




1. Background
Today, more than 10 million individuals worldwide suffer from brain injury annually, and brain injury remains one of the main causes of death and morbidity. In the United States, for example, brain injury is the first cause of death in individuals under 45 years and the cause of 78% of deaths in the age group of 15 - 24 years (1). Many brain injury patients are admitted to the intensive care unit (ICU) (2). Due to their critical condition, dependence on mechanical ventilation, and many limitations, such as the inability to move or communicate due to being intubated and having a low level of consciousness, these patients require complete and accurate care. Therefore, it is imperative that the ICU care-treatment team, especially nurses, provide comprehensive and humane care according to their needs and preferences (3).
However, the literature suggests that most nurses often neither know their patients and their expectations well nor check their needs correctly, and for this reason, they act on the basis of self-evaluation (4, 5). According to Yousefi et al., nurses tend to evaluate the needs of patients based on their own presuppositions, which might lead to ignoring the unique physical and mental needs of patients (6). Hajinezhad et al. also demonstrated that although nurses provide good care for patients from their own point of view, what patients perceive is that the nurses are not able to meet their expectations and needs (7). Nurses must ensure that they provide care based on what patients request, not on what they think patients want (8). Therefore, it behooves nurses to examine their care based on the experiences and views of patients so that they can be helpful in solving the concerns and limitations of their patients (4).
In this sense, patients hospitalized in the ICU have a special position. Because most of these patients do not have the ability to express their experiences and desires to the staff during their stay in the ICU due to their low level of consciousness, nor are they able to communicate with the care team due to the tracheostomy tube and this condition might persist even for several months after discharge from the ICU (9). For this reason, unfortunately, the experiences of patients hospitalized in the ICU are often obscured from the perspective of nurses and ICU personnel (10). This is despite the fact that explaining and getting to know the experiences of patients hospitalized in the ICU can be one of the most important determining factors in formulating and providing humane and holistic care according to the needs and preferences of these patients (11).
Previous studies on the explanation of ICU patients’ experiences have confirmed these patients’ understanding of the ICU environment, even with their low level of consciousness. These studies have also highlighted the importance of explaining the experiences of these patients in order to provide comprehensive and humane care according to their preferences and needs (12-14). For example, an integrated review study by Gomes and Carvalho. (2018) on patients’ experiences during hospitalization in the ICU showed that these patients, despite having a series of unrealistic experiences, perceive negative and positive realities, which can be used to improve interventions in the ICU (12). In addition, the results of Samuelson ’s study showed that 81% of their patients remember the experiences of being hospitalized in the ICU (15).
2. Objectives
Given the importance of examining the experiences of brain injury patients hospitalized in the ICU, the current study was conducted to explain the experiences of brain injury patients hospitalized in the ICU.
3. Methods
3.1. Design
The current research was a qualitative study using conventional content analysis. It was conducted between 2021 and 2022 on brain injury patients admitted to the ICU departments of Golestan Hospital in Ahvaz, Iran. Content analysis is a qualitative research method that has been widely used in nursing studies in recent years (16). Qualitative content analysis allows to interpret data subjectively but by relying on a scientific method (17). Content analysis provides the required knowledge and understanding regarding the phenomenon under study (16). In general, content analysis is classified into conventional (inductive), directed (deductive), and summative methods (18). In cases where there is insufficient prior knowledge about the phenomenon under investigation, the inductive approach is recommended (19).
3.2. Participant Recruitment
In this study, 14 brain injury patients who were discharged from the ICU were selected for interviewing using the purposive sampling method. Eligibility criteria included hospitalization in the ICU due to brain injury, full alertness and ability to conduct an interview 3 months after discharge from the ICU, and willingness to participate in the study. Participants who met the eligibility criteria were invited for an interview at least 3 months after discharge.
3.3. Data Collection
To explain participants’ experiences, unstructured in-depth, face-to-face interviews were conducted with open-ended questions. With the permission of the participants, their voices were recorded during the interview. The interviews were held in a room located in Ahvaz Golestan Hospital, Ahvaz, Iran, which had enough facilities to conduct the interview and provide the patient with comfort. The interviews started by asking the participants this question: “Can I ask you to tell me about your experiences when you were hospitalized in the ICU?”. Then, during the interview, the interviewer raised probing questions, such as “Please explain more?”, “Please give an example?”, and “How did this happen?”. At the end of each interview, the interviewer, by raising the questions such as “Is there anything else you have not said?” and “Do you think there is a question that has not been asked?”, encouraged the participant to express his/her experiences. The interviews, depending on the participants’ tolerance, lasted from 25 to 60 minutes. The interviews continued until data saturation. Data saturation in this study was obtained by interviewing 12 brain injury patients. However, to ensure data saturation, the interviews were conducted with two more participants. Moreover, due to the inadequate content of the first interview, two patients were re-interviewed. Therefore, a total of 16 interviews were conducted with 14 participants.
