinine, and glomerular filtration rate (GFR), which was measured by the creatinine clearance using the following Equation, and and its unit was considered mL/min. These two factors show renal function.
The frequency of urological complications was obtained based on the information, tests, and performed measures recorded in the file. Data were analyzed by using SPSS software version 18. To report the data, the mean and standard deviation were used based on the quantity of the data, and the frequency tables and diagrams were used based on the quality of the data.
3.5. Ethical Considerations
The ethical code of the research with the ID IR.UMSU.REC.1397.103 was obtained from Urmia University of Medical Sciences. Principles of information confidentiality were observed during the research.
4. Results
First, 245 people entered the study based on the inclusion criteria, of whom 130 (53.1%) and 115 (46.9%) cases belonged to the first and second transplant recipients, respectively. The average age of the patients was 38.93 ± 13.46 years. The minimum and maximum age among the studied patients were 72 and 19 years, respectively.
In addition, in first transplant patients, 82 (63.1%) and 48 (36.9%) patients were men and women, respectively. Moreover, the number of men and women was 85 (73.9%) and 48 (26.1%) in the second transplant patients, respectively. No statistically significant difference was observed between the two groups (P = 0.069).
Evaluating the files of the studied cases indicated that 211 patients (86.1%) had normal function during the follow-up period. However, eight cases (3.3%) died in this study.
The average age of the patients was 35.90 ± 12.54 and 42.36 ± 13.70 years in the first and second transplant groups, respectively. A statistically significant difference was found between the two groups (P = 0.001) (Table 1).
| Groups | Mean ± Standard Deviation | P-Value |
|---|---|---|
| First transplant | 35.90 ± 12.54 | 0.001 |
| Second transplant | 42.36 ± 13.70 |
Evaluating the Average Age of the Patients
The survival rate of the patients was assessed based on gender. Based on the results, no significant difference was observed between the primary and secondary survival of the graft in male patients. The graft survival was 137.85 ± 4.75 and 101.51 ± 4.69 months in the first and second transplant male patients, respectively, and this difference was not statistically significant (P = 0.252) (Figure 1).

Evaluating the survival of the graft in the male patients based on the type of the transplant
The graft survival was 136.85 ± 8.52 and 59.25 ± 4.69 months for the first and second transplant female patients, respectively. This difference was statistically significant (P = 0.004) (Figure 2).

Evaluating the survival of the graft in female patients based on the type of the transplant
Graft survival of the patients was assessed based on the type of the transplantation (Figure 3). The graft survival of the first and second transplant patients was 144.23 ± 4.87 and 96.05 ± 3.55 months, respectively. The difference observed was not statistically significant (P = 0.372).

Graft survival based on the type of the transplantation
Evaluating the graft survival based on the year is given in Table 2. The graft survival was lower in the second transplantation compared to that of the first.
| Percentage of the Graft Survival | ||
|---|---|---|
| First Graft | Second Graft | |
| One year | 100 | 100 |
| Three years | 98 | 89 |
| Five years | 73 | 69 |
Percentage of the Graft Survival
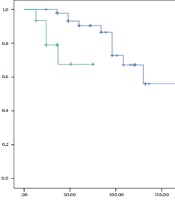
Overall survival of the patients was 128.27 ± 4.29 months (95% confidence interval: 119.86 - 136.67) (Figure 4).