3.4. Data Analysis
In this study, the data were analyzed based on Graneheim and Lundman method (20). Firstly, typed interviews were reviewed several times. In the next step, the semantic units were extracted and classified as condensed meaning units. The condensed meaning units were then categorized into subcategories, and an appropriate label for each was selected. Then, the subcategories were placed into categories based on their similarities and differences. Finally, each of the obtained categories was placed into main themes that are at a high level of abstraction.
3.5. Methodological Trustworthiness
In this study, trustworthiness was ensured based on Lincoln and Guba’s criteria. Lincoln and Guba’s evaluative method for validating qualitative studies is based on the four axes of credibility, dependability, confirmability, and transferability (21). The researchers in this study were continuously involved in the process of implementing the study and allocated enough time to conduct the study and analyze the data. Additionally, all the extracted data were reviewed and validated by the research team (peer check). Any disagreement about the obtained codes was resolved through a meeting and consensus among the research team members. The collected and analyzed data were also presented to the participants, and they were asked if the narrative was accurate and if a true reflection of their experience was shown (member check). All the themes obtained were approved by the participants. Therefore, there was no change in the process of reaching themes during member checks.
4. Results
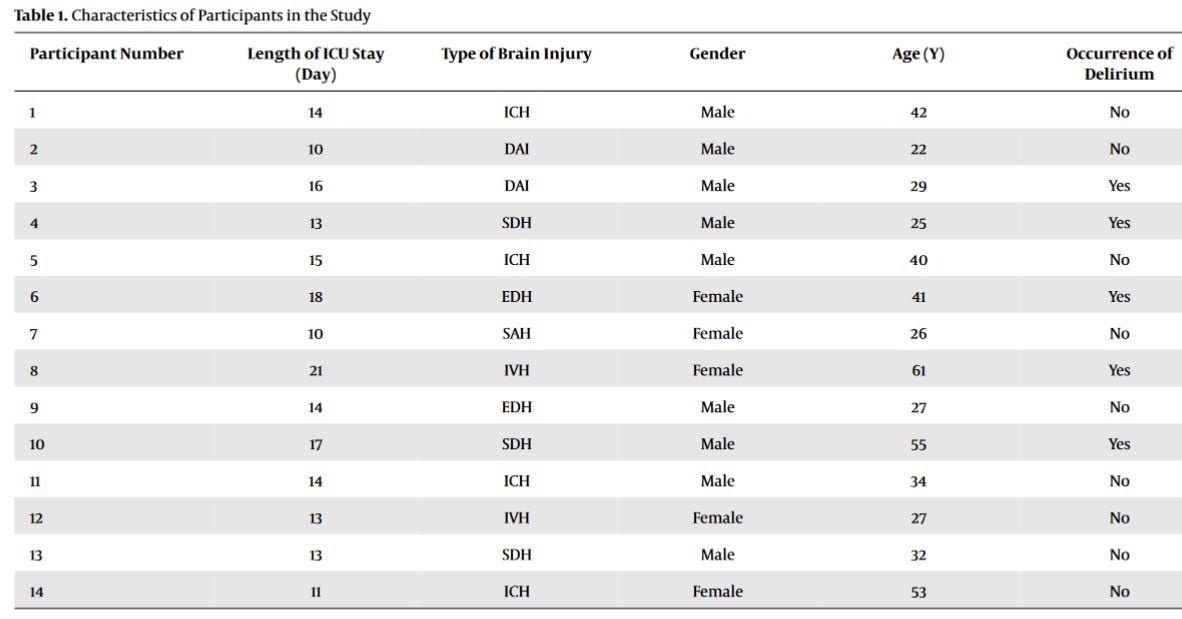
Fourteen brain injury patients who were discharged from the ICU participated in this study. The details of the participants’ characteristics are listed in Table 1.