Overall survival of the studied patients
The overall survival of the patients in the second transplant patients was less compared to that of the first (Table 3).
| Percentage of the Patient Survival | ||
|---|---|---|
| First Transplantation | Second Transplantation | |
| One year | 100 | 99 |
| Three years | 100 | 96 |
| Five years | 98 | 84 |
Percentage of the Patient Survival
In this study, GFR and CR of the patients in the first and second transplant groups were examined separately in the first to fifth years of transplantation. As shown in Table 4, a significant difference was observed between creatinine and GFR levels in the first and second transplants according to transplant year.
In addition, the rate of postoperative and internal complications after transplantation in the patients with first and second seizures was evaluated. The results showed that the prevalence of infectious diseases and underlying diseases was not significantly different in patients.
| Variables | Second Graft | First Graft | P-Value |
|---|---|---|---|
| Prevalence malignancy | 7 (75) | 2 (25) | 0.106 |
| Cytomegalovirus infection | 37 (50.7) | 36 (49.3) | 0.627 |
| Bacterial infection | 30 (55.6) | 24 (44.4) | 0.747 |
| Urinary infection | 67 (55.4) | 54 (44.6) | 0.474 |
| Urological complication | 13 (68.4) | 6 (31.6) | 0.051 |
| Diabetes | 46 (65.7) | 24 (34.3) | 0.01 |
| Blood pressure | 31 (50.8) | 30 (49.2) | 0.686 |
Evaluation of Underlying Disease and Postoperative and Internal Complications After Transplantation in the First and Second Grafts a
5. Discussion
A significant fraction of ESRD patients experiences dialysis and kidney transplantation at different time periods. These treatment decisions may affect the incidence and nature of the disease and mortality after the onset of ESRD (21). This study indicated a significant difference between the average age of the first and second transplant patients. Based on the results, the second transplant patients had a higher average age compared to the first, which is consistent with the results of Ingsathit et al. (22). Legendre et al. reported that many factors affected the long-term outcome of kidney transplantation, which were schematically characterized by the patient's death, renal dysfunction, and graft loss. The quality of the transplant is one of the most important factors. Other factors include the recipient's age, disease recurrence, HLA compliance, HLA immunization, recipient ethnicity, dialysis time, and cardiovascular diseases. The graft survival was not significantly different based on the first and second transplants in the present study. Moreover, the graft survival for the second transplant in the third (89%) and fifth (69%) years compared with that of the first transplant in the third (98%) and fifth (73%) years showed that it was lower in the second transplant. A significant difference was observed between the graft survival of the first and second transplants in the female patients (23). The graft survival of the first and second transplants was 136.85 ± 8.52 and 59.25 ± 4.69 months, respectively. However, the graft survival in the men was not significantly different in the first and second transplants. No significant difference was found between the survival of the patients based on the first and second transplants. The survival of the patients with the first and second transplants was 165.14 ± 4.49 and 101.34 ± 2.42 months, respectively. Based on the results, patients with the first transplant had longer survival than those with the second transplant.
All patients received the kidney from a living donor in the present study. Therefore, better results were obtained in this study compared to the study using the kidney from a corpse. This issue can play an important role in the survival of the graft and patients. Wang et al. indicated that the graft rate was 90% in the first year of the transplantation (24).
Coeman’s et al. assessed 108787 transplant recipients in the European population and indicated that improvement in graft survival from 1986 to 1999 was more pronounced in the short period than in the long period. The hazard rate at one, five and ten years post-transplant after transplantation decreased 64% (95% confidence interval, 61 - 66%), 53% (49 - 57%), and 45% (39 - 50%), respectively. The hazard rate at one, five, and ten years post-transplant declined 22% (12 - 30%), 47% (36 - 56%), and 64% (45 - 76%), respectively from 2000 to 2015 (19). Improvement in graft survival in the first five years after transplantation has been significantly less since 2000. However, improvement after five years was comparable to before. These changes were independent of the characteristics of the donor and the recipient. Short-term improvement in graft survival has decreased since 2000. However, the long-term improvement did not change in Europe (14, 19).
In the study performed by the Medin et al. in the Stockholm between January 1987 and April 1996, five-year survival was considerably better after LD-kidney transplantation (94%), then after cadaveric-kidney transplantation (76%) or on chronic dialysis (60%). Cox hazard regression analysis gave an age-adjusted relative risk for death of 0.46 for LD-transplanted and 1.49 for remaining on dialysis compared with cadaveric-transplanted patients (18).
Based on the studies, the two-year survival rate of a living donor was reported to be 76% in Sweden (18). Furthermore, the transplant survival rate in the first, third, and fifth years was 90%, 73%, and 65% in Mexico, respectively (25), which is almost consistent with the results of the present study. The one-year survival rate was reported to be 85% and 92% in Norway (25) and Australia, respectively, which is lower compared to that of the present study (26).
In this study, only the first transplant of patients was not enough, and the complications after transplantation and the study of underlying diseases were also studied.
5.1. Limitations of the Study
Due to the retrospective nature of the study and the incompleteness of the information recorded in the patients' files, 245 samples in a 25-year period were considered. Furthermore, access to patients (completion of incomplete information) was limited, and calling patients was not possible.
5.2. Conclusions
In general, the results indicated that the patients with the first transplant have longer survival than the second transplant. Further, the survival of patients in the first, third, and fifth years in the second transplant is less than in the first transplant.
However, some studies have reported that diabetes, hypertension, and cardiovascular diseases, along with advanced age, are considered as the conditions, which facilitate chronic renal failure. It is necessary for each country to obtain its local information due to racial differences, environmental factors, and different food-cultural habits in order to identify the importance of each of the risk factors.
Further, there is the possibility of transplant rejection and reduced survival rate if the underlying diseases and quality of life in people who receive their first transplant and the level of activity of the immune system is not controlled, leading to the rejection of the transplant due to high antibody levels.
The incidence of advanced kidney disease in the country can be reduced when the patients at risk are identified and treated. Due to limited resources, it is recommended to do screening for high-risk patients. Since controlling the underlying disease is the purpose of therapy with mild renal insufficiency, population studies are considered as the condition for any planning and determination of the target group for therapeutic or preventive treatment.
5.3. Suggestions
Since long-term follow-up of patients after transplantation to assess the need for multiple transplants is time-consuming, the patients who have already had a kidney transplant were evaluated retrospectively, which may have some shortcomings. In addition, due to the review of transplant patients over a period of 25 years (1991 - 2016), 245 patients were included in this study. Thus, the sample size was small for evaluation in some cases. For this purpose, the present study recommends the use of information from several centers for a more comprehensive review.