| Participant Number | Length of ICU Stay (Day) | Type of Brain Injury | Gender | Age (Y) | Occurrence of Delirium |
|---|---|---|---|---|---|
| 1 | 14 | ICH | Male | 42 | No |
| 2 | 10 | DAI | Male | 22 | No |
| 3 | 16 | DAI | Male | 29 | Yes |
| 4 | 13 | SDH | Male | 25 | Yes |
| 5 | 15 | ICH | Male | 40 | No |
| 6 | 18 | EDH | Female | 41 | Yes |
| 7 | 10 | SAH | Female | 26 | No |
| 8 | 21 | IVH | Female | 61 | Yes |
| 9 | 14 | EDH | Male | 27 | No |
| 10 | 17 | SDH | Male | 55 | Yes |
| 11 | 14 | ICH | Male | 34 | No |
| 12 | 13 | IVH | Female | 27 | No |
| 13 | 13 | SDH | Male | 32 | No |
| 14 | 11 | ICH | Female | 53 | No |
Characteristics of Participants in the Study
Data analysis indicated 238 compact semantic units (initial codes). Based on their similarities and differences, these codes were organized into 22 subcategories, 6 categories, and 2 themes, including “the suffering body and soul” and “illumination in the dark”. More details are provided in Table 2.
| Themes | Categories | Subcategories |
|---|---|---|
| The suffering body and soul | Physical suffering | A mountain of pain |
| Inflammation of the body | ||
| Being tied up | ||
| Presence in a war zone called ICU | Adverse physical conditions of the ICU | |
| Receiving no humane care | ||
| Feeling desperate and helpless | Fear of death | |
| Feeling hopeless and lonely | ||
| Constant stress and anxiety | ||
| A feeling of lack of authority and control over the situation | ||
| Feeling vulnerable | ||
| Perceiving unreal events | ||
| Illumination in the dark | Healing physical ailments | Reduced pain and physical discomfort |
| Freedom from restrictions | ||
| Softening the ICU atmosphere | Improved physical conditions of the ICU | |
| Presence of qualified personnel | ||
| Presence of a family member: A bridge back to life | A spark in the brain | |
| Silence of pain | ||
| Arriving at the shore of tranquility | ||
| A sense of security and confidence | ||
| Increased energy and life expectancy | ||
| Dissociation from fear of death | ||
| Receiving emotional support |
Subcategories, Categories, and Themes Extracted Based on Conventional Content Analysis
4.1. The Suffering Body and Soul
This theme includes 3 categories, namely physical suffering, presence in a war zone called ICU, and feeling desperate and helpless. Most of the participants did not clearly remember some of the days when they were hospitalized in the ICU, which were mostly the early days of hospitalization (due to the low level of consciousness). However, they stated that being hospitalized in the ICU was a very unpleasant and uncomfortable experience where their body and soul went through enormous suffering for different reasons. In the following, the experiences of several patients in this area are mentioned:
4.1.1. Physical Suffering
“When I gradually got my consciousness back in the ICU, I understood more of the pain and suffering I was going through ... My lifeless body was like being tortured every day and every moment ... It was nothing but pain and suffering ... The pain of that tube that was always in my throat, the pain of all the needles and ampoules, the headaches were so severe that I thought my brain was going to explode ... I was tied to the bed with all that pain ... No, I could neither move nor scream to ask for help.” (P. 4, a 25-year-old male)
4.1.2. Presence in a War Zone Called ICU
“I used to be on the front for several years during the war ... during the operations, we did not know when it was nighttime and when it was daytime ... there was only the clatter of gunshots and shrapnel and mortar shots ... everyone was running in different directions ... Many fellas were shot and fell down ... They were rolling in their own blood and were dying, but no one could help them ... Yes, in the ICU, it was as if I had gone to the front line of the war again ... All the noise of those devices, which sounded like a volley of bullets and mortar shots, was deafening my ears... the lights were on above me day and night ... I was lying on a bed just like the wounded in the war, but this time with my hands being tied ... It was like an operation here too, no one could help anyone else.” (P. 10, a 55-year-old male)
4.1.3. Feeling Desperate and Helpless
“Most of the time, the noise of the devices above my head was my only soulmate, and there were these monotonous events and conditions that were constantly repeating ... I did not have any authority to do anything by myself ... What is more, I could not tell anyone about my pain and suffering ... In the end, I had to deal with my pain and suffering alone at the peak of despair ... Sometimes, I was so tired and helpless that I said I wish I could die and be relieved.” (P. 4, a 25-year-old male).
4.2. Illumination in the Dark
The present analysis of the experiences of the patients showed that despite the fact that they experienced a great amount of pain and suffering during their hospitalization in the ICU and often lived in difficult, bitter, and painful conditions, sometimes they experienced situations and events which seemed to them like an illumination in the dark. This, as they claimed, had relaxed the situation to some extent and reduced their physical and mental hardships and sufferings. This theme includes 3 categories, namely healing physical ailments, softening the ICU atmosphere, and the presence of a family member: A bridge back to life. In the following, the experiences of several patients in this area are mentioned:
4.2.1. Healing Physical Ailments
“Sometimes I did not know if they were giving me painkillers or what was happening!! My pain would go away for a while; this way, I could sleep comfortably without pain even if it was for an hour ... or when the tube inside my mouth (endotracheal tube) would move from one corner of my lip to another and the pressure and pain on my lips would be less ... when my thirst was quenched ... maybe you think this is nothing, but these things for me in those terrible conditions were like a light shining in all the darkness and torment I was in.” (P. 1, a 42-year-old male)
4.2.2. Softening the ICU Atmosphere
“I remember they pulled aside the curtains of the window above my head several times, I think, and as they opened the window, the sunlight, and fresh air rushed into my room ... Amid all the darkness and the smell of disinfectants, when I smelt the fresh air and felt the sunlight, I was refreshed, and it made me feel better.” (P. 6, a 41-year-old female)
4.2.3. Presence of a Family Member: A Bridge Back to Life
“I wish my daughter was always with me ... If she were always with me, I am sure I would recover much sooner and come out of that ward ... When she was with me, she would do everything she could for me ... In those moments, the glimmers of hope lit up in me, who was constantly disappointed and worried, and I felt that I could return to life.” (P. 14, a 53-year-old female)
5. Discussion
Based on the present analysis of the patients’ experiences, hospitalization in the ICU is a very grueling and uncomfortable experience for brain injury patients because their bodies and souls go through considerable pain and suffering in the ICU. This could be due to various reasons, including physical pains and discomforts, physical limitations, the unfavorable atmosphere and conditions of the ICU, and the feeling of desperation and helplessness.
The results of the present study are consistent with the results of a study by Vahedian Azimi et al., who showed that unpleasant physical experiences (e.g., the inability to communicate with others, heavy bleeding, inability to breathe, being confined to bed, sleep disturbance, and feeling thirsty) and unpleasant mental and emotional experiences (e.g., unfamiliar voices, being away from family, anxiety and fear, mental confusion, and perception of illusory and unreal events) have made patients go through a great deal of physical and mental sufferings during hospitalization in the ICU (13). The results of a meta-synthesis study by Gomes and Carvalho also showed that patients perceived many negative realities during their stay in the ICU, which caused them substantial suffering. The most important negative experiences that the patients mentioned include pain, physical limitations, lack of privacy, uncomfortable lighting, constant noise, communication problems, separation and distance from family and familiar individuals, probes and tubes connected to the patient, preconceived ideas about the ICU, fear of death, and anxiety and doubts during treatment (12).
Moreover, the results of Albanesi et al.’s study showed that patients undergoing cardiac surgery hospitalized in the ICU described the period of their hospitalization in the ICU as a difficult and uncomfortable period for reasons such as fear and worry of not waking up, physical discomforts (e.g., difficulty breathing while being connected to the ventilator), noise and crowding, not being conscious of time and having control over it, and negative emotional feelings (e.g., despair) (22). In addition, according to Tolotti et al., the most important factors that cause discomfort in tracheostomy patients hospitalized in ICU include feelings of helplessness, frustration, and anger due to the inability to use their voice to communicate, lack of awareness about the upcoming events and the treatment process, the staff being indifferent, and the feeling of living in a vacuum (23). According to the results of the present study and the results of the above-mentioned similar studies, it can be argued that pain, physical discomfort, and physical limitations, along with not receiving holistic, humane care from the ICU staff (especially nurses and doctors) and being away from the family, are the most important factors that create unpleasant and uncomfortable experiences for patients during their stay in the ICU.
Several quantitative studies have also been conducted regarding the experiences of patients hospitalized in the ICU, which have almost come up with the same results as the current study’s results and those of other qualitative studies conducted on this very topic. For example, the results of a descriptive cross-sectional study by Soh et al. showed that approximately 65.4% of the studied patients were able to recall the physical and psychological effects of their ICU experience after being discharged from the ICU. The most important unpleasant experiences of patients were reported to include five stressful experiences, namely endotracheal tube suction, pain, confinement to bed, general discomfort, dependence on the ventilator, and frequent venipunctures (24). Furthermore, the results of a descriptive-exploratory study by Alasad et al. showed that most patients could correctly remember their stay at the ICU. They also observed that in addition to physical discomfort, care providers’ ignorance of patients’ psychological and emotional problems is among their main unpleasant experiences (25).
Therefore, the results of the present study and similar studies mentioned above showed that contrary to the public opinion and even the opinion of the staff providing care and treatment, the needs and problems of patients admitted to the ICU are not merely physical and being in the ICU is a psychologically and emotionally challenging experience, which can have many negative effects on patients. However, the psychological and emotional consequences that patients admitted to the ICU might suffer are often not sufficiently addressed by the care and treatment team of this department.
Therefore, based on the current study’s analysis of the studied patients’ experiences, it can be argued that ICU patients have often been deprived of receiving humane and holistic care that takes into account all the aspects of their physical and mental needs. This runs counter to the fact that the philosophical foundation of the nursing profession is the sacrifice to help mankind, and nursing as an art is all about the creative application of science for human well-being (26). Humanism and putting humans at the center of attention is not unique to nursing; however, it does have a uniquely special value in nursing and lies at the essence of care (27). According to Watson’s theory of human caring, patient care and treatment should not be like caring for an emotionless object. In this theory, ideal care includes the simultaneous care of the soul and body of the patient (28, 29).
The present study’s findings revealed that although being hospitalized in the ICU is a very bitter and unpleasant experience for the patients, at times, things changed for them during their stay at the ICU and helped them get some relief from their physical and mental hardships and sufferings, “just like a light shining in the darkness”. According to the experiences of the current study’s patients, the most important factors contributing to this illumination in the dark include healing the physical sufferings (including reducing pain, physical discomfort, and physical limitations), softening the atmosphere and conditions of the ICU (including the improvement of the environment and equipment of the ICU and the behavior and performance of some personnel), and meeting with a family member and receiving sensory stimulation.
In line with the results of this study, Vahedian Azimi et al.’s study showed that the most important pleasant experiences recounted by patients during hospitalization in the ICU include relief from physical discomfort (e.g., the ability to communicate, sleeping comfortably, moving around in bed, receiving pain relief interventions, reduced airway secretions, and breathing) and experiences related to emotional relief (e.g., feeling safe due to the attention and presence of nurses and hearing the voice of family members) (13). In addition, Gomes and Carvalho demonstrated that the most important positive facts perceived by patients during hospitalization in the ICU are largely related to the interpersonal relationships established between the patient, the treatment team, and the family. The studied patients stated that when the treatment team took care of them with love and dedication, better feelings grew in them, and their sufferings were reduced to a minimum (12).
In Albanesi et al.’s study, patients hospitalized in the ICU of cardiac surgery likened trust in nurses to an anchor that turned fear and worry into a sense of comfort for them (22). Gaete Ortega et al. reported that the nurses’ relationship with and attention to the patients and meeting with a family member made the patients feel more comfortable during hospitalization in the ICU. Meeting with the family allows the patients to have the determination and motivation to continue living (14). Furthermore, in Tolotti et al.’s study, patients stated that family visits during ICU hospitalization and the better understanding of their needs by staff are the main factors that made patients feel comfortable (23).
In addition, Samuelson showed that 81% of their patients remembered the experiences of hospitalization in the ICU, with 71% and 59% of them recounting unpleasant and pleasant memories, respectively. The results of the aforementioned study, in line with the present study’s results, showed that based on the analysis of patients’ experiences, unpleasant and pleasant memories are opposite to each other and that pleasant experiences can moderate unpleasant ones. The categories extracted in Samuelson ’s study include physical suffering and relief of physical suffering, emotional distress and emotional well-being, perceptual distress and perceptual well-being, environmental distress and environmental comfort, and appropriate care and stressful care services (15).
To sum up, based on the results of the present study and similar studies, it can be argued that a number of factors have a very critical and decisive role in softening the impact of unpleasant memories of hospitalization in the ICU to some extent. These factors include providing care and treatment services to reduce the stress and anxiety of brain injury patients hospitalized in the ICU, performing timely and accurate interventions to reduce pain and physical discomfort, paying attention to their emotional and spiritual needs, and providing a context for family-oriented care and meeting with family members. The results of the present study showed that meeting with the family and receiving sensory stimulation from them could play a much more prominent role in this regard.
5.1. Conclusions
Due to going through enormous physical and mental suffering, the experiences of brain injury patients hospitalized in the ICU are excessively difficult and fundamentally unpleasant. Although a hefty portion of these sufferings are related to the critical conditions with which the patients struggle, the ICU care and treatment team can palliate these unpleasant experiences to some extent by paying more attention to and addressing the physical and mental needs of the patients. Therefore, the results of the present study can serve as a clinical manual to provide humane and holistic care tailored to the needs and preferences of brain injury patients hospitalized in the ICU. In the end, it is suggested that future studies use the results obtained in this study to design interventions according to the preferences, needs, and problems of patients hospitalized in the ICU.
